
Abstract
BACKGROUND: The perception of symptoms is a cornerstone in asthma management, but studies concerning this aspect provide conflicting evidence. The visual analog scale has been proposed as a useful tool for assessing perception of respiratory symptoms. The present study investigated whether visual analog scale assessment of perception of asthma symptoms was correlated to lung function or clinical features.
METHODS: This cross-sectional study enrolled 388 subjects with asthma (159 males; mean age 39.7 y). Perception of asthma symptoms was assessed by the visual analog scale; lung function was measured by spirometry. Asthma control was evaluated by the asthma control test. Anxiety and depression were evaluated on the Hospital Anxiety and Depression Scale questionnaire.
RESULTS: Asthma was well controlled in 46.6% of subjects. Asthma symptoms in the prior month were reported by 59% of subjects; asthma signs were detected in 7.2%. The visual analog scale score was moderately correlated to FEV1 (r = 0.43). Subjects with bronchial obstruction had lower visual analog scale values than those without (P < .001). A visual analog scale score of 6 was a reliable cutoff point to discriminate subjects with bronchial obstruction (area under the curve = 0.71 at receiver operating characteristic curve; odds ratio [OR] = 7.58). Reported asthma symptoms (OR = 4.83), asthma signs (OR = 8.36), and anxiety (OR = 1.14) were predictive of a visual analog scale score of <6.
CONCLUSIONS: This real-life study found that assessment of asthma symptoms by the visual analog scale might be a reliable tool in managing patients with asthma.
- asthma
- visual analog scale
- asthma symptoms
- lung function
- bronchial obstruction
Introduction
Asthma is a chronic disorder characterized by episodic and variable bronchial air flow limitation that may cause the appearance of symptoms and signs as defined by the Global Initiative for Asthma guidelines.1 Asthma control is currently considered the principal goal of management strategies; the degree of control serves to classify asthma severity. The definition of well-controlled asthma, proposed by the Global Initiative for Asthma guidelines, includes: daytime asthma symptoms not more than twice per week, no night waking, reliever use not more than twice per week, and no activity limitation in the past 4 weeks.
Most patients with asthma are managed by their general practitioner, who bases treatment decisions solely on reported symptoms and clinical examination. Typical asthma symptoms include breathlessness, chest tightness, wheezing, cough, and exercise-induced symptoms. Inaccurate perception of asthma severity often delays asthma diagnosis and treatment, worsening both morbidity and mortality.2 Precise symptom perception is an important component in appropriate self-management of asthma, since recognition of asthma severity enables the patient to make appropriate changes in activity level, to alter the physical environment, and to modify the medical regimen in a timely fashion.3 However, there may be a discrepancy between the patient's perception of asthma symptoms and objective measures of lung function.4,5 A number of tools exist to evaluate symptom perception; of these, the visual analog scale has been used successfully in several studies. The validity of the visual analog scale to assess the sensation of breathlessness has been evaluated in both experimental and clinical studies.6,7 The visual analog scale was found to be reliable in assessing symptom severity, as compared with lung function testing: bronchial air flow obstruction is the hallmark of asthma and may readily be measured by spirometry. Although FEV1 is considered the accepted standard to diagnose and manage asthma, the forced expiratory flow between 25 and 75% of vital capacity (FEF25-75%) may be a more sensitive indicator of chronic air flow obstruction in patients with mild asthma and normal FEV1.8–10
Conversely, physical signs may be inadequate for detecting bronchial obstruction with certainty, and considerable airway obstruction may be present despite a normal clinical examination.11 Further, spirometry is not regularly performed by general practitioners treating patients with asthma, as reported by the Asthma Insights and Reality Europe study12: only 29% of subjects with asthma had undergone lung function testing in the past year, and >50% of subjects with asthma had never undergone spirometry. Thus, many patients with asthma are managed without going to specialized centers and without lung function assessment.
In this context, it was first shown that visual analog scale assessment of asthma symptoms may be useful in children with asthma.13 A subsequent cross-sectional study provided evidence that visual analog scale assessment of breathlessness perception could reliably evaluate symptom severity as compared with lung function measurement in a large cohort of children with a clinical diagnosis of asthma.14 It was hypothesized that the patient's perception of asthma symptoms, expressed through a visual analog scale score, might correlate with the degree of bronchial obstruction as measured by the FEV1. The present study aimed to test this hypothesis in an adult cohort of subjects with asthma in a real-life setting.
QUICK LOOK
Current knowledge
Asthma is a chronic disorder characterized by episodic and variable bronchial air flow limitation that may cause the appearance of symptoms and signs, as defined by the Global Initiative for Asthma guidelines. Asthma control is currently considered the principal goal of management strategies; the degree of control serves to classify asthma severity.
What this paper contributes to our knowledge
In a group of out-patient subjects with asthma, a visual analog scale score for asthma symptoms of <6 reflected a 7 times greater likelihood of bronchial obstruction (eg, FEV1 <80% of predicted) than a score of ≥6. Visual analog scale scoring appeared to be a reliable tool to assess subjects' perceptions of asthma symptoms.
Methods
Subjects
This cross-sectional study enrolled 388 subjects suffering from asthma (159 males; mean age 39.7 y). They were out-patients who had been referred to an asthma or allergy clinic for specialist examination and were recruited consecutively. The examination included medical history, clinical examination, lung function testing, Hospital Anxiety and Depression Scale (HADS) and asthma control test questionnaires, and assessment of the degree of asthma control. The hospital review board approved the study procedure; written informed consent was obtained from each subject.
Study Design and Setting
The inclusion criterion was a documented asthma diagnosis, made by a pulmonary specialist or an allergist and based on a history of intermittent wheezing, breathlessness, cough, and chest tightness, in combination with reversibility to bronchodilators and/or bronchial hyper-responsiveness to methacholine. Exclusion criteria were: a history of lung disease other than asthma; coronary artery disease; congestive heart failure or cor pulmonale; recent asthma exacerbation; and the presence of acute (in the last 4 weeks) or chronic upper and/or lower respiratory infections. Subjects discontinued use of long-acting bronchodilators for 12 h before measurement of lung function.
For all subjects, the following variables were recorded: age, sex, co-presence of rhinitis, reported asthma and rhinitis symptoms in the last month, presence of asthma signs (in particular wheezing) at physical examination, FVC, FEV1, FEV1/FVC, FEF25-75%, degree of asthma control, visual analog scale, HADS, and asthma control test.
Functional Assessment
Spirometry was performed using a computer-assisted spirometer (Pulmolab 435-Spiro 235, Pulmolab, Morgan, United Kingdom; predictive values ECCS, 1993), with optoelectronic whirl flow meter. This spirometer fulfills the American Thoracic Society/European Respiratory Society standards as per the guidelines, and the test was performed as described by the European Respiratory Society.15,16
Asthma Control
Asthma control was assessed following the most recent Global Initiative for Asthma guidelines: subjects were classified as having well-controlled, partly controlled, or uncontrolled asthma.
Asthma Control Test
The asthma control test questionnaire comprised 5 questions, each with 5 possible responses, and aimed to explore the subject's perception of his/her asthma control.17 The resulting score was in the range 0–25, where 25 indicates optimal asthma control.
Rhinitis
Rhinitis was diagnosed if there was a history of typical nasal symptoms, such as itching, sneezing, watery rhinorrhoea, and nasal obstruction. If symptom occurrence was consistent with exposure to one or more sensitizing allergens, a diagnosis of allergic rhinitis was formulated.
Visual Analog Scale
The visual analog scale evaluation system comprised a 10 cm long segment, upon which the subject was asked to indicate his/her actual perception of asthma symptoms by marking a point along the segment.18 In this study, 0 corresponded to the most severe symptoms, whereas 10 corresponded to optimal symptom-free breathing. The segment was without interval markers.
HADS Questionnaire
Participants were asked to fill out the self-reported HADS.19 The HADS is a 14-item scale that generates ordinal data. Seven of the items relate to anxiety, and 7 relate to depression. Each item is rated on a 4-point scale: 0, not at all; 1, sometimes; 2, often; 3, all of the time. This gives maximum subscale scores of 21 for anxiety and 21 for depression. HADS gives clinically meaningful results when used as a psychological screening tool in clinical group comparisons and has been found to correlate with several aspects of patient disease and quality of life.20 In the validation of the questionnaire, a score of >7 in the 2 subscales has been found to discriminate non-cases from suspected cases.19
Statistical Analysis
Possible correlations between visual analog scale score and any other clinical or personal variable were assessed using non-parametric tests. In particular, differences in visual analog scale score between patients with bronchial obstruction (FEV1 < 80% of predicted value) and those without bronchial obstruction (FEV1 ≥ 80% of predicted value) were evaluated with the Mann-Whitney test.
The non-parametric Spearman rank correlation coefficient was applied to assess the degree of correlation between visual analog scale score and measurements of lung function; correlation coefficients were classified as: ≥0.8 = very strong; 0.6–0.79 = strong; 0.4–0.59 = moderate; 0.2–0.39 = weak; and <0.2 = very weak.21
A receiver operating characteristic curve, a graphical plot with values of sensitivity (reported on the y axis) and specificity (on the x axis), was applied to assess the accuracy of the visual analog scale in predicting bronchial obstruction. For each receiver operating characteristic curve, the area under the curve with the corresponding 95% CI was plotted, and the best cutoff point for visual analog scale scores, which provided both the highest sensitivity and the highest specificity, was determined.
Correlations between the visual analog scale cutoff point and other clinical variables were determined using the Fisher exact test, the chi-square test, and the Mann-Whitney test. Statistically significant variables at univariate analysis (P < .10) were fitted in a binary logistic regression model.
A 2-tailed P value of < .05 was considered significant. All statistical analyses were performed using the SPSS 20.0 (SPSS, Chicago, Illinois).
Results
The personal and clinical characteristics of the enrolled subjects are reported in Table 1; the mean age was 39.7 y, 41% of the study group were males, and approximately two thirds of subjects suffered from rhinitis. Mean lung function parameters were normal; at least one asthma symptom was reported by 59% of subjects, and asthma signs were present in 7.2% of subjects. With regard to asthma control, 13% of subjects were found to be uncontrolled, 40.4% partly controlled, and 46.6% well-controlled. The mean asthma control test value was 19.8; the visual analog scale score for breathlessness was 7.2.
Demographic and Clinical Characteristics in Subjects
A weak, although significant, positive correlation was found between visual analog scale score and percent-of-predicted FEV1/FVC (r = 0.13, P = .01). A moderately significant positive correlation was found between visual analog scale score and percent-of-predicted FEV1 (r = 0.43, P = .001) (Fig. 1A). The visual analog scale was also weakly correlated with percent-of-predicted FVC (r = 0.38, P < .001) and with percent-of-predicted FEF25-75% (r = 0.33, P < .001), as reported in Figure 1B.
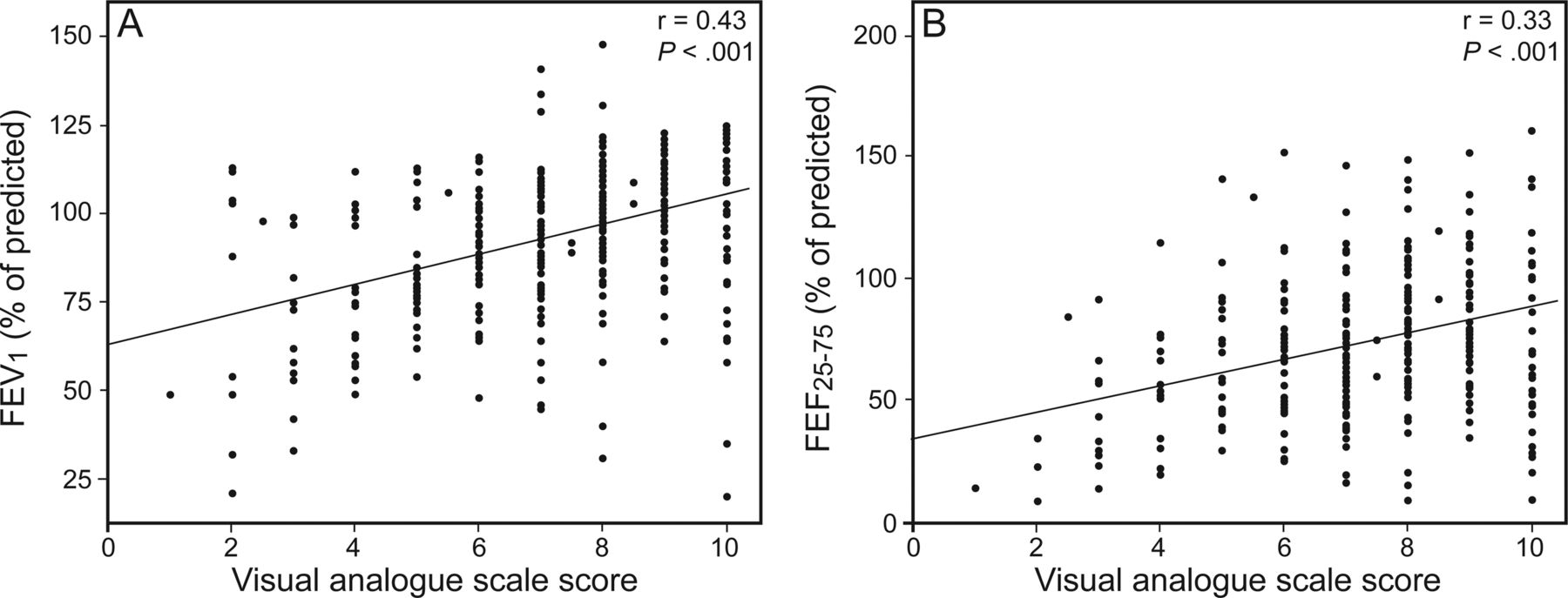
Correlation between visual analog scale score and pulmonary function.
A statistically significant difference in visual analog scale score was found between subjects with and those without bronchial obstruction (P < .001), with a lower score in the former (median 6.0, interquartile range 4.0–7.0) than in the latter (median 8.0, interquartile range 6.0–9.0) (Fig. 2).

Comparison between the median visual analogue scale scores between subjects with FEV1 values ≥80% or <80% of predicted. Boxes show interquartile range, whiskers denote ±SD, and the center lines show the median.
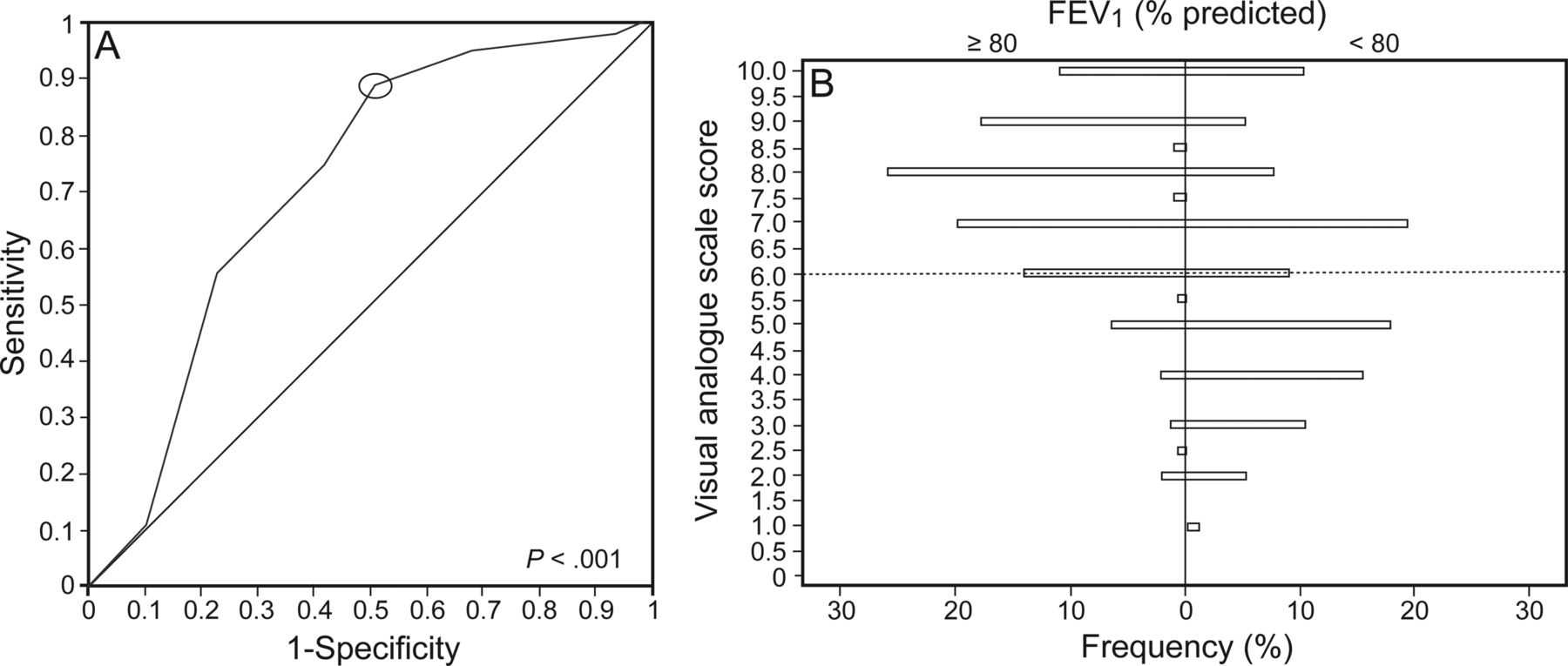
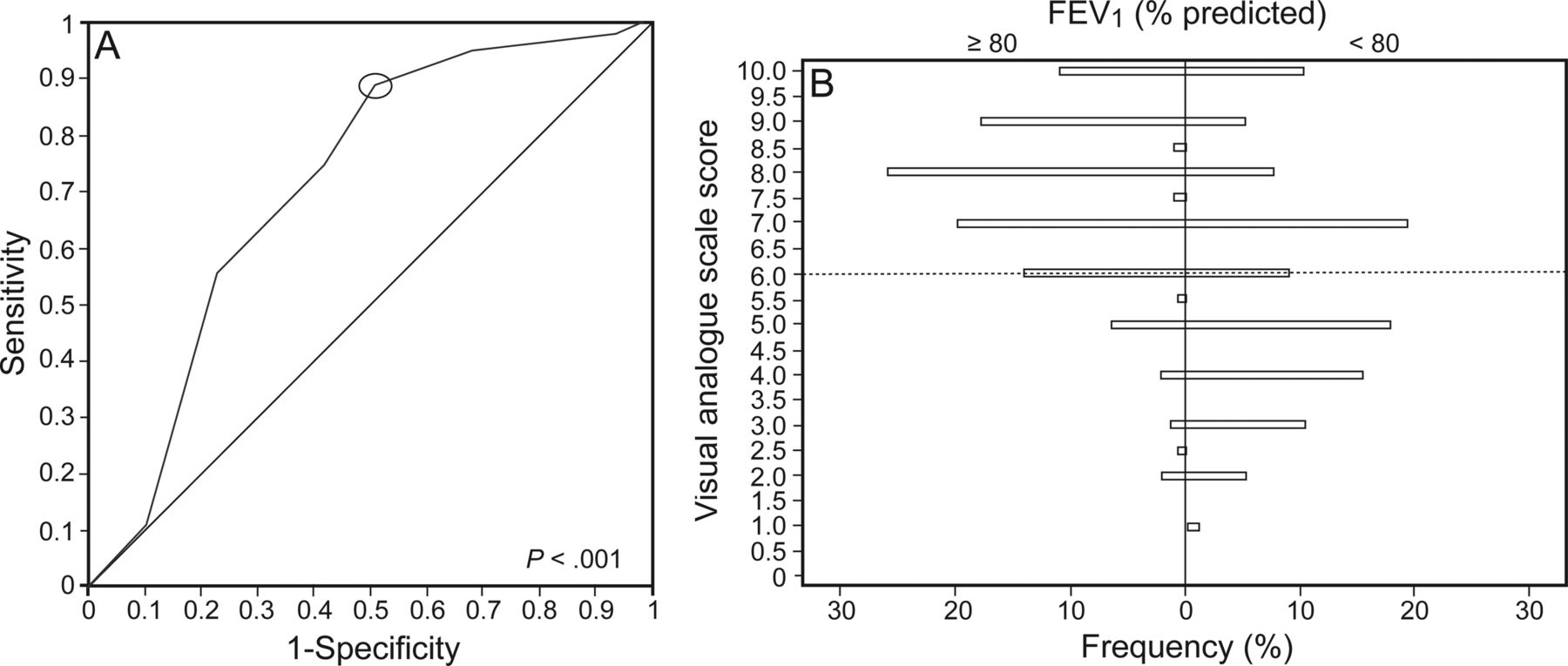
Receiver operating characteristic curve analysis revealed an optimal predictive cutoff value of the visual analog scale for detecting bronchial obstruction (ie, FEV1 < 80% of predicted). It was set at 6.0, with sensitivity 88.60%, specificity 49.37%, diagnostic accuracy 80.57%, and area under the receiver operating characteristic curve 0.71 (95% CI: 0.64–0.79) (P < .001). The positive likelihood ratio was 1.75, and the negative likelihood ratio was 0.23, with a statistically significant (P < .001) diagnostic odds ratio (OR) of 7.58 (95% CI: 4.31–13.32). In brief, this means that subjects reporting visual analog scale scores of <6 were almost 8 times more likely to have bronchial obstruction than those reporting visual analog scale scores of ≥6 (Fig. 3). Figure 3 shows the percentage frequency distribution of visual analog scale scores in subjects with and without bronchial obstruction.
{kind=link}
{kind=link}
{kind=link}
A: Optimal cutoff point (circled) at which visual analog scale score categorizes subjects with versus those without bronchial obstruction. Area under the curve = 0.71 (CI: 0.64–0.79). B: Frequency of distribution of visual analogue scale scores in subjects with and without bronchial obstruction.
Once the optimal visual analog scale score cutoff point was set at 6, the subjects were subdivided in 2 subgroups: subjects with a visual analog scale score of ≥6 and subjects with visual analog scale score of <6 (Table 2). Subjects with a visual analog scale score of <6 had all spirometric parameters significantly (P < .001 for all) lower than subjects with a visual analog scale score of ≥6; less frequently had rhinitis (P < .001); more frequently had asthma signs at clinical examination; and more frequently reported asthma symptoms in the past month than subjects with a visual analog scale score of ≥6. In addition, subjects with a visual analog scale score of <6 more frequently had uncontrolled asthma (P < .001), had lower asthma control test values (P < .001), and had higher HADS-A (HADS anxiety) and HADS-D (HADS depression) scores (P < .02 and P < .02, respectively) than subjects with a visual analog scale score of ≥6. However, mean HADS-D score was also in the normal range in subjects with a visual analog scale of <6, whereas mean HADS-A score was impaired, defined as >7, in subjects with a visual analog scale of <6.
Relationship Between Visual Analog Scale Score and Other Characteristics Assessed by Univariate and Multivariate Analysis
Considering the visual analog scale cutoff of 6, the variables found by multivariate analysis to be related to it were asthma signs and symptoms and HADS-A score. In particular, subjects with reported symptoms and subjects with asthma signs were almost 5 and 8 times more likely, respectively, to have a visual analog scale score of ≤6, compared with subjects without these characteristics (OR = 4.83, 95% CI: 1.63–14.34, P = .005; OR = 8.36, 95% CI: 2.22–31.43, P = .002, respectively). Moreover, subjects with higher values of HADS-A were more likely to have lower visual analog scale scores (OR = 1.14, 95% CI: 1.01–1.28, P = .04 (Table 2).
Discussion
Although a number of studies have examined subjects' perception of asthma symptoms, most were conducted on subjects having symptoms induced experimentally by bronchoconstriction stimuli (eg, methacholine, histamine, or exercise) or only during periods of asthma exacerbation. These studies may thus be considered to have been conducted in experimental settings. A recent study investigated the relationship between lung function and symptom perception in subjects with asthma, reporting a weak association; however, this study was conducted on a restricted cohort, and bronchial obstruction was exercise- and methacholine-induced.22 An earlier large real-life study, conducted in pediatric subjects with asthma, provided evidence that the visual analog scale score for breathlessness could predict bronchial obstruction reasonably well.14 The present study was designed to confirm those data in a large real-life population of adult subjects with asthma.
The findings show that most subjects had controlled asthma and that lung function was normal in many subjects. Most subjects perceived their symptoms as moderate. Obviously, the perception of impaired respiration mainly depends on the severity of the asthma and partially also on lung function. In this connection, there was a significant correlation between perceived respiratory symptoms and lung function, especially applying to FEV1. Subjects with bronchial obstruction, namely those with FEV1 < 80% of predicted, were found to have visual analog scale scores markedly lower than those without bronchial obstruction. A cutoff point for visual analog scale scores of 6 satisfactorily discriminated subjects with bronchial obstruction; thus, the simple assessment of asthma symptoms by the visual analog scale could offer some preliminary information concerning the bronchial air flow. This finding confirms those of the above-mentioned pediatric study.15
The present results are also consistent with findings reported by an epidemiological survey conducted on 29,518 subjects with asthma,23 which found that visual analog scale measurement of asthma severity predicted the degree of asthma control, the authors concluding that the visual analog scale score could be a simple guide in clinical situations requiring daily or regular evaluation of asthma control. The present data also suggest that the visual analog scale might be a simple predictor of lung function because there was a statistically significant correlation with both FEV1 and FEF25-75%.
It should be stressed that this study also confirms the earlier pediatric study,14 since both studies suggest that visual analog scale scores of <6 point to suspected bronchial air flow limitation. This outcome is of clinical relevance, since the simple assessment of the visual analog scale, which can be administered in any setting, may give indications of suspected bronchial obstruction.
Interestingly, subjects with higher anxiety tended to report lower visual analog scale scores. This is consistent with a recent study that found a close correlation between respiratory symptoms and psychological status, particularly anxiety.24 It is known that there is a correlation between asthma and some mental disorders, chiefly those related to anxiety and depression25,26; elevated comorbidity with anxiety and depression has been reported, and several theories have been advanced. A cognitive theory connects the long-term experience of respiratory symptoms with the generation of fear.27 Biological theories consider hypoxia and hypercapnia as factors sensitizing the neural circuits that control fear responses.28 Psychological theories emphasize the role played by stress, which affects respiration.29 The current study found that subjects with asthma with a perception of impaired breathing (ie, visual analog scale score of <6) also had above-normal anxiety scores: this is consistent with the hypothesis that anxiety may negatively affect asthma.30
In addition, subjects with low visual analog scale scores had lower asthma control test values than did those with high visual analog scale scores. This finding could reinforce the relevance of visual analog scale assessment, since well-controlled asthma is associated with the perception of good breathing; a study is ongoing to investigate this issue.
More interestingly from the clinical standpoint, the presence of asthma signs, namely wheezing, together with any asthma symptom during the past 4 weeks were relevant predictors for low visual analog scale values. This finding reinforces the concept that clinical assessment remains a cornerstone in the management of patients with asthma. Conversely, this real-life study has some limitations: few of the subjects had overt bronchial obstruction, and the study was cross-sectional. It is thus to be hoped that further studies will address these issues.
Conclusions
The principal finding of the present real-life study is that a subject with a visual analog scale score for asthma symptoms of ≤6 has a 7 times greater likelihood of bronchial obstruction (eg, FEV1 < 80% of predicted) than a subject with a visual analog scale score of >6. It may thus be concluded that visual analog scale scoring appears to be a reliable tool to assess patients' perception of asthma symptoms.
Footnotes
- Correspondence: Giorgio Ciprandi MD. E-mail gio.cip{at}libero.it.
The authors have disclosed no conflicts of interest.
- Copyright © 2016 by Daedalus Enterprises
REFERENCES
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.