

Abstract
BACKGROUND: Measurement of PCO2 is vital in determining effective alveolar ventilation. However, obtaining capillary PCO2 by a skin prick of the earlobe is painful, and nocturnal measurements disturb sleep. End-expiratory measurement of PCO2 is also well established, but there is a low precision in predicting arterial or capillary CO2. The purpose of the study was to evaluate nocturnal measurement of noninvasive, transcutaneous PCO2 (PtcCO2) measurement in hypercapnic subjects.
METHODS: In this prospective study, 31 subjects with chronic hypercapnic failure—in a stable phase of the underlying disease—and a control group of 12 healthy volunteers were included. Transcutaneous measurements were taken by the Tosca sensor (Radiometer, Copenhagen, Denmark) over a period of at least 6 h during the night. A capillary blood gas was measured at midnight and 4:00 am.
RESULTS: The mean nocturnal capillary PCO2 (PcapCO2) of subjects was 50.6 ± 10.2 mm Hg. In the 31 subjects with known hypercapnic respiratory failure, the correlation between PtcCO2 and PcapCO2 at midnight was 0.86 and at 4:00 am r = 0.80. The bias of the hypercapnic subjects was d = + 4.5 with a limit(s) of agreement of 2 SD = 13.0. The process of blood sampling caused no significant change in PtcCO2.
CONCLUSIONS: Our study evaluated transcutaneous capnography as a continuous nocturnal measurement in hypercapnic subjects. We found a good agreement between the methods. Because CO2 is not constant in patients with respiratory failure, but instead fluctuates, we would recommend the continuous transcutaneous measurement of PCO2 as our method of choice in the diagnosis of nocturnal hypercapnia.
- chronic obstructive pulmonary disease
- hypercapnic failure
- hypoventilation
- noninvasive measurement of carbon dioxide pressure
- obesity-hypoventilation syndrome
- sleep-disordered breathing
Introduction
The assessment of PCO2 is the most important parameter for evaluation of alveolar ventilation and is therefore essential in the diagnosis and treatment of hypoventilation (PCO2 > 45 mm Hg) in which alveolar ventilation is abnormally low in relation to oxygen uptake or carbon dioxide output.1 The accepted standard of measuring PCO2 is analyzing CO2 through an arterial blood gas analysis. Because obtaining a blood gas sample from an artery is an invasive and painful procedure2 with the risk of arterial lesion, this method is mostly used in the ICU or during surgery. An alternative method is measuring capillary PCO2 (PcapCO2) using blood obtained from a skin prick of the earlobe, which is a simple and less painfulness method of obtaining PCO2.3 With the exception of severe shock, capillary blood gas analysis accurately reflects arterial PCO2 (PaCO2), with earlobe sampling being slightly more accurate than fingertip sampling, as concluded by a 2007 meta-analysis.4
PCO2 can also be measured noninvasively and continuously through the end-tidal measurement of expired air (PETCO2). Its routine use is recommended in every patient with invasive ventilation during anesthesia,5 although there is low precision in predicting arterial or capillary PCO2.6–8 Nevertheless, detecting PETCO2 via a face mask is not accurate9 because of the leakage of the masks and is therefore not recommended during sleep or noninvasive ventilation.10 This also applies to the measurement of PETCO2 via a nasal cannula, which allows a qualitative analysis of ventilation and may be suitable for monitoring during anesthesia11 but does not allow a reliable qualitative calculation of PaCO2.
Measurement of PCO2 during sleep is important because respiratory mechanics change during sleep and abnormal gas exchange worsens, or may only be present during sleep, in disorders such as COPD, scoliosis, or obesity-hypoventilation syndrome.12 If PCO2 fluctuates during the night in subjects with respiratory failure (Fig. 1),13 taking only one blood sample at a random single point of the night may lead to an over- or underestimation of respiratory failure.
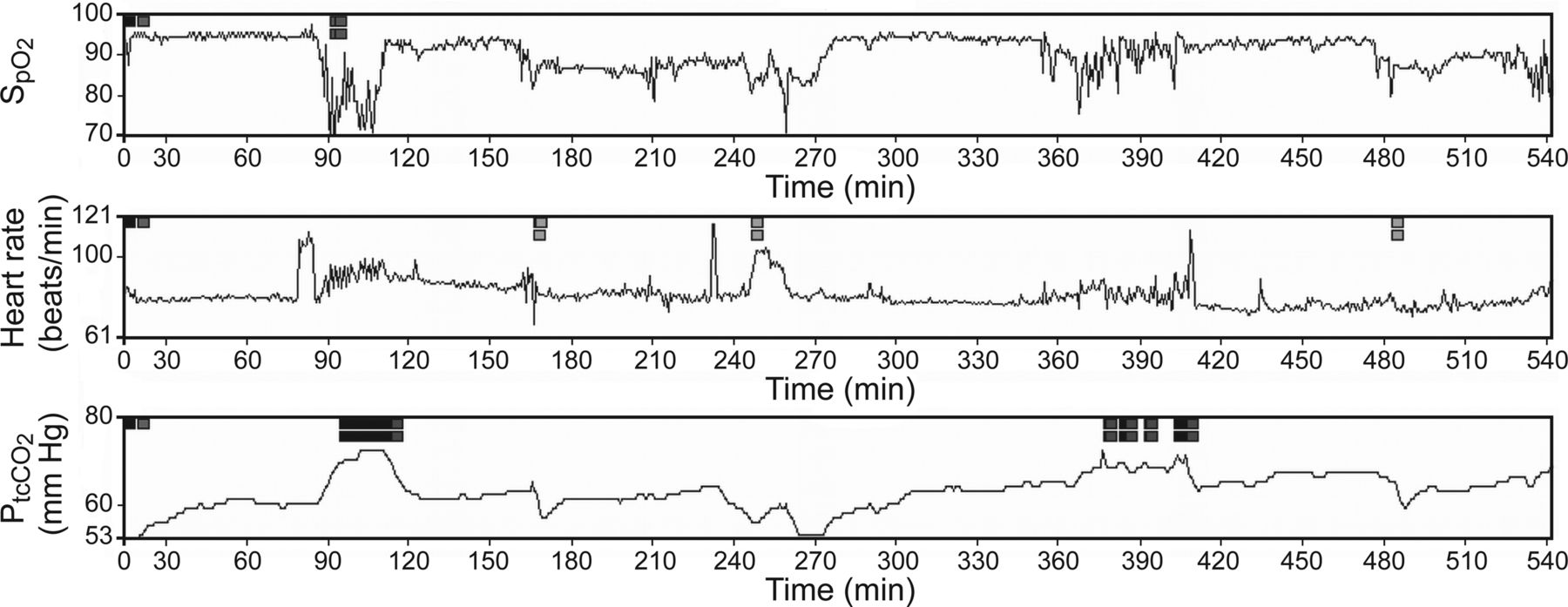
Example of long-term capnometry (9 h) with simultaneous measurement of oxygen saturation (top), heart rate (middle), and carbon dioxide (bottom) by a single Tosca earlobe electrode in a subject with intermittent nocturnal hypercapnia. Each period of hypoventilation (hypercapnia) is accompanied by desaturation and increase of the heart rate except midway through the plot, when both transcutaneous PCO2 and SpO2 drop, which is probably due to an artifact of the PCO2 measurement.
The measurement of transcutaneous PCO2 (PtcCO2) has been examined in critically ill14–16 or ventilated adults17,18 and newborns,19 as well as during bronchoscopy20 or inter-hospital ground transport. The aim of our study was to compare PtcCO2 with PcapCO2 in hypercapnic subjects during the night. Capillary instead of arterial blood gas measurement was chosen because of its impact on routine clinical practice. It was also planned to evaluate whether the process of blood sampling from the earlobe leads to a change in the blood gases because obtaining a blood sample from a sleeping subject may awaken the subject or at least disturb the subjects' breathing pattern, which could theoretically underestimate PCO2.
QUICK LOOK
Current knowledge
Monitoring arterial carbon dioxide (PaCO2) from arterial blood samples is the standard of care for evaluating the effectiveness of alveolar ventilation. Alternatives to blood gas analysis include airway carbon dioxide and transcutaneous monitoring. The former is affected by the presence of ventilation perfusion matching in the lung and cardiac output, whereas the latter is affected by tissue perfusion (cardiac output, skin temperature, and vasoconstriction).
What this paper contributes to our knowledge
In a small group of spontaneously breathing, normal and hypercapnic subjects, transcutaneous monitoring of CO2 closely tracked arterialized capillary blood CO2 at rest and during exercise. The limits of agreement between measurements were greater in hypercapnic subjects.
Methods
Subjects
We conducted a prospective study at a university-affiliated pulmonary care center. The study protocol was approved by the local ethics committee of the University of Witten/Herdecke. After giving their written informed consent, 31 subjects with either proven or suspected hypercapnia who were admitted to hospital were included in the trial (from May 2006 to August 2007). Hypercapnia was suspected on the grounds of clinical assessment in combination with either the results of a previous blood gas analysis with elevated PCO2 or by severe limitation of the lung function. Only subjects with stable disease of chronic hypercapnic failure due to obesity-hypoventilation syndrome, COPD, or thoracorestrictive diseases like scoliosis were included. Patients who needed emergency and intensive care treatment such as intubation or the application of vasoactive drugs were excluded. Exclusion criteria also included home mechanical noninvasive ventilation before study inclusion as well as lack of informed consent. To prove the accuracy of the system in chronic hypercapnic failure, there was a control group of 12 subjects with normocapnia.
Design
Measurements were made as long-term measurement during a sleep period of at least 6 h in a hospital room. Capillary blood gas analysis was performed at midnight and 4:00 am after rendering the earlobe hyperemic by a nicoboxil/nonivamide-containing cream. Blood gas analyses were performed twice because of the variation of PCO2 during sleep and served also to detect a drift of PtcCO2. Drift was defined by an increase of PtcCO2-PcapCO2 difference overnight. The samples were analyzed immediately (Ecosys II, Eschweiler, Kiel, Germany). Transcutaneous long-term monitoring of PtcCO2 by an earlobe sensor was performed during the whole night. The PtcCO2 value was taken from the CO2 monitor at the time of the blood gas analysis. To detect sample error caused by taking a blood gas sample during sleep, PtcCO2 values were additionally measured 30 min before and 30 min after the blood sample (11:30 pm, midnight, 12:30 am; 3:30 am, 4:00 am, 4:30 am).21 In addition, a 6-min walk test and a cycle ergometer exercise test were performed whenever possible.
Transcutaneous Capnometry
The tc Sensor 92 of the Tosca 500 monitor (Radiometer, Copenhagen, Denmark) offers simultaneous monitoring of PtcCO2, oxygen saturation (SO2pO2), and pulse rate by a single sensor. The Tosca uses a temperature of 42°C, which lowers the reactivity to rapid changes in PaCO2, but avoids heat damage and still shows a good correlation to PaCO2. Because heat also increases the metabolism of poorly oxygenated skin layers (anaerobic factor) by approximately 4.5%/°C, PtcCO2 is measured higher than capillary CO2.22 PtcCO2 is not measured directly but potentiometrically derived by determining the pH of the electrolyte layer separated from the skin by a highly permeable membrane and calculated by the equation of Severinghaus: PaCO2 = (tcCO2 – 5 mm Hg)/10(l0.019 × [T - 37]),23 where T is the temperature in degrees celsius and PaCO2 the estimated arterial value displayed on the screen of the monitor after temperature correction. Before starting the measurement each night, a calibration of the system was carried out. The sensor was placed at the subject's earlobe. The Tosca sensor may remain during a period of 12 h. In vivo calibration using a reference capillary blood sample was not performed.
Analysis
To evaluate changes of blood gas analysis by the sampling capillary blood, the PtcCO2 values 30 min before and after blood sampling were calculated through the analysis of variance. The drift of transcutaneous capnography was calculated by comparing the difference between PtcCO2 and PcapCO2 at midnight with the values at 4:00 am using the Wilcoxon test. PtcCO2 and PcapCO2 were correlated by linear regression, with calculation of Pearson coefficient of correlation. The bias and the agreement between the 2 different methods measuring CO2 was calculated as described by Bland and Altman.24 The bias (d) was defined as the mean difference between PtcCO2 and PcapCO2. The limits of agreement between the 2 methods are defined as d ± 2s with s being the standard deviation of d.
Results
The 12 healthy volunteers hat a normal daytime PcapCO2 at rest (36.9 ± 3.2 mm Hg) and at exercise (38.5 ± 0.8 mm Hg), as well at night (37.6 ± 6.1 mm Hg). In contrast, the 31 subjects with suspected hypercapnia showed a higher daytime PcapCO2 at rest (47.2 ± 10.0 mm Hg, P < .001) and at exercise (49.5 ± 5.4 mm Hg, P = .02), as well as at night (50.6 ± 10.2 mm Hg, P < .001) (for details, see Table 1). The main reasons for hypercapnia were COPD, obesity-hypoventilation syndrome, and thoracorestrictive diseases like scoliosis.
Anthropometric Data and Results of Different Capillary Blood Gas Analysis in Subject Groups
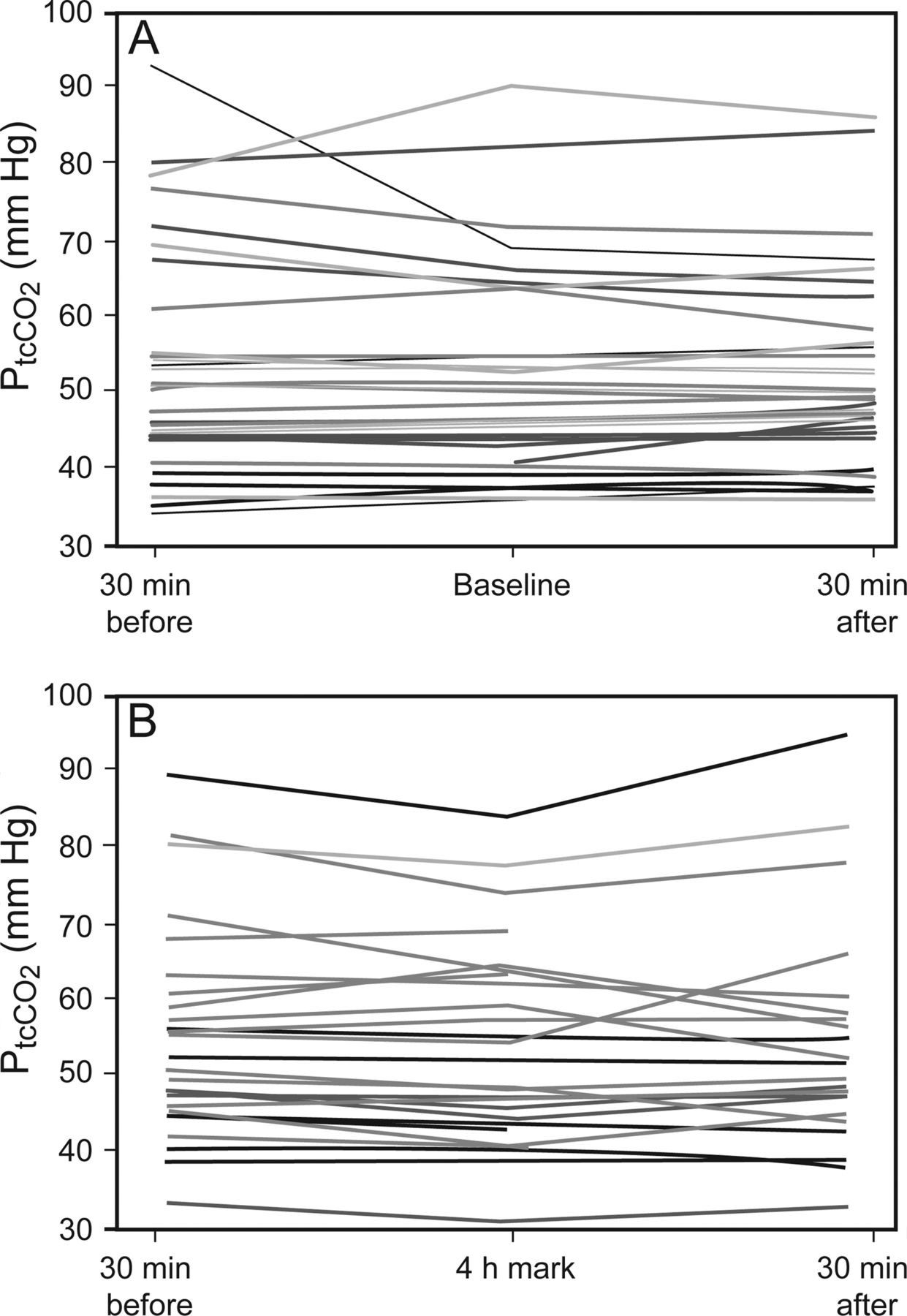
Because some blood gas analyses were not performed, only 51 of 62 possible paired measurements of PtcCO2 before/after blood gas sampling were obtained. At 30 min before/after blood gas sampling, there was no significant change of PtcCO2, indicating that there was no interference caused by blood sampling (Fig. 2, A and B).

Subjects and control group are shown together. Invasively sampling blood gas analysis did not influence the ventilation measured by the short-term trend of transcutaneous PCO2 30 min before and after initiation (A) and 30 min before and after 4:00 am (B). PtcCO2 = transcutaneous PCO2.
Furthermore, the difference between PtcCO2 and PcapCO2 did not change between midnight and 4:00 am (subjects n = 24, P = .19; volunteers n = 10, P = .20; 34 paired measurements with only 68 of 86 pairs due to missing data), indicating that there was no variation over time (drift during the night).
The correlation between PtcCO2 and PcapCO2 in the normocapnic control group at midnight was r = 0.78 and at 4:00 am r was 0.71. In the hypercapnic subjects, a total of 55 paired measurements by earlobe sensor and by capillary blood gas analysis were obtained. Considering only the 31 subjects with hypercapnia, the correlation between PtcCO2 and PcapCO2 at midnight was 0.86 and at 4:00 am r = 0.80 (Fig. 3, A and B). Summarizing subjects and control group, the correlation between PtcCO2 and PcapCO2 at midnight was r = 0.84 and at 4:00 am r was 0.84. Furthermore, the difference between PtcCO2 and PcapCO2 was constant between the different levels of CO2.

Demonstrated are the subjects with hypercapnia only. Differences between transcutaneous PCO2 and capillary PCO2 at baseline (A) show a correlation of r = 0.8615 (interception y-axis −2.03) and at 4:00 am with (B) a correlation of r = 0.8061 (interception y-axis is 11.38). PtcCO2 = transcutaneous PCO2, PcapCO2 = capillary PCO2.
Because correlation measures only relationship and not agreement between 2 methods, we calculated the bias and limits of agreement as described by Bland and Altman.24 The bias of the transcutaneous capnography of healthy controls was 4.9 mm Hg, and the limits of agreement were 8.8 mm Hg. The bias of the hypercapnic subjects was d = + 4.5 mm Hg with a limits of agreement of 13.0 mm Hg (Fig. 4).
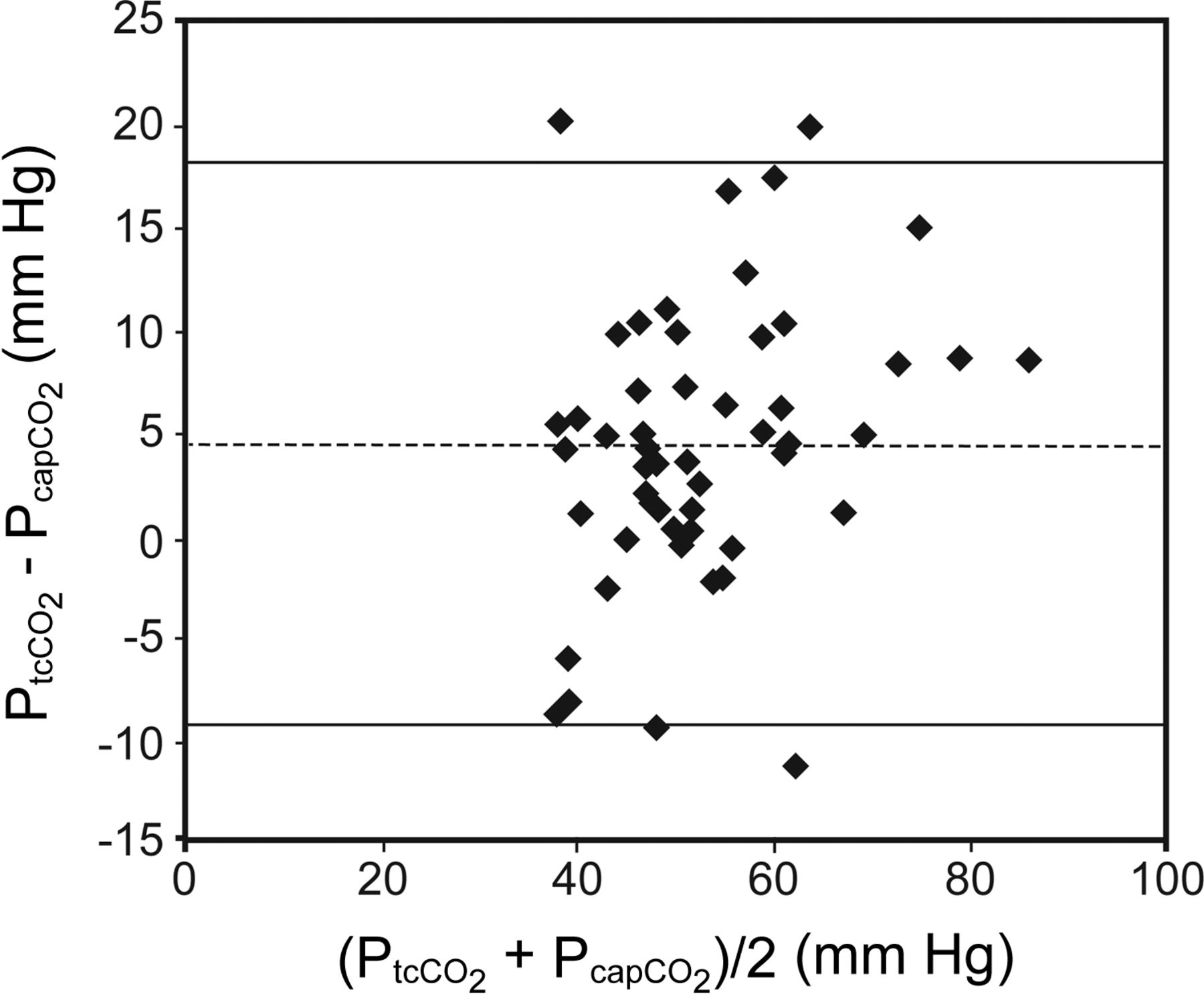
Bland-Altman plot graphing the bias and the limits of agreement on the vertical against the average of the 2 different methods on the horizontal. The plot shows the results of the hypercapnic subjects only (values of baseline and 4:00 am together). Bias and limits of agreement first of all show good accordance of transcutaneous PCO2 and capillary PCO2. The bias was d = +4.5 with a limits of agreement of 2 SD = 13. Second, the bias does not increase with increasing hypercapnia. PtcCO2 = transcutaneous PCO2, PcapCO2 = capillary PCO2.
Discussion
We evaluated the accuracy of measuring noninvasively by the Tosca sensor in hypercapnic subjects during the night. Our studies21 are the only studies to examine transcutaneous capnography via the comparison of capillary instead of arterial blood gas measurement with PtcCO2. This is important because of its impact on routine clinical practice.
We found a good but not an ideal agreement compared with capillary blood gas analysis. Theoretically, the ideal agreement should have a bias of 0. However, there will never be a bias of 0, regardless of which kind of transcutaneous monitoring system is used. The first reason is that transcutaneous PCO2 is a different parameter compared with capillary or arterial PCO2. PtcCO2 measures epidermal CO2 content and is not a direct measurement of arterial or capillary CO2. Moreover, there is additional difference between PtcCO2 and PcapCO2 caused by the CO2 production by the living epidermal cells themselves, which contributes to the capillary CO2 level at a constant amount (metabolic constant). The PtcCO2 is increased by about 4–5 mm Hg due to the metabolic rate. There is a correction algorithm used by manufactures of PtcCO2 systems as described by Severinghaus et al.25 Metabolic processes26 as well as the capillary blood flow27 of the earlobe contribute to the value that is measured transcutaneously. Both factors are highly influenced by cardiac output and general circulation.28
There is a second reason for the difference between transcutaneous and capillary PCO2 in our study population: we examined only subjects with hypercapnia during sleep. In our example (Fig. 1), PCO2 is not constant during the night in subjects with ventilatory failure. The greatest increase in PCO2 is during the REM phase of sleep because skeletal muscle hypotonia during REM includes the accessory muscles of respiration (sparing only the diaphragm). The capillary blood of the earlobe takes a while to equilibrate with the arterial CO2, so that tcCO2 has a certain delay when PCO2 is changing: one study analyzing the TCM (Radiometer, Copenhagen, Denmark) found a lag of 17 s with increasing and a lag of 78 s (90% response time) with decreasing PCO2.29 Thus, the lag of the systems explains why a bias of 0 cannot be found in subjects with rapidly changing PCO2 levels, as can be observed in subjects with hypercapnic failure during sleep.
The third important reason explaining the difference between transcutaneous and capillary PCO2 is that both analytical apparatus also have a certain error in measuring. Therefore, the error in measurement is not only caused by the transcutaneous PCO2 measurement but also by analyzing the capillary PCO2, although there is a systemic rather than a random difference between the 2 values.
Surprisingly, the agreement between PtcCO2 and PcapCO2 did not worsen with the magnitude of hypercapnia, although one could expect this due to statistical reasons: if there would be a constant deviation of, eg, 10%, then the absolute magnitude of difference would increase with increasing PCO2.
One problem with the long-term measurement of PCO2 throughout the night, as in our study, might be that the PtcCO2 could increase because of heating the skin, thereby increasing metabolism and production of CO2 (sensor temperature of the Tosca is 42°C). Occasionally a drift of PtcCO2 values was recorded, so that re-calibration of the systems during the night was required.30 In this respect, we found no significant drift throughout the night by Tosca in our study.
One of the questions answered in our study was whether disturbances by the process of sampling capillary blood in a patient during sleep could be detected. In our study, we found no statistically significant disturbances incurred by the sampling process.
Thus, we found a good but not perfect agreement between PtcCO2 and PcapCO2. What is the clinical implication? Should PtcCO2 or PcapCO2 be preferred in clinical routine to diagnose hypercapnia? In fact, accuracy of PCO2 measurement is not the same as accuracy of detecting hypercapnia, although there are only a few studies examining this issue.39 There are few studies examining the agreement of PtcCO2 and PaCO2 in patients during sleep. Sanders9 examined the accuracy of end-tidal carbon dioxide tension as well as PtcCO2 in subjects undergoing polysomnographic evaluation for suspected obstructive sleep apnea or nocturnal hypoventilation. Each subject received an indwelling arterial catheter for blood sampling during sleep. Nineteen subjects were spontaneously breathing room air, 13 received supplemental oxygen via nasal cannula, and 22 were ventilated (mostly bi-level). Only 17 subjects of the last group were analyzed regarding the transcutaneous measurement. Three different capnographs (from Novametrics Medical Systems [Wallingford, Connecticut], Radiometer [Copenhagen, Denmark], and Sensormedics Corporation [Yorba Linda, California]) were evaluated. In that study, no agreement could be found between either PETCO2 or PtcCO2 in relation to PaCO2: the average PaCO2 was elevated to approximately 50 ± 10 mm Hg, and only the capnograph of Radiometer showed a minor difference of +0.14 mm Hg. However, the error was ± 10.9 mm Hg, therefore being wide and having an off-setting scatter. Therefore, the authors concluded that there is no agreement between transcutaneous and arterial PCO2. In another study, 29 healthy volunteers21 were evaluated via Tosca. The conclusion by the authors was that the investigated systems enabled stable measurement of PtcCO2 without any drift. Nevertheless the correlation at 2 different points of time were only 0.5 and 0.72. Hanly et al31 examined transcutaneous measurement of PCO2 in 16 subjects with congestive heart failure and found that congestive heart failure subjects with daytime hypocapnia are more likely to develop Cheyne Stokes respiration during sleep. However, the subjects did not have arterial blood gas sampling at the time of sleep study. Estimation of PaCO2 was validated in 5 brain-dead subjects. In this case, they found an excellent correlation of 0.97.
Johnson et al18 evaluated PtcCO2 in a specialized weaning unit in tracheostomized subjects with prolonged weaning failure during daytime spontaneous breathing trials, the first nights off the ventilator and during bronchoscopy, and compared the results with simultaneous measurement of arterial PCO2 and PETCO2. In this study, PaCO2 was closely matched to PtcCO2 (mean ± SD difference of 0.5 ± 4.1 mm Hg). There was a greater difference between PaCO2 and PETCO2 (3.7 ± 7.7 mm Hg during prolonged exhalation, and 6.8 ± 7.2 mm Hg during tidal breathing).18
Is there any recommendation for one of the capnographs in published data relating to accuracy? Janssens et al17 overviewed different capnographs. We updated the overview and added the average PCO2 and the study population of the published studies (Table 2). The study populations are extremely heterogeneous, ranging from ventilated brain dead subjects to healthy volunteers with ergometer exercise. One must also consider that, in the different studies, not only were different capnographs analyzed, but also different blood gas analyzers, which themselves have certain variations and errors in analyzing PcapCO2 or PaCO2.
Correlation Between PtcCO2 and Arterial (Capillary) PCO2, Bias, and Limits of Agreement for Different Capnographs According to Available Published Data
Our study has some limitations that must be acknowledged. First, the number of subjects is limited. We tried to improve the sample size by measuring each subject twice. Second, we did not measure arterial PCO2 additionally. The conclusion that arterial and capillary PCO2 are equal is drawn by other studies. Finally, in method-comparison methodology, the methods to be compared need to measure the same variable, which is not the case with transcutaneous measuring of PCO2 where metabolic processes of the earlobe contribute to the value that is measured transcutaneously.40
Conclusions
Transcutaneous CO2 monitoring reliably reproduced capillary PCO2 measurements in normocapnic and hypercapnic subjects.
Acknowledgments
We thank Karin Steinraths for data collection and help in the transcutaneous measurement of PCO2. We also thank Norbert Anduleit for help in statistical analysis.
Footnotes
- Correspondence: Sven Stieglitz MD, Department of Pneumology and Cardiology, Petrus Hospital Wuppertal, Carnaper Strasse 48, 42283 Wuppertal, Germany. E-mail: sven.stieglitz{at}cellitinnen.de.
A version of this paper was presented during a poster session of the 47th Congress of the German Society of Pneumology, held——March 1, 2006, in Nürnberg, Germany.
The authors have disclosed no conflicts of interest.
- Copyright © 2016 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}