

Abstract
Because of the progressive muscle weakness they experience, patients with Duchenne muscular dystrophy frequently utilize positive-pressure devices to maintain adequate bronchial hygiene and ventilation. This case illustrates the course of a 19-y-old male who presented with a perforated right tympanic membrane (TM) following the use of these devices. Perforation of the TM while utilizing positive-pressure devices is a rarely reported event. A challenging aspect in this case was balancing the reduction of pressures and maintaining adequate ventilation while at the same time allowing the TM to heal.
- positive-pressure ventilation
- perforated tympanic membrane
- myringorupture
- insufflator-exsufflator
- noninvasive ventilation
Introduction
Because of the progressive muscle weakness that patients with degenerative neuromuscular diseases experience, positive-pressure devices are frequently utilized to maintain adequate bronchial hygiene and support ventilation. When used properly, these devices can improve quality of life and survival.1–5 In their review, Toussaint et al1 noted that patients with Duchenne muscular dystrophy (DMD) considered home mechanical ventilation to be beneficial for independent living and enhancing their overall health and quality of life, whereas health-related quality of life further decreased without mechanical ventilation. In their report, Kohler et al4 concluded that patients with DMD perceive a high health-related quality of life independent of the degree of their physical disability, respiratory impairment, and dependence on noninvasive ventilation (NIV). Although quality of life is a good indicator for patients with DMD, a more important facet is the improvement in survival. Research performed by Ishikawa et al5 noted a significant increase in the 50% survival age of patients using NIV and mechanically assisted cough devices (MACD) compared with those not using them. However, these devices can be responsible for unforeseen consequences that present unique challenges to the medical team. We describe a patient with DMD who experienced a perforated tympanic membrane (TM) during the course of his home-care regimen using positive-pressure devices.
Case Report
During a routine follow-up clinic visit with a pulmonologist, a 19-y-old male with DMD reported that while using an MACD at 35–40 cm H2O, he experienced a loud pop in his right ear. He also noted that while using NIV at night, he experienced a dull pain in his right ear and a whistling noise that kept him awake. The patient was unable to determine a specific time when the incident occurred but stated that it occurred within the last few weeks. The physical examination revealed him to be in no distress and resting comfortably in a chair. He was afebrile with a resting heart rate of 89 beats/min, a breathing frequency of 18 breaths/min, a blood pressure of 123/68 mm Hg, and an SpO2 of 97% on room air. Breath sounds were suppressed bilaterally, no crackles or wheezes were noted, and respiratory effort appeared unlabored. Heart auscultation revealed a regular rhythm without murmur. Examination of his head, eyes, nose, and throat revealed only some nasal turbinate edema with minimal drainage. The extremities were negative for clubbing or edema. Capillary refill was brisk, and nail beds were pink. He was negative for any significant scoliosis or kyphosis. Capillary blood gas (CBG) revealed a pH of 7.42, PCO2 of 48.2 mm Hg, HCO3− at 30.9 mmol/L, and a base excess of 6 mmol/L (Table 1).
Timeline of Ventilator Changes Before and in Response to the Patient's Perforated TM and Subsequent CBG Results With Proceeding Increase in PCO2 Levels
The respiratory home-care regimen to maintain cardiopulmonary stability included supplemental oxygen used only as needed, a pulse oximeter to monitor SpO2 levels, a home-care ventilator (LTV 950, Pulmonetic Systems, Colton, California) used during sleep, a suction machine to assist in clearing airway secretions, and an MACD (Emerson CoughAssist mechanical insufflator-exsufflator, Philips Respironics, Murrysville, Pennsylvania) for lung expansion exercises and to assist ineffective and weak cough.
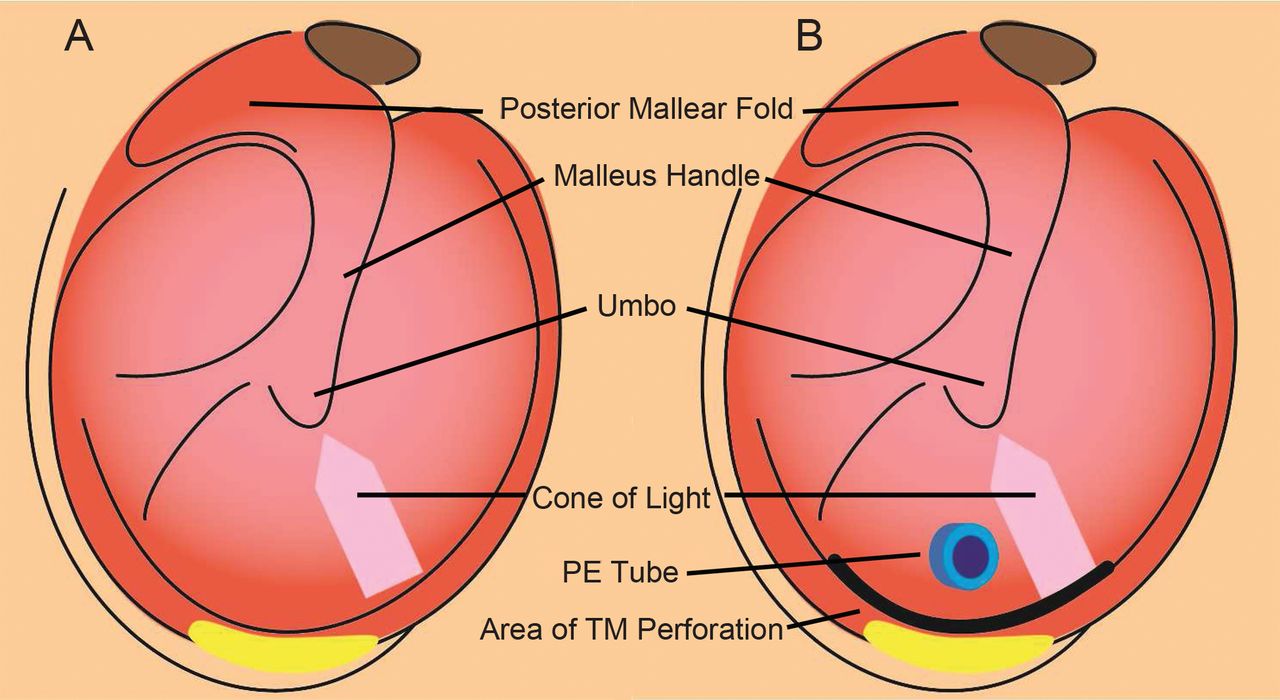
To further investigate the right ear complaint, the patient was placed on NIV for assessment. His home-care ventilator was used with his home regimen settings: assist control/pressure control mode, breathing frequency of 17 breaths/min, pressure control of 20 cm H2O, PEEP of 6 cm H2O, and inspiratory time of 1.2 s. A full face mask (PerformaTrak, Philips Respironics) was used. These settings resulted in an expired tidal volume of 5 mL/kg (total volume of 410 mL) and a mean airway pressure of 10 cm H2O. Following placement on the ventilator, repeat CBG was obtained with a reduction in PCO2 from 48 to 43 mm Hg, whereas the pH and HCO3− remained essentially unchanged. During this evaluation, with a pressure control of 20 cm H2O, air could be heard escaping from the right ear. During visual examination, the TM was noted to be moving in a flutter-like presentation. He had a pressure equalization (PE) tube in place that could be visualized (Fig. 1). It was clear that air was escaping through a perforation at the base of the right TM. The left TM was noted to be normal. According to the caregiver, the patient had bilateral PE tubes placed when he was a baby, but a specific timeline could not be established. In an attempt to minimize the air flow through the TM, pressure control was reduced from 20 to 18 cm H2O. The patient felt that the ventilator was giving him an appropriate volume. The fluctuations of the right TM could still be appreciated, and he felt discomfort in the right ear. Pressure control was further reduced to 16 cm H2O, and he became asymptomatic with regard to any ear problems.

A: Illustration depicting a normal tympanic membrane (TM). B: Illustration depicting the perforation at the base of the TM upon visual examination of the ear during the initial clinic visit. The perforation caused the TM to flutter during positive-pressure ventilation.
The patient was discharged from the out-patient clinic on the following ventilator settings: breathing frequency of 17 breaths/min, pressure control of 16 cm H2O, PEEP of 6 cm H2O, and inspiratory time of 1.2 s. MACD pressures were also lowered to a maximal setting of 30 cm H2O, a reduction from his previous home-care regimen of 35–40 cm H2O. An appointment was made with an ear, nose, and throat (ENT) specialist for evaluation and to determine a strategy for correction of the right TM perforation.
Three days after the initial clinic visit, the ENT specialist removed the PE tube. No other interventions were performed. It was expected the TM would heal in time. After several days, the patient still noted air escaping from his right ear. There was concern that the positive-pressure devices would not allow the perforation to heal, even with the reduction of pressures. To address this concern, the patient was to remain off NIV for the following 3 d and to use only the MACD as needed and not on a regular basis. The patient's SpO2 was closely monitored during this time period. A follow-up appointment was made with the ENT specialist 1 month after the removal of the PE tube.
Seventeen days after the initial clinic visit, the patient reported using NIV 3 times per week. He also stated that he did not hear air leaking though his ear, and he had no complaint of ear pain or discomfort. He used the MACD once daily to relieve congestion. He was instructed to continue the current regimen and to get a repeat CBG the following week. Additionally, no changes in pressures or frequency of use were to be initiated until the CBG results were obtained and the status of the TM could be assessed by the ENT specialist. Twenty-three days after the initial clinic visit, CBG revealed a pH of 7.38, PCO2 of 54.0 mm Hg, HCO3− at 32.5 mmol/L, and a base excess of 7 mmol/L. One month after the initial clinic visit, the ENT specialist stated that the TM had completely healed and that changes in pressures and frequency of use of NIV and the MACD could be considered. It was decided that no changes would be made until the patient could be seen in the clinic by the pulmonologist 2 weeks later.
The patient was seen for a follow-up clinic visit 51 d after the initial clinic visit. Pressure control during NIV was increased from 16 to 20 cm H2O. CBG revealed a pH of 7.4, PCO2 of 54 mm Hg, HCO3− at 33.4 mmol/L, and a base excess of 9 mmol/L. He was to increase his use of NIV to every night and to continue with the MACD at pressures of 30/30 cm H2O. Approximately 1 week later, he was tolerating the increased pressure with NIV. However, he had increased sinus drainage and increased coughing. He required the MACD 3 times daily to mobilize secretions and noted that, after these sessions, his ear made bubbling noises. It was recommended he be evaluated by the ENT specialist again and, if possible, to have his ear examined while the ventilator was in use.
Five months after the initial clinic visit, the patient was seen by the pulmonologist. NIV settings were: assist control/pressure control mode, breathing frequency of 17 breaths/min, pressure control of 20 cm H2O, PEEP of 6 cm H2O, and inspiratory time of 1.4 s. These settings resulted in an expired tidal volume of 5 mL/kg (total volume of 425 mL) and a mean airway pressure of 11 cm H2O. CBG revealed a pH of 7.4, PCO2 of 58.9 mm Hg, HCO3− at 36.3 mmol/L, and a base excess of 11 mmol/L. It was noted that the TM was still leaking. No changes were made, and the patient was to return to the clinic 2 months later. At that clinic visit, no changes were noted in NIV or MACD settings, and a repeat CBG revealed a pH of 7.39, PCO2 of 61.6 mm Hg, HCO3− at 36.9 mmol/L, and a base excess of 12 mmol/L. He was also seen by the ENT specialist at that time. His TM was still leaking air, but the ENT specialist was optimistic that it would heal.
Eight months after the initial clinic visit, the patient collapsed at work. He was noted by co-workers to be cyanotic, with no pulse or respiration. Cardiopulmonary resuscitation was performed, and he became awake and alert. He was taken to the local emergency department and examined. Chest x-ray, electrocardiogram, and blood gas were obtained, and all were within normal limits. It was suggested that the patient be admitted for observation, but he refused. He was subsequently discharged from the emergency department. Approximately 9 months after the initial report of TM perforation, he was again seen by the pulmonologist. At this point, it was determined that the TM was no longer leaking. Pressure control during NIV was increased from 22 to 25 cm H2O, resulting in an exhaled tidal volume of 7 mL/kg (total volume of 600 mL) in an attempt to improve his ventilatory status and to normalize PCO2 levels. He was lost to follow-up, and confirmation of improving PCO2 levels was not verified.
Discussion
Perforated TM associated with positive-pressure ventilation has rarely been reported in the medical literature. A literature search in PubMed utilizing the search terms positive-pressure ventilation, perforated TM, myringorupture, insufflator-exsufflator, and NIV in various combinations revealed only one reported occurrence.6 Studies to determine the pressures needed to perforate TMs have been carried out on subjects postmortem. One study noted that pressures required to perforate TMs ranged from 984 to 2,320 cm H2O (mean of 1,758 cm H2O) on 30 cadaver TMs, with the observations made between 2 and 14.5 h postmortem.7 Another study of cadaver subjects with normal TMs (n = 144) noted that perforation pressures ranged from 700 to 2,300 cm H2O (median of 1,300 cm H2O), while for TMs with atrophic scars (n = 23), perforation pressures ranged from 300 to 800 cm H2O (median of 600 cm H2O), with the observations made between 7 and 112 h postmortem.8 Another study on blast injuries noted that auditory injury happened at the lowest blast overpressure of 357 cm H2O.9 This is in close agreement with the pressures noted in perforating TMs with atrophic scars.
In this patient, there was no documentation of any type of TM injury that would have contributed to the perforation. Additionally, the PE tube should have served as a pressure relief device to prevent TM perforation. This did not occur. The opening in the TM made by the insertion of the PE tube could actually increase the risk of a perforation-type injury due to atrophic scarring, as noted in the study by Jensen and Bonding.8 The patient's PE tube should have allowed elevated pressure to be released. If the PE tube was occluded, the TM possibly perforated as a result of the increased pressure applied by the MACD. This would have occurred at a lower pressure than a normal TM. However, the pressure applied by the MACD at 40 cm H2O was only 7% of that reported for the lowest pressure observed for TM perforation in TMs with atrophic scarring.
The American Association for Respiratory Care clinical practice guideline on use of positive-pressure adjuncts to bronchial hygiene therapy lists “known or suspected TM rupture or other middle ear pathology” as a contraindication to this mode of treatment.10 However, the authors found no evidence of TM rupture or perforation noted as a hazard or complication resulting from utilization of positive-pressure devices in any other clinical practice guidelines. This would attest to the rarity of this event occurring. There are many respiratory devices that generate positive pressure; however, the pressures utilized are a fraction of what is required to rupture a TM based on the above studies. This may explain the scarcity of information in the medical literature.
It is possible that the combination of a compromised TM, an occluded PE tube, pressures generated by the MACD, and the patient performing a Valsalva maneuver simultaneously may have led to a significant increase in pressure and resulted in TM perforation. Another possibility is the uncertainty of the patient's actual compliance with the home-care regimen. During periods of time when he was not experiencing respiratory difficulties, we suspect that overall compliance was quite low. When he started to experience increased mucous production and dyspneic episodes, we suspect that he complied with the home-care regimen to avert possible deterioration resulting in hospitalization. Restarting his home-care regimen in an aggressive fashion may have caused the TM perforation. These potential explanations are speculative: however, some combination of these factors probably contributed to the perforated TM.
In this case, the importance of duplicating the home-care regimen in the clinic to validate the patient's complaints was invaluable. Clinicians were able to modify the pressures and minimize the air flow through the TM while directly visualizing the TM and getting direct input from the patient. Without visual confirmation of the perforated TM during NIV, downward adjustments in pressures during NIV and using the MACD might not have been performed. Although substantial efforts were made to minimize pressures, the TM would appear to heal and then subsequently start leaking air again. This continued over an extensive period of time (9 months) and led to an increase in PCO2 levels.
This case illustrates the following points. First, pressures utilized during NIV and with the MACD had to be reduced to allow the TM to heal. Second, following the reduction of pressures during NIV and with the MACD, there was a resultant increase in capillary PCO2 levels during the timeframe reviewed. Third, the patient's lack of compliance regarding the medical regimen led to a resuscitation event that was successfully managed. The TM eventually healed, and measures were subsequently initiated to increase pressures during NIV and with the MACD in an attempt to normalize the PCO2 levels. This rare presentation created many challenges for the medical team.
Acknowledgments
We thank Mr Michael Spigner (Public Relations Department, Arkansas Children's Hospital) for creating the illustration used in this manuscript.
Footnotes
- Correspondence: Gary R Lowe MEd RRT-NPS RPFT, Respiratory Care Services, Slot 303, 1 Children's Way, Little Rock, AR 72202-3591. E-mail: lowegr{at}archildrens.org.
Mr Gee presented a version of this paper at the AARC Congress 2012, held November 10–13, 2012, in New Orleans, Louisiana.
The authors have disclosed no conflicts of interest.
- Copyright © 2015 by Daedalus Enterprises





{kind=link}