

Abstract
BACKGROUND: COPD is associated with cardiovascular and renal dysfunction. Cystatin C (CysC) is a biomarker of renal function and an independent risk factor for all-cause and cardiovascular mortality among elderly persons. The aim of the study was to examine the prognostic role of CysC for in-hospital mortality in subjects with a COPD exacerbation.
METHODS: Upon admission, serum CysC levels and arterial blood gas analysis from 477 subjects with a COPD exacerbation were measured. Clinical characteristics were also recorded. A receiver operating characteristic curve analysis was used to determine the level of CysC that discriminated survivors from non-survivors. Univariate and multiple logistic regression analyses were used to identify the risk factors for in-hospital mortality. To reduce the influence of confounders, subgroup analyses were performed according to the comorbidities, including states of heart failure, renal dysfunction, and pH, PaCO2, and PaO2 levels.
RESULTS: During the in-hospital period, 59 subjects died, and 418 subjects recovered. The decedent group showed lower pH (7.27 ± 0.17 vs 7.38 ± 0.06, P < .001), higher CysC (2.21 ± 1.05 mg/L vs 1.39 ± 0.54 mg/L, P < .001), higher PaCO2 (77 ± 39 mm Hg vs 48 ± 14 mm Hg, P < .001), and lower PaO2 (74 ± 32 mm Hg vs 84 ± 26 mm Hg, P < .001) levels. The area under the receiver operating characteristic curve for the CysC prediction of death was 0.77 (95% CI 0.70–0.84). CysC values ≥1.59 mg/L were associated with significantly higher in-hospital mortality (relative risk = 5.49, 95% CI 3.24–9.32, P < .001). Multiple logistic regression analysis showed that pH <7.20, CysC ≥1.59 mg/L, and heart failure were independent predictors of in-hospital mortality. The subgroup analysis showed that the comorbid states of renal dysfunction, congestive heart failure, and the levels of pH, PaCO2, and PaO2 did not alter the conclusion that CysC was a mortality risk factor for subjects with a COPD exacerbation.
CONCLUSION: CysC was a strong and independent risk factor for hospital mortality secondary to COPD exacerbation.
Introduction
COPD is one of the leading causes of morbidity and mortality worldwide.1 Because COPD is considered to be a systemic disorder, one of its multiple co-morbidities is cardiovascular dysfunction. Epidemiological evidence suggests that impaired lung function is strongly correlated with increased cardiovascular-related deaths.2,3 Cardiac dysfunction may trigger exacerbation in up to 25% of COPD patients, and acute myocardial infarction and chronic heart failure may be associated with COPD exacerbation, whereas acute respiratory failure itself may lead to right and/or left ventricular failure.4,5
Another co-morbidity associated with COPD is renal dysfunction. Gjerde et al6 reported that the prevalence of a glomerular filtration rate of <60 mL/min was 9.6% in female COPD subjects and 5.1% in male subjects. Undiagnosed renal failure is a concern, particularly in elderly COPD patients and in COPD patients with cachexia.
Cystatin C (CysC) is a low-molecular weight protein found in the plasma, which is freely filtered by the renal glomerulus and reabsorbed in the tubules, where it is metabolized almost completely.7 A serum CysC-based equation has even been proposed to estimate the glomerular filtration rate in patients with chronic kidney disease.8 Recent studies have revealed that CysC has a predictive and prognostic value in cardiovascular disease, especially coronary artery disease and heart failure.9–13 However, the literature on the role of CysC in subjects with COPD exacerbation is sparse. One study that examined the level of CysC in COPD subjects showed that a high CysC concentration may be a potential indicator of impaired lung function and that routinely measuring CysC may improve the diagnosis and assessment of COPD severity in elderly male subjects.14 Another study examined the 1-y prognostic value of elevated CysC among subjects with exacerbation of chronic lung disease who were hospitalized and showed that CysC has no predictive value for mortality in subjects with chronic respiratory disease.15 However, no articles have presented an evaluation of the prognostic value of CysC in subjects with COPD exacerbation. It is possible that CysC measurements can contribute to the early identification of patients at risk for the development of clinically important ventricular dysfunction. We hypothesized that CysC exhibits an inverse relationship with the prognosis of COPD exacerbation. Accordingly, the objective of the current study was to explore the in-hospital prognostic value of elevated CysC during COPD exacerbation.
QUICK LOOK
Current knowledge
COPD is considered to be a systemic disorder, and cardiovascular and renal dysfunction are 2 of its multiple co-morbidities. Cystatin C (CysC) has a predictive and prognostic value in cardiovascular disease, especially coronary artery disease and heart failure. Understanding the prognostic value of CysC in patients with COPD exacerbation could contribute to the early identification of patients at risk for death.
What this paper contributes to our knowledge
In this cohort study, univariate and multiple logistic regression analysis showed that pH, CysC, and heart failure were independent predictors of in-hospital mortality; the comorbid states of renal dysfunction, congestive heart failure, and levels of pH, PaCO2, and PaO2 did not alter the conclusion that CysC was a mortality risk factor for subjects with COPD exacerbation. CysC may be used to evaluate the in-hospital mortality for patients with COPD exacerbation.
Methods
Study Design
This was a prospective study conducted in the Third Affiliated Hospital of Guangzhou Medical University, Guangzhou, Guangdong, China, between July 2010 and July 2013 in subjects hospitalized with a diagnosis of COPD exacerbation. Subjects were included if the following criterion was met: a diagnosis of COPD according to the criteria set by the Global Initiative for Chronic Obstructive Lung Disease (ie, a post-bronchodilator FEV1/FVC of <0.7 according to the records of lung function testing at our hospital). COPD exacerbation was defined by the presence of an increase in at least 2 of 3 symptoms: dyspnea, cough, and sputum purulence. Patients were excluded if the primary reason for their hospitalization was not an exacerbation of COPD according to their medical history (information from interview and clinical records provided by the patients). Patients diagnosed with coronary ischemia were also excluded along with those diagnosed with chronic renal insufficiency, renal failure, or nephritis before the COPD exacerbation. However, we did not exclude subjects who had been diagnosed with heart failure. Subjects' treatment was not influenced by participation in the study. The study was carried out according to the principles of the Declaration of Helsinki and was approved by the ethics committee of the Third Affiliated Hospital of Guangzhou Medical University.
Biochemical Measurements
The age, sex, and smoking status of subjects were recorded at the time of admission. CysC levels were measured within 24 h of admission. Scattering immunoturbidimetry was used to measure the serum CysC concentration. Serum creatinine levels were assayed using the Jaffe method on a Hitachi Modular Pre-Analytics Plus system (Roche Diagnostics, Basel, Switzerland). The glomerular filtration rate was estimated within 24 h of admission by the simplified Modification of Diet in Renal Disease equation.16 Renal dysfunction was defined as a glomerular filtration rate of <90 mL/min. An arterial blood gas analysis (PaO2, PaCO2, and pH) was performed upon admission. Congestive heart failure was diagnosed according to the Chinese guidelines published in 2007 for the diagnosis and management of chronic heart failure,17 which included typical symptoms of heart failure (breathlessness, orthopnea, paroxysmal nocturnal dyspnea, reduced exercise tolerance, fatigue, tiredness, increased time to recover after exercise, and ankle swelling); typical signs of heart failure (elevated jugular venous pressure, hepatojugular reflux, a third heart sound, a laterally displaced apical impulse, and a cardiac murmur); and a reduced left ventricular ejection fraction.
Statistical Analyses
The primary outcomes of interest were in-hospital mortality and factors associated with in-hospital mortality. Continuous variables are presented as the means ± SD. Categorical variables are presented as n (%). Comparisons between groups were made using analysis of variance (for continuous variables) or a chi-square test (for categorical variables). Logistic regression analysis was used to identify independent variables associated with death. To limit the number of events per variable, only variables yielding univariate associations with P ≤ .05 were included in the logistic regression model. Receiver operating characteristic curve analysis was used to optimize the minimal level of CysC that predicted mortality. Subgroup analyses were performed according to the comorbidities, including states of heart failure, renal dysfunction, and the levels of pH, PaO2, and PaCO2. Nonparametric data are reported as the mean ± SD. Across-groups comparison of 3 groups was performed using the non-parametric Kruskal–Wallis test followed by the Dunn post hoc test. Direct comparisons between 2 groups were performed with the nonparametric Mann–Whitney test. Stata 7.0 (Stata, College Station, Texas) and GraphPad Prism 5.0 (GraphPad Software, La Jolla, California) were used for all calculations. A 2-sided P value of < .05 was considered to be statistically significant.
Results
A total of 477 subjects with COPD exacerbation were included in our cohort study. The differences between survivors and non-survivors among the hospitalized subjects are listed in Table 1. The subjects who died were more likely to have renal dysfunction. In addition, the subjects who died were significantly more hypercapnic (PaCO2 = 77 ± 39 mm Hg) and older (79.9 ± 9.7 y) than the survivors (PaCO2 = 48 ± 14 mm Hg and age 76.9 ± 9.3 y, respectively). There was no difference in lung function between survivors and those who died. The pH and PaO2 levels were significantly lower in non-survivors (pH 7.27 ± 0.17, PaO2 = 74 ± 32 mm Hg) compared with survivors (pH 7.38 ± 0.06, PaO2 = 84 ± 26). The plasma concentrations of CysC, creatinine, and blood urea nitrogen were higher in non-survivors (CysC = 2.21 ± 1.05 mg/L, creatinine = 123.8 ± 83.3 μmol/L, and blood urea nitrogen = 11 ± 8 mmol/L) than in survivors (CysC = 1.39 ± 0.54, creatinine = 93.8 ± 51.5 μmol/L, and blood urea nitrogen = 7 ± 8 mmol/L).
Baseline Characteristics and Survival of Subjects Hospitalized With COPD Exacerbation
Receiver operating characteristic curves were used to determine the cut-off values for the biochemical parameters. The optimal values of CysC for predicting death were defined as the concentrations with the largest sensitivity plus specificity for the curves. The receiver operating characteristic curve analysis (Fig. 1) identified CysC levels of ≥1.59 mg/L as the optimal level that discriminated the survivors from the non-survivors (area under the receiver operating characteristic curve = 0.77, 95% CI = 0.70–0.84, P < .001). The entire cohort was then divided into 2 groups according to the serum CysC levels. There were 148 subjects with CysC levels of ≥1.59 mg/L and 329 with CysC levels of <1.59 mg/L. Table 2 shows non-statistically significant associations of CysC levels with sex and PaO2 (P = .14 and P = .37, respectively) and statistically significant associations with age, pH, PaCO2, and the concentration of creatinine and blood urea nitrogen (P < .001).

A receiver operator characteristic curve for plasma cystatin C as an overall predictor of death in subjects with COPD exacerbation. Area under the receiver operator characteristic curve = 0.77 (95% CI 0.70–0.84).
Baseline Characteristics Stratified by the Cystatin C Concentration
In univariate analyses, the survival of subjects with CysC levels <1.59 mg/L and those with CysC levels ≥1.59 mg/L differed significantly. The probability of in-hospital death of subjects with CysC levels ≥1.59 mg/L was 28.4%, whereas the corresponding probability of death in subjects with CysC levels <1.59 mg/L was 5.2% (RR = 5.49, 95% CI = 3.24–9.32). At the same time, pH, PaCO2, PaO2, renal dysfunction, and congestive heart failure also predicted in-hospital mortality, whereas sex, age, and history of smoking did not (see Table 3).
Mortality Risk in Subjects With COPD Exacerbation
The logistic regression revealed that the factors associated with in-hospital mortality were a pH of <7.20 (odds ratio 4.33, 95% CI 2.27–8.24), PaO2 < 60 mm Hg (odds ratio 3.41, 95% CI 1.61–7.22), and a CysC level of ≥1.59 mg/L (odds ratio 6.20, 95% CI 2.61–14.75) (Table 4).
Logistic Regression Analyses of the Risk Factors Associated With Mortality in Subjects With COPD Exacerbation
Table 5 and Figures 2 and 3 show the results of the subgroup analyses stratified by the comorbidities of congestive heart failure, renal dysfunction, and the levels of pH, PaCO2, and PaO2. Our analysis showed that CysC was a mortality risk factor for subjects with COPD exacerbation with and without renal dysfunction or congestive heart failure. Our results also showed that CysC was a mortality risk factor for subjects with COPD exacerbation with various levels of pH, PaCO2, and PaO2.
Subgroup Analysis of the Mortality Risk in Subjects With COPD Exacerbation
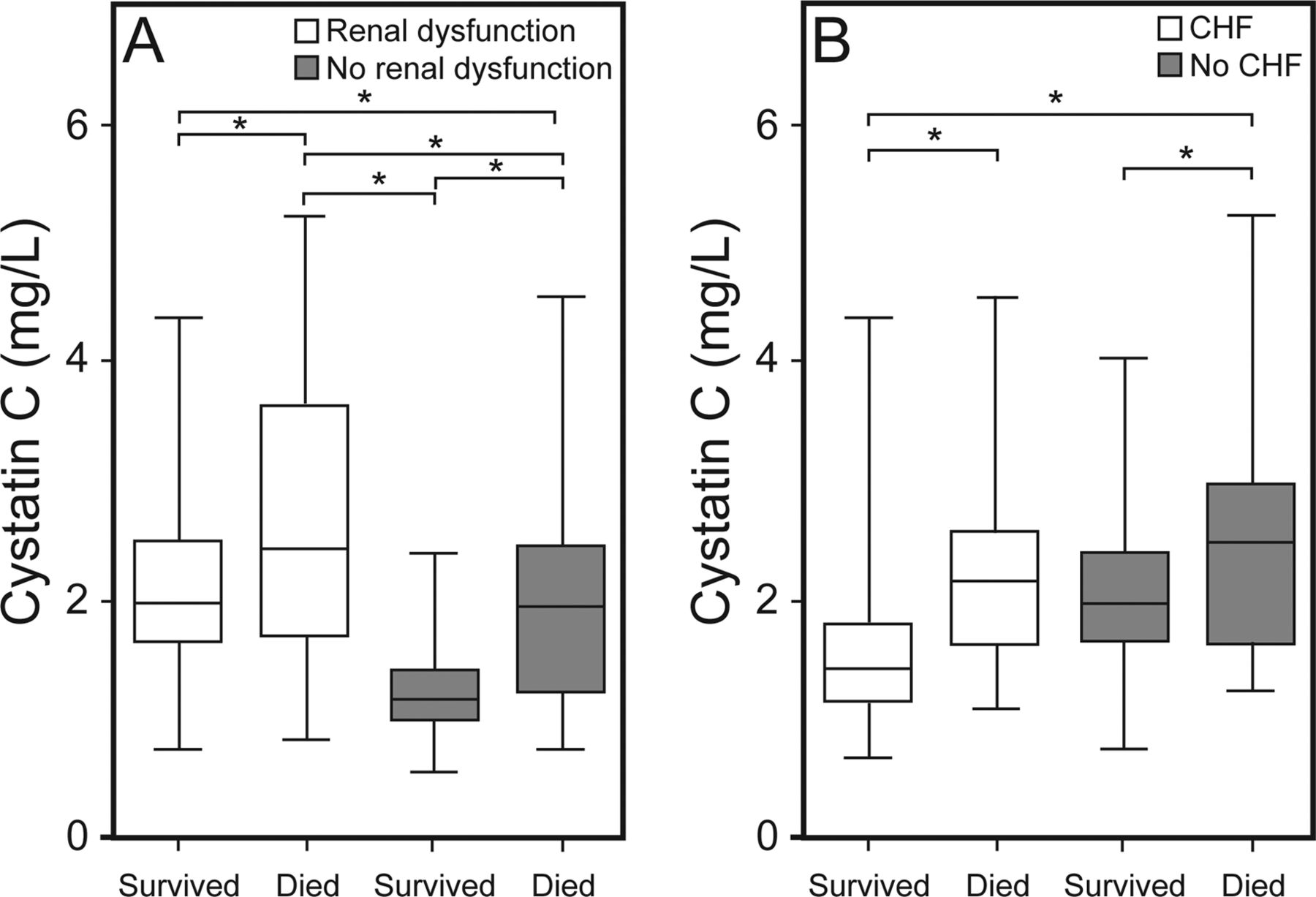
Cystatin C levels (mg/L) in survivor and non-survivor subjects with COPD exacerbation stratified by the comorbid presence of renal dysfunction (A) and congestive heart failure (B) at the time of admission. Boxes show first and third quartiles, center lines denote the median, and whiskers show the minimum and maximum. * P < .05.

Cystatin C levels (mg/L) in the survivor and non-survivor subjects with COPD exacerbation stratified by the levels of pH (A), PaO2 (B), and PaCO2 (C). Low pH is <7.35, and high pH is >7.35; low PaO2 is <60 mm Hg, and high PaO2 is ≥60 mm Hg; low PaCO2 is <50 mm Hg, and high PaCO2 is ≥50 mm Hg. Boxes show first and third quartiles, center lines denote the median, and whiskers show the minimum and maximum. * P < .05.
Discussion
This study is the most comprehensive prospective study to report associations between the CysC status determined during hospitalization for COPD exacerbation and short-term prognosis. The main finding of the current study was that elevated CysC is a strong independent prognostic factor for in-hospital mortality (RR = 5.49, 95% CI 3.24–9.32). Even after adjusting for multiple, well-accepted predictors of mortality, a CysC level ≥1.59 remained a strong predictor of in-hospital mortality (odds ratio = 6.20, 95% CI (2.61–14.75). To the best of our knowledge, this association between CysC elevation and mortality due to COPD exacerbation is a novel finding. Moreover, it may be important for risk stratification and the treatment of patients hospitalized with COPD exacerbation. Many studies have reported the predictive value of CysC, and serum CysC has been reported not only as a marker of glomerular filtration rate but also as an independent risk factor for all-cause and cardiovascular mortality among elderly persons with chronic kidney disease with or without renal impairment.18 One study reported that higher CysC levels independently predicted 5 y all-cause and cardiovascular death in subjects with peripheral arterial disease.19 A positive correlation between CysC and inflammatory parameters, including interleukin-6, resistin, tumor necrosis factor, and C-reactive protein, has been reported.20 Carrasco-Sánchez et al21 reported that the serum CysC level at the time of admission in subjects with heart failure with preserved ejection fraction is a strong and independent predictor of an unfavorable outcome. This relationship is also present in patients without advanced renal dysfunction.21 Akgul et al22 reported that the presence of high CysC levels at the time of admission was associated with increased in-hospital and 1-month cardiovascular mortality in subjects with ST-elevation myocardial infarctions undergoing primary percutaneous coronary intervention. Increased levels of CysC were an independent predictor of cardiac events within a 1-y follow-up in this contemporary series of Mediterranean subjects with non-ST-elevation acute coronary syndrome.11 The concentration of CysC was strongly associated with long-term all-cause and cardiovascular mortality in subjects referred for coronary angiography, irrespective of the renal function status based on creatinine measurements.23 However, the literature describing the role of CysC in COPD is sparse, and few studies have addressed this issue to date. In China, Zhang et al14 reported that high CysC levels were directly associated with decreased lung function in elderly Chinese men with COPD. In a large representative non-institutionalized United States population, Rokadia and Agarwal24 demonstrated an association between emphysema and serum CysC. Active smokers with emphysema had significantly higher CysC levels. Takeyabu et al25 reported that increased levels of CysC were present in the bronchoalveolar lavage fluid from subjects with subclinical emphysema. Pérez-Calvo et al15 analyzed CysC levels at the time of admission in 107 subjects with exacerbation of chronic lung disease. During a 12-month follow-up, the mortality, new hospital admissions, and prescriptions of diuretics were recorded. The results showed that CysC had no predictive value in terms of mortality for subjects with chronic respiratory disease.
In the present study, our results showed that the levels of CysC were associated with the comorbidities of renal dysfunction, congestive heart failure, old age, lower pH, and higher PaCO2 (Table 2). We also found that age, heart failure, hypercapnia, hypoxemia, and pH <7.20 were also risk factors for the death of subjects with COPD exacerbation: These factors may be involved in the mechanism for the CysC elevation in non-survivors versus survivors. Our results were consistent with the previous studies.26,27 Li et al26 reported that hypercapnia and chronic pulmonary heart disease were independent risk factors for mortality in hospitalized subjects with COPD exacerbation. Fruchter and Yigla27 also found that the presence of ischemic heart disease and PaO2 levels upon admission were independent predictors of mortality for subjects with COPD exacerbation. In our study, elevated CysC levels were most often detected in older subjects and in subjects who were more hypoxemic, hypercapnic, and acidotic and had high levels of blood urea nitrogen and creatinine; however, there were no significant correlations with PaO2 or sex (Table 2). To our knowledge, no studies of the relationship between CysC and the results of a blood gas analysis have been published. Akgul et al22 reported that subjects in the high CysC group were older. Sarnak et al28 determined that elevated CysC was an independent predictor of heart failure after adjusting for traditional and nontraditional risk factors for heart failure. Ix et al29 found that higher CysC had a stronger association with diastolic compared with systolic dysfunction in the Heart and Soul Study.
To reduce the influence of confounding factors, we performed the subgroup analysis stratified by the comorbidities of congestive heart failure, renal dysfunction, and levels of pH, PaO2, and PaCO2. We found that the comorbidities of renal dysfunction, congestive heart failure, and levels of pH, PaCO2, and PaO2 did not alter the conclusion that CysC was a mortality risk factor for subjects with COPD exacerbation. In general, patients with COPD exacerbation may suffer several types of comorbidities, including congestive heart failure and renal dysfunction, and may have a high PaCO2 and a low pH. At the same time, the comorbidities of congestive heart failure, renal dysfunction, high PaCO2, and low pH also could affect the level of CysC, which may be related to the source of elevated CysC.
In our study, the levels of CysC, which is a form of cysteine protease inhibitor, were higher in the non-survivor group than in the survivors. Cysteine proteases (cathepsins) have a role in the pathogenesis of COPD.30 Cathepsin-L has been detected in bronchoalveolar lavage fluid from patients with emphysema,31 and alveolar macrophages in patients with COPD secrete more cysteine proteases than macrophages from normal smokers or nonsmokers.31 Furthermore, some authors have suggested that an increased concentration of CysC may reflect an attempt to counterbalance a potentially damaging level of increased elastolytic activity.32 However, we did not determine the levels of cysteine protease inhibitor activity. We therefore cannot conclude that there was a relationship between the inhibitor activity and poor prognosis.
Our study had several limitations. First, the diagnosis of COPD was established according to historical spirometry results. We were unable to recruit patients with stable COPD before hospitalization for COPD exacerbation for the purpose of this study. Second, we only recorded the mortality of hospitalized subjects with COPD exacerbation. The follow-up time was relatively short, and the study was mostly cross–sectional. Third, the intervention for COPD exacerbation was not identical for all subjects, which is another confounder. Fourth, we did not collect information regarding the subjects' use of glucocorticoids before COPD exacerbation, and the use of glucocorticoids may affect the level of CysC. Finally, the relatively small number of subjects included in each group also made it difficult to draw firm conclusions from the data.
Conclusions
An elevated CysC level present during COPD exacerbation is an important and independent determinant of subsequent mortality in a hospital setting.
Footnotes
- Correspondence: Pixin Ran PhD, Guangzhou Institute of Respiratory Disease, First Affiliated Hospital, Guangzhou Medical University, 151 Yanjiang Road, Guangzhou, Guangdong 510120, China. E-mail: pxran{at}vip.163.com.
Drs Hu and Wu are co-first authors.
This study was supported by the National Key Technology R&D Program of the 12th National Five-Year Development Plan 2012BAI05B01 (to Dr Ran) and by the Guangzhou municipal health bureau scientific research fund (201102A213176). The authors have disclosed no conflicts of interest.
- Copyright © 2016 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}