

Abstract
BACKGROUND: Technological advances have increased ventilator mode complexity and risk of operator error.
OBJECTIVE: To compare differences in volume control (VC) ventilation with set-point and dual targeting. Two hypotheses were tested: tidal volume (VT) delivery is different with VC using set-point versus dual targeting during active versus passive breathing; VC with dual targeting delivers VT similar to pressure support ventilation (PS) with active breathing.
METHODS: The Ingmar Medical ASL 5000 lung model simulated pulmonary mechanics of an adult patient with ARDS during active and passive ventilation. Resistance was standardized at 10 cm H2O/L/s and compliance at 32 mL/cm H2O. Active breathing was simulated by setting the frequency (f) = 26 breaths/min, and adjusting the muscle pressure (Pmus) to produce a VT of 384 mL. VC was initiated with the Puritan Bennett 840 (set-point targeting) and the Servo-i (dual targeting) at VT = 430 mL, mandatory f = 15 breaths/min, and PEEP = 10 cm H2O. During PS, cycle threshold was set to 30% and peak inspiratory pressure adjusted to produce a VT similar to that delivered during VC. Expiratory VT was collected on 10 consecutive breaths during active and passive breathing with VC and PS. Mean VT differences (active vs passive model) were compared using analysis of variance. Statistical significance was established at P < .05.
RESULTS: The mean ± SD VT difference varied with targeting schemes: VC set-point = 37.3 ± 3.5 mL, VC-dual = 77.1 ± 3.3 mL, and PS = 406.1 ± 1.5 mL (P < .001). Auto-triggering occurred during VC set-point with the active model.
CONCLUSIONS: Dual targeting during VC allows increased VT, compared to set-point, but not as much as PS.
- targeting scheme
- mode of ventilation
- breath sequence
- mechanical ventilator
- tidal volume
- simulation
- taxonomy
Introduction
The respiratory therapist plays a vital role in the initiation and management of mechanical ventilation. The ability to support the work of the respiratory system and safely and effectively improve gas exchange has been substantially influenced by the variety of options available to deliver ventilatory support.1 However, lack of standardized nomenclature, innovative marketing strategies, and technological advancements complicate the process of determining ventilator output and mode capability. It is difficult for the clinician to have a comprehensive understanding of mode capability when ventilator manufacturers coin unique names for different modes of ventilation or identical names for different modes.2
The problem is wide in scale and affects not only practicing clinicians, but educators and students as well. The confusion promulgated by ventilator manufacturers, published in textbooks3 and found in the literature,4–6 makes learning difficult, encumbers teaching and competency assessment,7 and increases the propensity for medical errors.8,9 The literature does offer a viable solution to determine mode identification. This systematic method uses 3 essential components to classify a mode of ventilation; the control variable, breath sequence, and targeting scheme.10
The control variable describes how the ventilator manages pressure, volume, and flow during a breath. Since a ventilator can control only one variable at a time, the control variable represents that which is independent of the patient's lung mechanics (including effort) during breath delivery. Volume control (VC) ventilation implies a preset tidal volume (VT) and inspiratory flow waveform. During VC ventilation the shape of the volume and flow waveforms are not affected by the patient's respiratory system mechanics. Pressure control (PC) implies a preset inspiratory pressure and inspiratory time. During PC ventilation the shape of the pressure waveform is not affected by the patient's respiratory system mechanics.
The breath sequence is a particular pattern of mandatory or spontaneous breath delivery (Table 1). A spontaneous breath is one for which inspiration is both triggered (initiated) and cycled (ended) by the patient. Any other combination of patient and machine trigger and cycle events is considered a mandatory breath (ie, patient triggered and machine cycled, machine triggered and patient cycled, and machine triggered and machine cycled).
A Description of the 3 Breath Sequences Used to Classify Modes
The targeting scheme is a model of the relationship between operator inputs and ventilator outputs to achieve a specific ventilatory pattern. The targeting scheme is a key component of a mode description. There are 6 basic targeting schemes used on commercially available mechanical ventilators (Table 2).11 A “target” is a predetermined goal of ventilator output. Targets can be viewed as the parameters of the targeting scheme. Within-breath targets are the parameters of the pressure, volume, or flow waveform. Between-breath targets are used with more advanced targeting schemes, where targets act over multiple breaths.
Glossary of Ventilator Targeting Scheme Terms and Definitions
The mode called “Volume Assist/Control” on the Covidien PB 840 ventilator is an example of VC ventilation with set-point volume targeting. Set-point targeting is a control system for which the operator sets all parameters of the pressure waveform (PC modes) or volume and flow waveforms (VC modes). Advanced VC modes actually allow the ventilator to make small adjustments to the set inspiratory flow to compensate for such factors as patient circuit compliance.12 From an engineering point of view, this is adaptive feedback control, but from a ventilator mode taxonomy point of view, such adjustments are better seen as a way of implementing operator preset values, and thus classified as set-point targeting.
The mode called “Volume Control” on the Maquet Servo-i is an example of VC with a dual targeting scheme. Dual targeting in this case means that each breath starts out in VC, but if the patient makes an inspiratory effort sufficient to decrease airway pressure by 3 cm H2O, the ventilator switches to PC within the breath. Depending on the intensity of the inspiratory effort, the ventilator may switch back to VC with a volume cycle criterion or end inspiration in PC with a flow cycle criterion, similar to a pressure support breath. In fact, the Servo-i operator's manual (V3.1, page 36) actually says “… if a pressure drop of 3 cm H2O is detected during inspiration, the ventilator cycles to Pressure Support with a resulting increase in inspiratory flow.”
The aforementioned ventilator manufacturers have proprietary algorithms for breath delivery. Superficially, these 2 modes may appear to be forms of VC continuous mandatory ventilation (VC-CMV), particularly in passive patients or those making very small inspiratory efforts (eg, just enough to trigger the breath). But the different targeting schemes make them respond very differently to large inspiratory efforts. “Volume Assist/Control” on the Covidien PB 840 is classified as VC-CMV. However, “Volume Control” on the Maquet Servo-i is classified as VC-IMV. The reason is that the dual targeting scheme allows the patient's inspiratory effort to change what would have been a mandatory VC breath into a spontaneous PC breath. Such a breath is almost identical (with a large patient effort, low set VT, and short inspiratory time) to PC continuous spontaneous ventilation (PC-CSV) (ie, pressure support, which is certainly counter-intuitive for a mode called “Volume Control”). The differences between these 2 modes may have clinically important effects on VT delivery and patient-ventilator synchrony. Indeed, one would expect that was the reason for the design differences. The purposes of this study were to use a mechanical lung model to determine if there are differences in delivered VT between set-point targeting and dual targeting, and to evaluate VT delivery during dual targeting and pressure support ventilation (PSV). Two hypotheses were tested:
VT delivery is different with VC using set-point versus dual targeting, when comparing active versus passive breathing.
VC with dual targeting delivers VT similar to PSV with active breathing.
QUICK LOOK
Current knowledge
Volume control ventilation implies a preset tidal volume and inspiratory flow waveform. During volume control ventilation the shape of the volume and flow waveforms are not affected by the patient's respiratory system mechanics.
What this paper contributes to our knowledge
During volume control ventilation, dual targeting, compared to set-point targeting, allowed an increased tidal volume and avoided double-triggering. However, tidal volume and flow increased with dual targeting, allowing tidal volumes greater than set. These findings have important implications to the clinical practice of lung protective ventilation.
Methods
Lung Model
The ASL 5000 (Ingmar Medical, Pittsburgh, Pennsylvania) is a sophisticated device comprised of a piston driven by a motor that is controlled by software based on LabView, a graphical programming environment created by National Instruments. The piston movement is governed by the equation of motion for the respiratory system, such that the distance and speed traveled simulate compliance (C) and resistance (R), respectively. Both of these parameters may be modeled as either linear or non-linear. The models may also be programmed to change from breath to breath in a scripted fashion. The user interface allows the operator to create both active and passive lung models and gives precise control over the simulated muscle pressure function (Pmus, ie, patient effort for both inspiration and expiration). It is important to note that, by definition, Pmus is always positive during inspiration. However, the ASL depicts it as a negative value during inspiration, to unclutter the waveform displays.
Lung Model Settings
The Ingmar Medical ASL 5000 lung model was programmed to simulate the pulmonary mechanics of an adult patient with ARDS during active and passive ventilation.13 Resistance was standardized at 10 cm H2O/L/s and compliance at 32 mL/cm H2O for all experimental conditions.
Active breathing was simulated by adjusting Pmus on the ASL 5000 to produce a VT of 384 mL.13 This adjustment was made prior to connecting the lung model to the ventilator with a standard adult circuit. During active breathing, Pmus settings were as follows: Pmax 15 cm H2O, Increase 30%, Hold 0%, and Release 25% (Fig. 1). The model breathing frequency was set to 26 breaths/min. A passive model was also used with the same settings for resistance and compliance but Pmax set to zero.
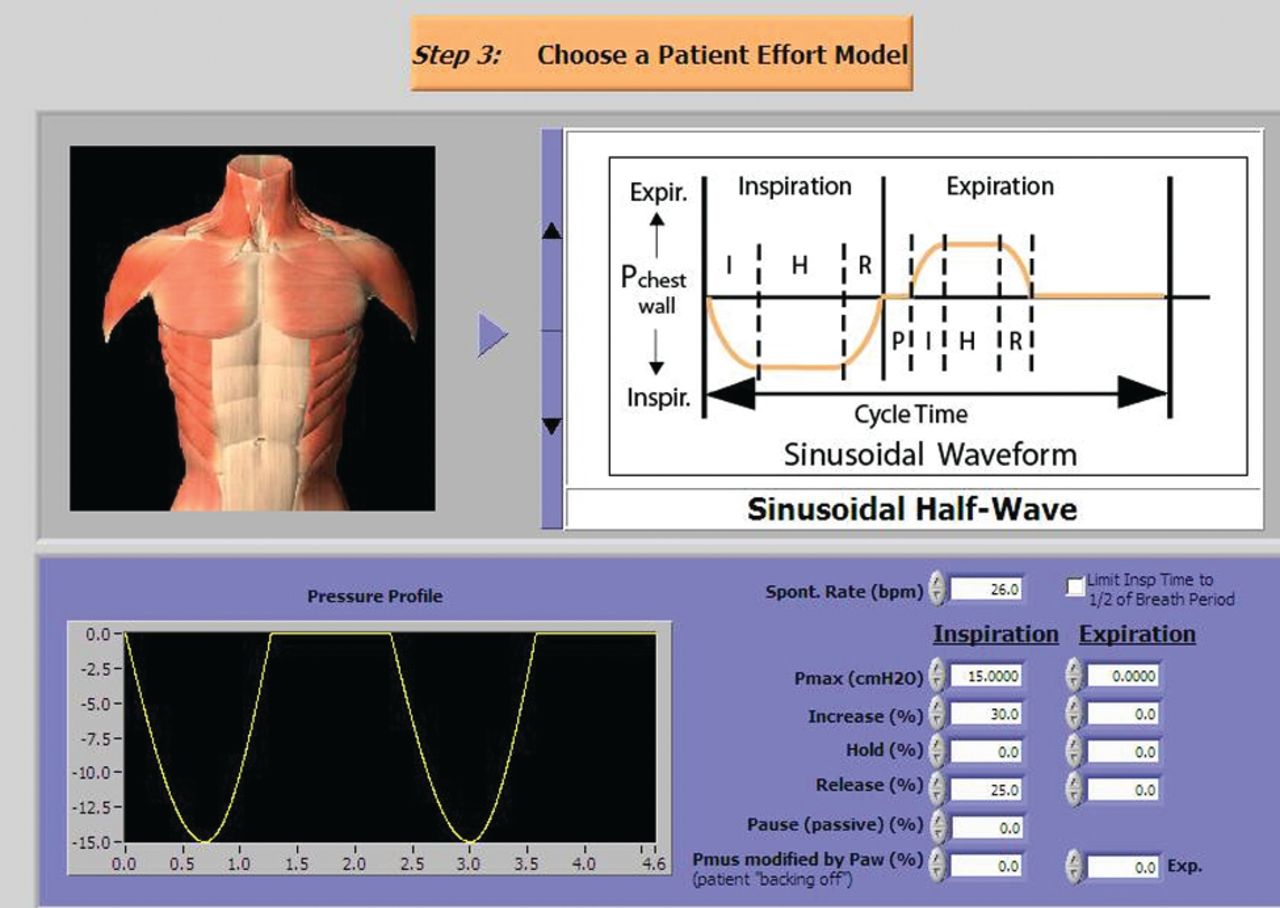
Screen capture of the parameter settings for muscle pressure (Pmus) during active breathing.
Ventilator Settings Used for Determining Differences in VT Delivery With VC Using Set-point Versus Dual Targeting
Two ventilators, Puritan Bennett 840 (Covidien, Mansfield, Massachusetts) and the Servo-i (Maquet, Wayne, New Jersey) were used to evaluate VC ventilation with set-point and dual targeting, respectively. The ventilator settings for the VC modes are found in Table 3.
Ventilator Settings Used to Test Differences in VT Delivery With Set-Point and Dual Targeting During Volume Control Ventilation
Ventilator Settings Used for Determining Differences in VT Delivery Between VC With Dual Targeting and PSV With an Active Breathing Model
The Servo-i was used to evaluate the effect of VC with dual targeting and PSV on VT delivery during active breathing. PC-CMV was used with the passive lung model to determine the inspiratory pressure setting needed to achieve the target exhaled VT of approximately 430 mL. These settings (shown in Table 4) were used during PC-CSV (ie, Pressure Support) with the active lung model to test the second hypothesis.
Ventilator Settings During Pressure Control Ventilation With the Servo-i
Experimental Procedures
Each mode was evaluated using passive and active lung models. The change in average values for VT, inspiratory time, and mean airway pressure between passive and active models were calculated and compared.
Data Collection and Analysis
Exhaled VT, inspiratory time, and airway pressure were collected on 10 consecutive breaths during each experimental condition. Data were entered into data analysis and graphing software (SigmaPlot 12.0, Aspire Software International, Ashburn, Virginia) for analysis. Differences (active minus passive model) in mean VT, inspiratory time, and mean airway pressure were compared using analysis of variance. Values for peak inspiratory flow rate were collected over 20 breaths during VC with set-point and dual targeting and Pressure Support using the active lung model. Differences in mean inspiratory flow were compared using analysis of variance. Statistical significance was established at P < .05. The ASL 5000 software was used to capture representative pressure and volume waveforms with the active and passive lung models during VC with set-point and dual targeting, as well as PC-CMV and Pressure Support.
Results
Representative waveforms for pressure and flow for VC with set-point and dual targeting in the passive lung model are displayed in Figure 2. The mean VT for set-point targeting was 402 mL, and for dual targeting 447 mL. The mean VT for PC was 439 mL. The mean value for inspiratory time was 0.6 second, and the average mean airway pressure was 12 cm H2O for all 3 modes.

Pressure, and flow waveforms during volume control (VC) with set-point and dual targeting with the passive lung model. Black = flow. Red = airway pressure. Blue = simulated muscle pressure.
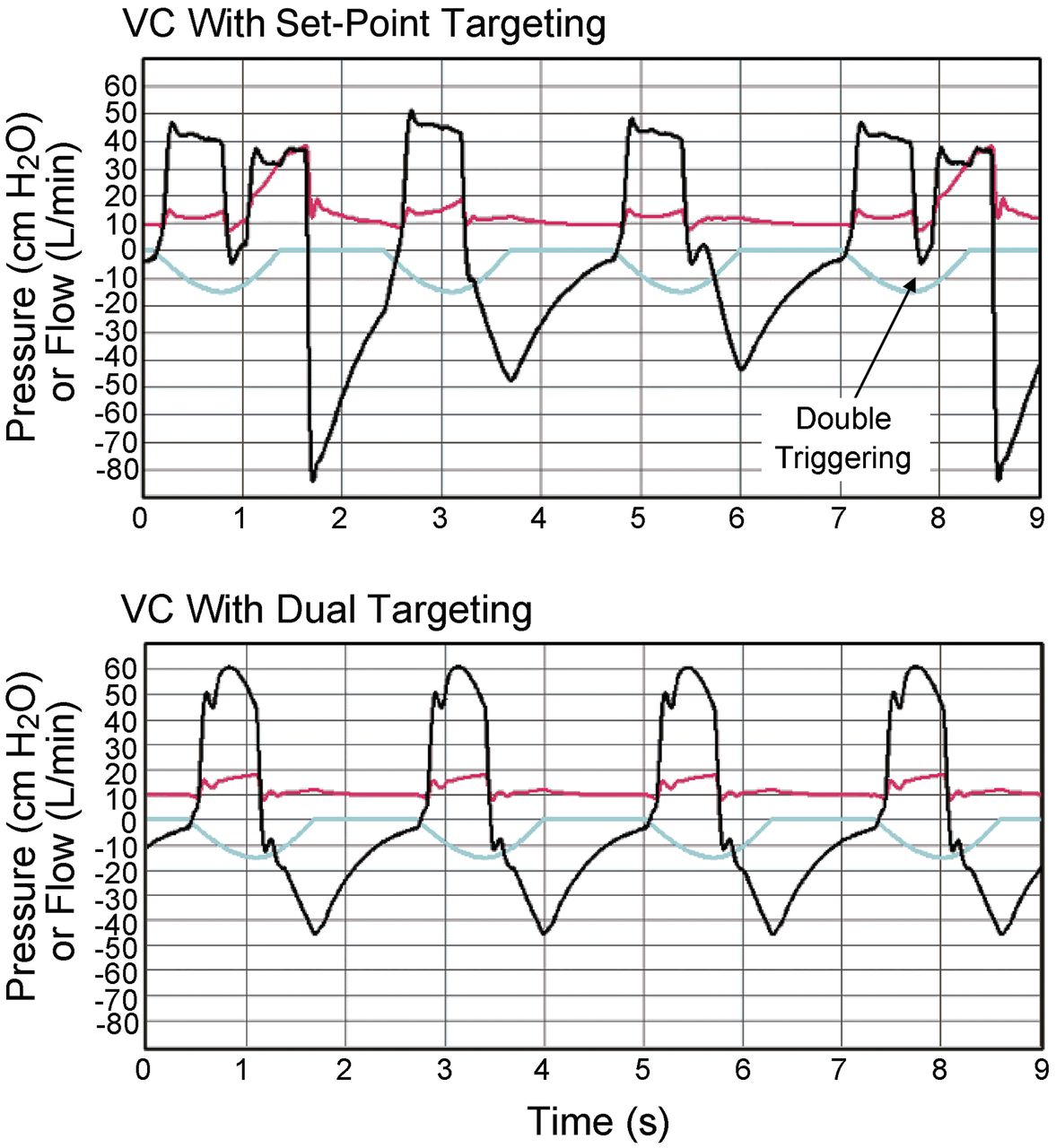
There was a significant difference in VT, inspiratory time, and mean airway pressure among the 3 modes during active versus passive breathing (Table 5). Figure 3 shows the changes in the pressure and volume waveforms that occurred with set-point and dual targeting during VC with simulated inspiratory efforts. Double-triggering occurred on every fourth breath during VC with set-point targeting. We used the breaths just before the double trigger event to calculate mean VT for comparison with dual targeting. Note that the airway pressure waveform was deformed (concave upward) during inspiration with set-point targeting, but much less so with dual targeting, indicating that the simulated patient received less inspiratory work unloading with set-point targeting.
The Change in Expiratory Tidal Volume (Active − Passive), Inspiratory Time, and Mean Airway Pressure During Volume Control With Set-Point and Dual Targeting Compared to Pressure Support

Pressure and flow waveforms during volume control (VC) with set-point and dual targeting in an active lung model. Note the double triggering with set-point targeting. Black = flow. Red = airway pressure. Blue = simulated muscle pressure.
Figure 4 compares VC with dual targeting with the passive and active lung models. It shows how a sufficient inspiratory effort (ie, one that decreases inspiratory pressure by 3 cm H2O) signals the ventilator to switch from VC to PC, with the result that the ventilator delivers more flow (and volume) to meet the demand.

Pressure and flow waveforms during volume control continuous mandatory ventilation (VC-CMV) with dual targeting in the passive and active lung models. Note the switch from VC to pressure control (PC) when the active inspiratory effort decreases inspiratory pressure below the default threshold of 3 cm H2O, and the subsequent increase in inspiratory flow. Black = flow. Red = airway pressure. Blue = simulated muscle pressure.
Figure 5 shows how flow delivery during VC with dual targeting compares to PC in the Pressure Support mode. Statistically significant differences in mean inspiratory flow occurred with the various targeting schemes. Inspiratory flow did not vary from set flow during active breathing during VC with set-point targeting. Mean inspiratory flow was increased during VC with dual targeting (61.2 L/min ± 0.2), but not as much as with PSV (91.2 L/min ± 0.2) (P < .001) (Table 6).
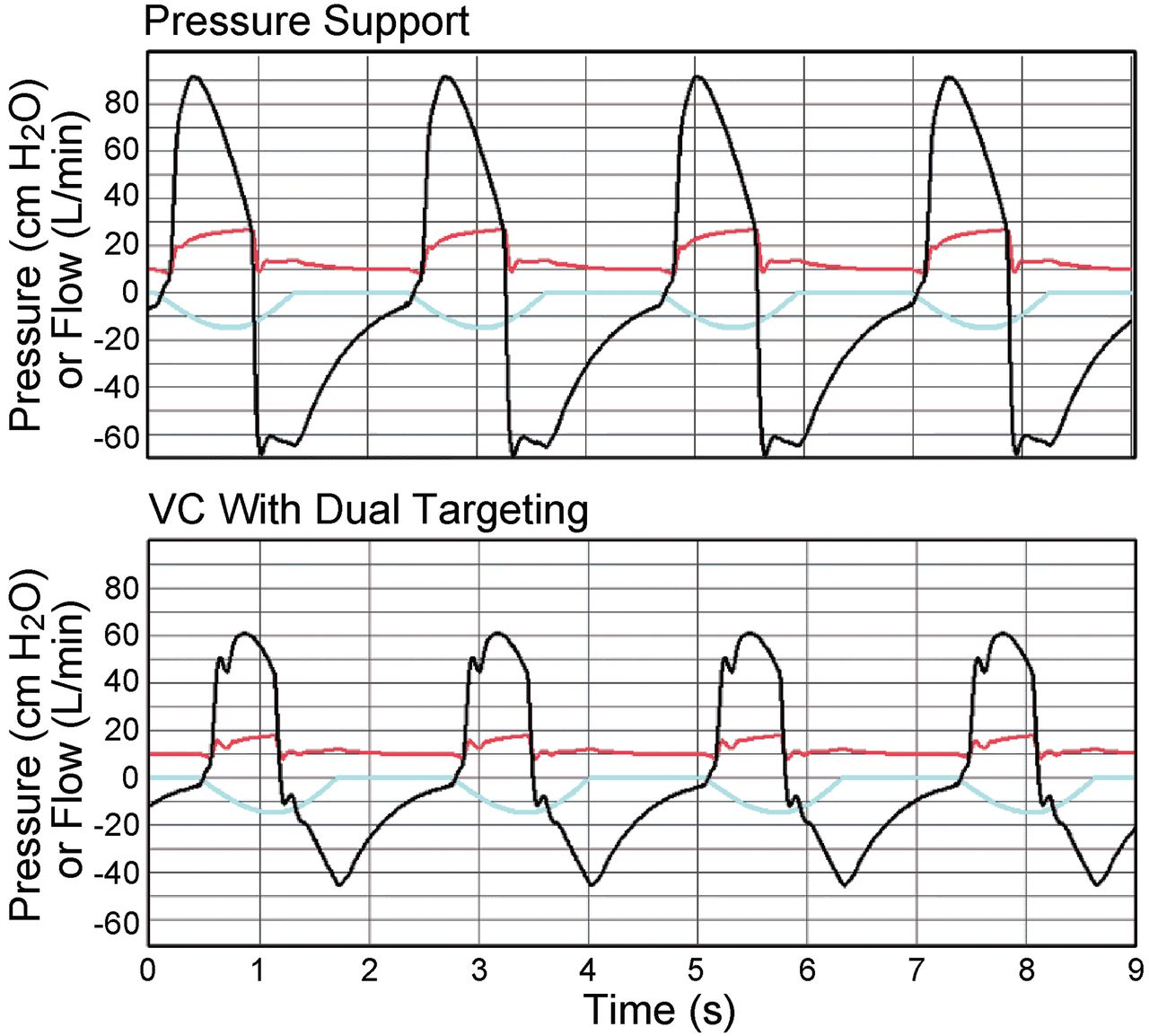
Pressure and flow waveforms during Pressure Support compared to volume control continuous mandatory ventilation (VC-CMV) with dual targeting during active breathing. Although dual targeting increases flow, compared to set-point targeting, it does not approach the flow available in Pressure Support in this particular model. Black = flow. Red = airway pressure. Blue = simulated muscle pressure.
The Effect of Targeting Scheme on Peak Inspiratory Flow During Volume Control Ventilation With Set-Point and Dual Targeting Compared to Pressure Support in an Active Lung Model*
Discussion
Significant differences in VT and flow delivery were found among targeting schemes. In our laboratory experiment a passive lung model was used to simulate a patient with no spontaneous inspiratory effort. During VC with both set-point and dual targeting, if the patient (or in the case of our experiment, the lung model) has no spontaneous effort, the ventilator will deliver a VT at the expected amount set by the operator. We were able to confirm the explanation provided by the operator's manual for the Servo-i. This manual states that if a patient makes an effort that generates a drop in pressure from baseline of < 3 cm H2O, the ventilator will behave in a manner identical to that of a patient who makes no spontaneous effort. In the passive lung model we observed subtle differences in the delivered VT during VC, despite the same VT setting. These differences may have been due to factors such as differences in ventilator calibration and differences in patient circuit compliance compensation algorithms. Also, the lung simulator was set to record variables as measured, and did not apply compensation for physiologic conditions (ie, body temperature and pressure saturated, BTPS), but the ventilators deliver gas corrected for BTPS. However, these factors are irrelevant for this experiment, as each ventilator served as its own control and we were interested only in the changes in VT associated with the way the targeting schemes responded to simulated inspiratory effort.
The active lung model was used to simulate an inspiratory effort that was large enough to cause a drop in inspiratory pressure of at least 3 cm H2O, triggering a mandatory breath during CMV and a spontaneous breath during Pressure Support. We observed that dual targeting during VC with active breathing allowed for an increased VT (77.1 mL more than operator set VT), compared to set-point (37.3 mL more than operator set VT), but not as much as Pressure Support (406.1 mL more than operator set VT). A change in VT of 77 mL with dual targeting represents an 18% increase in minute ventilation. That could, for example, mean a difference between a PaCO2 of 50 mm Hg and one of 41 mm Hg, which would probably be considered clinically important. A larger inspiratory effort would yield even larger effects. The increase in volume was expected for dual targeting and for pressure support. Figure 3 shows 4 distinct flow waveforms and thus 4 different VT delivered by the set-point targeting scheme, despite having operator preset values for volume and flow. We speculate that this behavior is related to the ventilator's circuit compliance compensation algorithm.12
Along with increasing inspiratory flow and volume in response to patient demand, both targeting schemes also increased the inspiratory time slightly during VC. This increase was negligible, and we speculate that it would have little effect on patient-ventilator synchrony in the adult critical care setting. Nevertheless, auto-triggering occurred with set-point targeting but not with dual targeting, which clinically can have an important effect on patient-ventilator synchrony. This observation demonstrates a potential clinical advantage of dual targeting, in that, with sufficient effort, the breath is patient cycled, which results in a mechanical inspiratory time more in synch with the patient's neural inspiratory time. The corresponding disadvantage of set-point targeting is that the operator presets arbitrary targets, including inspiratory time, that may or may not happen to synchronize with patient demands. The consequences of asynchrony include an increased work of breathing, patient discomfort, increased need for sedation, and confusion during the weaning process.14 These consequences may have a negative impact on the weaning process, which may ultimately prolong the length of ventilator support, ICU and hospital lengths of stay, as well as a potential for increased mortality.15
The effects on inspiratory flow further exemplify how differences in targeting schemes can influence patient-ventilator interaction. Inspiratory flow substantially increased during VC with dual targeting; more than set-point targeting, but not as much as Pressure Support. The increase in flow in Pressure Support compared to VC-CMV occurs for at least 2 reasons. First, Pmus adds to the set inspiratory pressure (Pvent) to create a larger pressure gradient between the airway opening and the lungs driving inspiratory volume, whereas with VC the airway pressure and hence the pressure gradient drops with inspiratory effort (ie, Pmus subtracts from Pvent in VC modes but adds to Pvent in PC modes). Second, the duration of Pmus is long enough to extend the inspiratory time in Pressure Support, compared to a preset inspiratory time with PC-CMV or volume modes; pressure acting for a longer time produces a larger VT. Figure 5 compares Pressure Support to VC with dual targeting. Note that while dual targeting responded to the demand for increased inspiratory flow, under these experimental conditions Pressure Support offered a higher peak flow and VT for the same inspiratory effort. Other settings for VC would yield different peak flow results.
One limitation of this study was that it used a simulated patient. This simulation did not reproduce the biological variability in resistance and compliance seen clinically with patients. This restricts the range of results we could measure, but, on the other hand, allowed for reproducible measurements. Also, given the popularity (in our experience) of using a descending ramp (aka, decelerating) wave for VC, one could question why we use a squared wave flow pattern. We chose to use a square wave on the PB 840 because that is the only choice on the Servo-i, and we wanted comparable results. According to the PB 840 manual, “If VT and V̇max are held constant, … inspiratory time approximately doubles when flow pattern changes from square to descending ramp.” Therefore, we could expect that, given our experimental setup, using a descending ramp flow may have decreased the double-trigger problem, due to the even longer preset inspiratory time relative to the simulated neural inspiratory time (ie, the Pmus Increase % setting on the ASL 5000). It is more difficult to predict the effect on actual VT: the pressure waveform would have been different, and there is a complex interaction between pressure and volume delivery imposed by the compliance compensation algorithm of the PB 840.12
Conclusions
In a lung model, dual targeting during VC ventilation allowed increased VT and avoided double triggering, compared to set-point targeting. Both of these effects are expected to improve patient-ventilator synchrony during actual clinical use. Although VT and flow increased with dual targeting, it was not as profound as that seen with PSV under these particular simulated conditions. Evaluating the manner in which the targeting scheme affects breath delivery may have important implications for clinical practice. An understanding of how a breath is delivered with different targeting schemes may assist practitioners in understanding how alterations in respiratory drive, timing, respiratory muscle pressure, and respiratory system mechanics influence the interaction between the patient and the ventilator.
Footnotes
- Correspondence: Teresa A Volsko MHHS RRT FAARC, Respiratory Care, Akron Children's Hospital, One Perkins Square, Akron, Ohio 44308. E-mail: TVolsko{at}chmca.org.
Mr Chatburn has disclosed relationships with Dräger, Hamilton, CareFusion, Covidien, Newport, IngMar, Radiometer America, Breathe Technologies, and the Alpha-1 Antitrypsin Foundation. The other authors have disclosed no conflicts of interest.
Mr Hoffman presented a version of this paper at the Open Forum of the AARC Congress 2011, held November 5–8, 2011, in Tampa, Florida.
- Copyright © 2012 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}