

Abstract
BACKGROUND: Pressure support ventilation (PSV) should be applied so that the inspiratory muscles are unloaded appropriately. We developed a computerized advisory system that assesses the load on the inspiratory muscles to spontaneously inhale, reflected by the automatically and noninvasively measured work of breathing per minute, and tolerance for that load, reflected by spontaneous breathing frequency and tidal volume, in a fuzzy-logic algorithm that provides recommendations for setting PSV. We call this a load and tolerance strategy for determining PSV.
METHODS: In a clinical validation study, we compared the recommendations from our PSV advisory system to the recommendations of experienced critical-care Registered Respiratory Therapists (RRTs) for setting PSV in patients with respiratory failure. With 76 adult patients in a university medical center surgical intensive care unit receiving PSV, a combined pressure/flow sensor, positioned between the endotracheal tube and patient Y-piece, sent measurements to the PSV advisory system. We compared the advisory system's recommendations (increase, maintain, or decrease the pressure support) to the RRTs' recommendations at the bedside.
RESULTS: There were no significant differences between the RRTs' and the advisory system's recommendations (n = 109) to increase, maintain, or decrease PSV. The RRTs agreed with 91% of the advisory system's recommendations (kappa statistic 0.85, P < .001). The advisory system was very good at predicting the RRTs' pressure support recommendations (r2 = 0.87, P < .02).
CONCLUSIONS: A load and tolerance strategy with a computerized PSV advisory system provided valid recommendations for setting PSV to unload the inspiratory muscles, and the recommendations were essentially the same as the recommendations from experienced critical-care RRTs. The PSV advisory system operates continuously and automatically and may be useful in clinical environments where experts are not always available.
- work of breathing
- mechanical ventilation
- pressure support ventilation
- acute respiratory failure
- respiratory monitoring
- artificial neural networks
Introduction
A goal of pressure support ventilation (PSV) is to appropriately unload the inspiratory muscles of patients with compromised pulmonary function and respiratory failure.1–3 The inspiratory muscles become loaded due to decreased respiratory system compliance and/or increased respiratory system resistance. The amount of inspiratory positivepressure assist applied with PSV is typically determined by observing the patient's spontaneous breathing pattern. The inspiratory muscle load, which can be assessed by work of breathing per minute (WOB/min), is thought to be appropriate when the spontaneous breathing frequency (f) and tidal volume (VT) are in clinically acceptable ranges, a comfortable breathing pattern is present, and accessory inspiratory muscles (eg, sternocleidomastoid) are not active. Because inspiratory muscle load and breathing-pattern data do not always correlate when applying PSV,2,3 another approach is to consider using measured values for WOB/min, f, and VT, and then using a portable computerized bedside monitor to assess the interrelationships of these values and formulate recommendations for setting PSV.
Changes in the patient's pulmonary mechanics and peak inspiratory flow rate may require a change in PSV, but highly trained, skilled clinicians may not always be available to make the assessments to properly set PSV. For these situations we propose an open-loop, computerized PSV advisory system that automatically assesses the breathing load on the inspiratory muscles (WOB/min) and tolerance for that load (f and VT) and provides recommendations for increasing, maintaining, or decreasing PSV.
Previously, we performed a multi-site clinical validation study in which we compared the recommendations of critical-care attending physicians to the recommendations of our PSV advisory system for setting PSV in patients with respiratory failure.4 The PSV advisory system provided valid recommendations for setting PSV to appropriately unload the inspiratory muscles, which were as good as the clinical judgment of attending physicians. Another group of clinicians who may make recommendations for setting PSV is critical-care Registered Respiratory Therapists (RRTs). In some hospitals RRTs are delegated, by authority of an attending physician, to make recommendations and changes to PSV settings within a specific range, and to wean patients from ventilatory support, as articulated in RRT-driven weaning protocols, for example. In other situations, experienced critical-care RRTs may be tasked to guide ventilatory management once a management algorithm is agreed upon between RRT leadership and the intensive care unit (ICU) attending medical staff. Thus, we conducted this follow-up study to compare the clinical judgment of critical-care RRTs in setting PSV to the recommendations from the PSV advisory system. We hypothesized that the PSV advisory system would supply PSV recommendations comparable to those chosen by the RRTs.
Methods
Approval was obtained from the institutional review board at the University of Florida at Shands Hospital to conduct the study in the surgical ICU. We enrolled 76 adult patients intubated or tracheostomized (tube inner diameter range 6.0–8.5 mm) with respiratory failure from various etiologies (pneumonia, pulmonary edema, sepsis, congestive heart failure, and subarachnoid hemorrhage) in the maintenance and weaning phases of ventilatory care (Table 1). Nine patients had direct lung injury from penetrating blunt chest trauma, and 6 had COPD. All the patients were breathing spontaneously, receiving PSV, receiving sedation and analgesia as needed, and hemodynamically stable. Excluded were patients who were hemodynamically unstable (eg, mean arterial blood pressure range 40–80 mm Hg, with irregular changes in heart rate and/or arrhythmias); heavily sedated (eg, high level of opioids, causing substantial changes in f and VT); or with irregular breathing patterns (eg, closed-head injury with sudden increases and decreases in f and VT).
Patient Data* at Enrollment (n = 76)
All the patients were ventilated with the same type of ventilator (840, Puritan-Bennett, Pleasanton, California), set in the PSV and PEEP modes, which we combined with synchronized intermittent mandatory ventilation (SIMV) set at 2 breaths/min and a VT of 6–8 mL/kg ideal body weight. It is a patient-care policy in our surgical ICU to employ SIMV at a minimum of 2 breaths/min when using PSV and PEEP, and our institutional review board required that we conform to all existing patient-care policies, so we used SIMV, with a decelerating inspiratory flow waveform. For PSV we set the “% rise” setting in the range 60–80%. This setting controls the ventilator's flow rate output during inhalation and affects the rate of pressure rise (ie, the interaction of the ventilator's flow rate output and patient's inspiratory flow rate demand affect the rate of pressure rise or shape of the pressure profile during a pressure-supported breath).5 With all patients we set the expiratory sensitivity setting (breath-termination criterion) at 25%.
Two components constitute the open-loop PSV advisory system: a commercially available respiratory monitor (NICO, Respironics, Wallingford, Connecticut), and a laptop computer. A combined pressure/flow/carbon dioxide sensor, positioned between the endotracheal tube and the patient Y-piece, directs data to the respiratory monitor for measurement of f, VT, exhaled minute ventilation, PSV, PEEP, and end-tidal partial pressure of carbon dioxide (PETCO2) (Fig. 1). Compliance and resistance of the respiratory system were calculated with the least-squares method.6 SpO2 readings were collected with a finger sensor. PETCO2 and SpO2 data were monitored to ensure that the patients were appropriately ventilated and oxygenated.

Open-loop pressure support ventilation (PSV) advisory system. Data from the pressure and flow sensors at the Y-piece go to the respiratory monitor, then to the PSV advisory system software, which also collects data from the ventilator. The PSV advisory system's artificial neural network software calculates the noninvasively measured work of breathing per minute (WOBN/min), and the fuzzy-logic inference system software uses the WOBN/min, spontaneous breathing frequency (f), and tidal volume (VT) to form its recommendation for setting PSV to appropriately unload the inspiratory muscles. In this load and tolerance strategy the load parameter, WOBN/min, reflects the load on the inspiratory muscles during spontaneous inhalation, and the tolerance parameters, f and VT, reflect the tolerance for the load on the inspiratory muscles. In this figure the PSV advisory system determined that the current pressure support setting of 10 cm H2O is insufficient because WOBN/min is too high (17 J/min) and tolerance for that load is borderline (f is 32 breaths/min and VT is low at 5 mL/kg ideal body weight), so the system recommends increasing PSV.
Data from the monitor go to the laptop computer where the PSV advisory system software (Convergent Engineering, Gainesville, Florida) operates an artificial neural network for immediate calculation of noninvasively measured WOB/min (WOBN/min)3 and a fuzzy-logic inference system that processes the WOBN/min, f, and VT information to assess the load on the inspiratory muscles to inhale (WOBN/min) and the tolerance for that load (f and VT) and provides recommendations to increase, maintain, or decrease the pressure support. We refer to this as a load and tolerance strategy (see Fig. 1). Fuzzy logic is a process of using probability distributions instead of simple “yes/no” decisions, as in a simple rule-based system, to drive the ventilator decision making.7,8 The WOBN/min data were highly correlated (r = 0.91, P < .02) with invasively measured WOB/min (from esophageal pressure measurements) and were considered a very good predictor of invasively measured WOB/min in adults treated with PSV.3 WOBN/min reflects the total load on the inspiratory muscles, which includes the elastic load of the respiratory system and resistive loads of the airways, endotracheal tube, and ventilator apparatus. A limitation of WOBN/min is that it cannot differentiate these component loads.
Artificial neural networks—a branch of artificial intelligence—have been used for medical applications9–12 (eg, breathing-pattern recognition during spontaneous breathing and PSV).11 Artificial neural networks are a class of mathematical models that are biologically inspired computer programs designed to simulate the way in which the human brain processes information.13,14 An artificial neural network can detect complex nonlinear relationships between dependent and independent variables in data that a human brain may fail to detect. They acquire knowledge by detecting patterns and relationships to facilitate learning; they are trained through experience. Basically, an artificial neural network learns from data and captures the knowledge contained in the data. An artificial neural network is formed by hundreds of single units (artificial neurons, or processing elements) connected with coefficients or weights (analogous to synaptic connections in the central nervous system), which constitute the neural system, and are organized into layers. The power/intelligence of neural computations is achieved from connecting neurons in a network. During training, the inter-unit connections are optimized until the errors in predictions are minimized and the artificial neural network reaches a specified level of accuracy. Once the network is trained, it can be given new input information to predict the output. A “multi-layer perceptron” (the most common type of artificial neural network) can be thought of as a combination of the weighted sum of a number of logistic regression models. Each logistic regression model (a “perceptron” in neural network terminology) has its own set of weights, and its output is weighted and added to the outputs of the other perceptrons to create the final prediction. WOB/min is the predicted variable of the artificial neural network in our PSV advisory system.
The training of our artificial neural network was previously described.3 Five input elements (predictors) are used:
Spontaneous minute ventilation (not including SIMV breaths) correlates directly with WOB/min.
Increased intrinsic PEEP is associated with increased WOB/min, and vice versa.
Lower inspiratory trigger pressure depth just before the ventilator triggers during PSV is associated with increased WOB/min, and vice versa.
Lower inspiratory flow rise time during a PSV breath is associated with increased WOB/min, and vice versa.
Higher respiratory muscle pressure (pressure = (VT/respiratory system compliance) + (inspiratory flow rate × respiratory system resistance)) is associated with increased WOB/min, and vice versa.15,16
One goal of the PSV advisory system is to maintain WOBN/min, f, and VT in the green ranges shown in Figure 1, which were derived, in part, from normal WOB values,3,15 a WOB outcome study,2 and our clinical experience.3 In adults the normal range of WOB/min is 4–8 J/min.15 Based on 15 years of experience measuring WOB in patients receiving ventilatory support, adults treated with PSV tolerate a maximum WOB/min of up to about 10–12 J/min. WOB/min values greater than 12–15 J/min in adults are not well tolerated and require a higher pressure support level. In adults treated with PSV it was found that WOB of 2–8 J/min was well tolerated.3 Another clinical study2 reported that WOB maintained in a fairly normal range during PSV was well tolerated.
Our PSV advisory system's target f and VT ranges are congruent with those applied to spontaneously breathing adults receiving PSV: 10–25 breaths/min, and 6–8 mL/kg, respectively.1,17 It is reasonable to apply PSV so that inappropriately low f (eg, 4–6 breaths/min) or high f (eg, 30–40 breaths/min) and low VT (eg, < 4 mL/kg) or high VT (eg, > 12 mL/kg) do not occur. The advisory system treats the wider WOBN/min, f, and VT ranges (the yellow areas in Figure 1) as cautionary. The advisory system assesses the probability of inspiratory muscle load (WOBN/min) and tolerance (f and VT) parameters varying in relation to one another in all ranges, and then provides an appropriate recommendation to increase, maintain, or decrease PSV. The system uses a 5-minute averaging filter for updating its recommendation.
PSV was set initially as ordered by the attending physicians. Subsequently, the RRTs' pressure support recommendations were permitted during the study. At periodic intervals the RRTs were asked to evaluate the patient to determine if PSV should be increased, maintained, or decreased. Their recommendations were based on using the traditional approach of assessing spontaneous breathing-pattern data (ie, f 15–25 breaths/min, VT 6–8 mL/kg ideal body weight), no sternocleidomastoid muscle contraction, and appearance of comfortable breathing. The RRTs were blinded to the measured respiratory data and the advisory system's recommendations.
PEEP and FIO2 settings, determined by the attending physicians (see Table 1), were held constant during the study period, which was over an 8-hour work shift. There were no clinically important differences in PEEP, PETCO2, or SpO2 at baseline or during the study, and no clinically important variations in hemodynamic parameters in any patients throughout the study.
We assessed the relationship between PSVs set by the clinicians and PSVs recommended by the advisory system. When the RRTs recommended an increase or decrease in PSV, generally the change was by 5 cm H2O from the current setting. When the advisory system recommended “Increase PSV” or “Decrease PSV,” this was interpreted to mean a change of 5 cm H2O up or down, respectively, from the current setting. With this understanding, the RRTs' recommended PSV settings were regressed with the recommended settings from the PSV advisory system.
We analyzed the data with chi-square, regression analysis, and the kappa statistic.18 Alpha was set at .05 for statistical significance.
Results
PSV ranged from 5 cm H2O to 20 cm H2O during the study. The advisory system made 109 recommendations to increase, maintain, or decrease PSV. There were no clinically important differences between the RRTs' and the advisory system's recommendations (chi-square = 0.49, P = .78) (Table 2). The mean total agreement between all the RRTs' and the advisory system's recommendations was 91% (kappa statistic ± standard error = 0.85 ± 0.05, P < .001). A kappa statistic value of 0.81–1.0 is considered almost perfect agreement.18 There were about 3 times as many recommendations to decrease PSV as to maintain it (P = .01), about 5 times as many recommendations to decrease PSV as increase it (P = .01), and about twice as many recommendations to maintain PSV as to increase it (P = .02) (see Table 2).
Recommendations Made by the Ventilator Advisory System, Compared to Recommendations Made by the RRTs for Setting PSV*
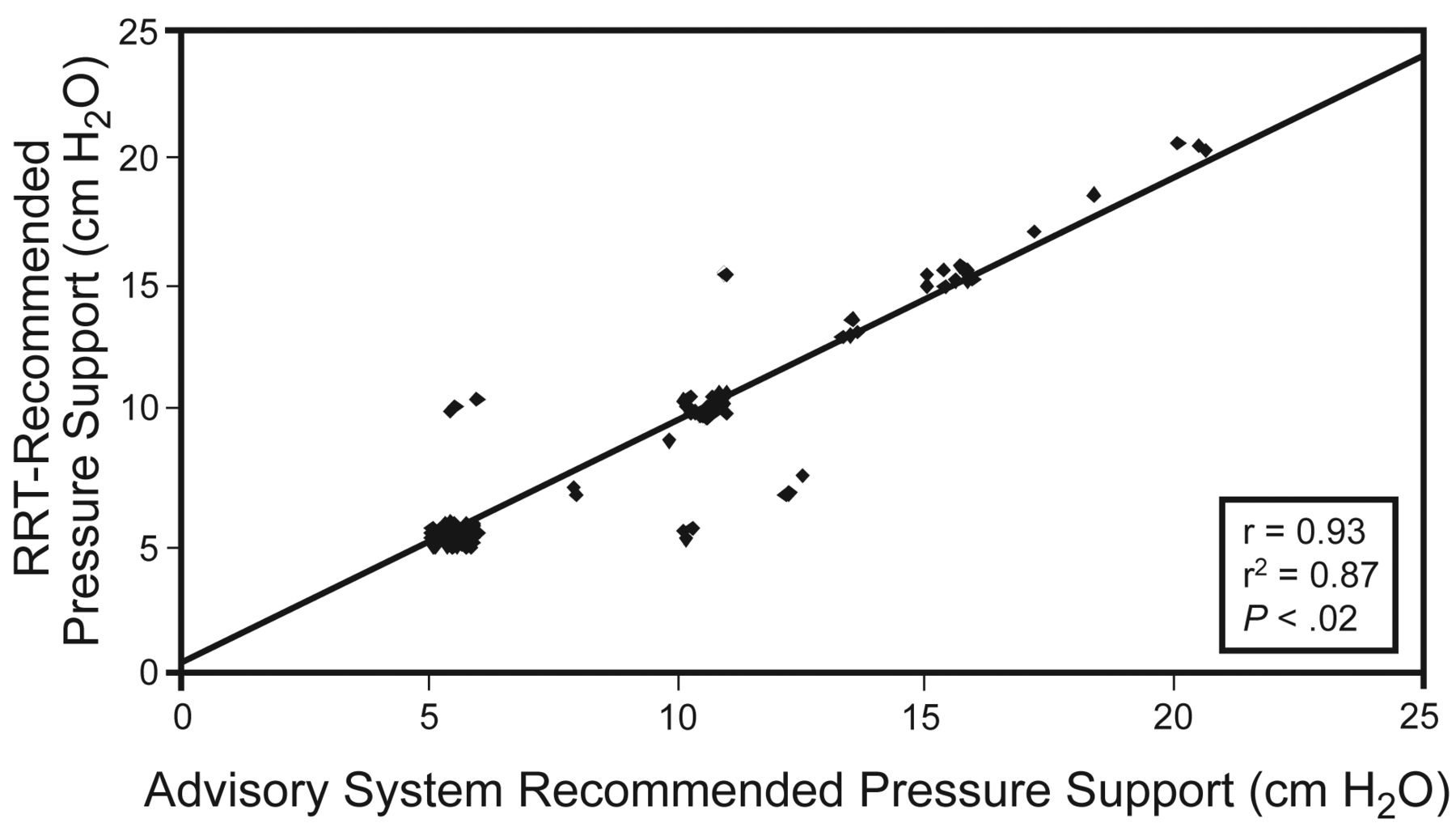
There was an excellent positive correlation between PSV ordered and that recommended by the advisory system: r = 0.93, P < .02, r2 = 0.87. The advisory system predicted or explained 87% of the variance in the RRTs' recommendations (Fig. 2).

Relationship between the Registered Respiratory Therapists' (RRTs') recommendations and the automated advisory system's recommendations on adjusting the pressure support level during pressure support ventilation (PSV). The clusters of data points (eg, at 5, 10, 12, and 15 cm H2O) represent considerable overlap of many of the recommendations at those levels. There was an excellent and significant correlation between the RRTs' and the PSV advisory system's recommendations (r = 0.93), and the advisory system was a very good predictor of the pressure-support level recommended by the RRTs (r2 = 0.87).
The WOBN/min values range was 1.2–18.6 J/min. The RRTs recommended “Maintain PSV” (implying appropriate inspiratory muscle loading) 27 times, and the advisory system agreed 25 times (93% agreement). Under that condition the mean ± SD WOBN/min was 6.0 ± 4 J/min.
Discussion
An inspiratory muscle load (WOBN/min) and tolerance (f and VT) strategy in an open-loop, computerized PSV advisory system provided valid recommendations for setting PSV in adults with respiratory failure. The advisory system's recommendations were congruent with those of the critical-care RRTs evaluating patients at the bedside 91% of the time (see Table 2). The RRTs recommended decreasing PSV by a 3-to-1 margin compared to maintaining PSV, and by a 6-to-1 margin compared to increasing PSV, and the advisory system's recommendations were in accordance with that recommendation trend. Our load and tolerance strategy appears to be appropriate in view of the high level of agreement between the recommendations of the advisory system and the RRTs. At no time did the advisory system recommend a change in the opposite direction to that of the RRTs.
Concerning the 9% disagreement for all recommendations, at times there may have been philosophical differences between the thinking of some of the RRTs and the advisory system's fuzzy-logic inference system. Or some RRTs may have misinterpreted a patient's breathing pattern data and inferred a need to maintain the current PSV setting while the advisory system recommended decreasing it. Although the difference was very small, that was the most common disagreement (see Table 2). Another explanation may be a clinical decision to totally unload the inspiratory muscles with higher pressure support (> 20 cm H2O) or to exercise them with lower pressure support (5 cm H2O). In either case, the PSV advisory system is not privy to a clinician's intentions and is incapable of “knowing” decisions to rest or exercise inspiratory muscles. This can cause disagreements, because the advisory system is unable to assimilate these types of decisions into its recommendations for setting PSV.
The load and tolerance operational strategy of our open-loop system is novel (see Fig. 1). In one respect, it determines WOB/min or power of breathing automatically, obviating esophageal balloon catheter and complex equipment.3 This method greatly simplifies measurement of WOB, especially during prolonged ventilatory support, where it may be impractical to employ an esophageal balloon catheter. WOB/min reflects the load on the inspiratory muscles to spontaneously inhale,15,19 while f and VT reflect a patient's tolerance for that load. Breathing load and tolerance are different but related concepts and should be used together. We believe that assessing both the inspiratory muscle load and the tolerance for that load (rather than assessing only patient tolerance) provides a more comprehensive understanding of a patient's ability to breathe spontaneously. Both concepts are important, and neither should be ignored. Our advisory system uses inspiratory muscle load and tolerance data in a complementary manner to determine a recommended pressure support level.
Other open-loop ventilatory advisory systems have been described for adults20,21 and neonates.22 With the neonatal ventilatory advisory system there was high agreement between the clinicians' and the advisory system's recommendations for setting the ventilator to treat ventilation and oxygenation abnormalities. In another study, an approach akin to an open-loop PSV system was employed, in which the response or input variable was WOB per breath, directly measured with an esophageal balloon catheter, and the output variable was PSV.2 The clinicians maintained WOB per breath in a specific and fairly normal physiologic range by increasing or decreasing PSV as needed. When WOB per breath was maintained in that range with PSV, adults weaned faster than with the traditional method.
Intelligent decision-support systems for mechanical ventilation employing closed-loop control have been recommended.23 Closed-loop feedback systems for controlling PSV have been described.24–26 For an intelligent decision-support system closed-loop ventilator to be useful, it should be effective, safe, and easy to use at the patient's bedside.23 Based on the findings from the present study, our open-loop system meets those criteria: it was effective in recommending appropriate PSV settings, appears to be safe, in that its recommendations were validated, and because it is automatic, it is easy to use. Our open-loop system may be the basis for a closed-loop ventilator feedback system that uses WOBN/min and spontaneous f and VT data as input variables to be directed back to a ventilator and used for automatically adjusting PSV.
Our PSV open-loop advisory system differs from SmartCare (Dräger Medical, Lübeck, Germany),25 which is a closed-loop system in that it assesses WOB/min, the load on the inspiratory muscles to spontaneously inhale, f, and VT, which reflect only the tolerance for the load. SmartCare uses f, VT, and PETCO2 as feedback or input data to automatically regulate PSV to maintain f between 12 and 28 breaths/min, VT > 0.3 L (or 0.25 L and if the patient weighs < 55 kg) and maintain PETCO2 < 55 mm Hg (or < 65 mm Hg if the patient has COPD). A potential shortcoming of that approach may be that WOB/min is not measured and taken into consideration when automatically regulating PSV. Because WOB/min is not measured, neither SmartCare nor the clinician knows whether the load on the inspiratory muscles is too high or low, so SmartCare might apply an inappropriate amount of PSV, which could prolong weaning. This may explain, in part, why reductions in weaning duration initially demonstrated with SmartCare were not confirmed when it was compared to weaning managed by experienced clinicians.25
Our system differs also from proportional assist ventilation (PAV+, Puritan Bennett, Pleasanton, California),27 which is a closed-loop system designed to automatically increase or decrease the inspiratory assist pressure in proportion to the patient's spontaneous WOB per breath, which is not measured. PAV+ uses a simple equation related to respiratory muscle pressure to calculate WOB per breath. Our approach was to employ an artificial neural network, which is a substantially more complex mathematical model that uses coefficients calculated from a clinically collected data set. A study of patients on PAV+ showed that the WOB-per-breath data displayed on the ventilator were inaccurately low, calling that method into question.28 This may offer some explanation of a clinical study that reported excessive WOB when PAV+ was applied at percentage support settings lower than 30%.27
A possible limitation of the present study is that to fully validate the advisory system a similar study with a wider variety of patient conditions and performed over the total duration of ventilatory support may be needed.
Conclusions
Our open-loop computerized PSV advisory system's recommendations on increasing, maintaining, or decreasing PSV were in close agreement with the RRTs' recommendations. The load and tolerance strategy in the advisory system automatically provides valid recommendations for setting PSV to appropriately unload the inspiratory muscles, that are as good as the clinical judgment of experienced critical-care RRTs. The advisory system is automatic and continuous, so in clinical situations with limited staff (eg, large ICUs, remote work areas), where skilled critical-care RRTs are not always available to perform bedside assessments, the system may be useful in recommending appropriate PSV settings. We recommend clinical outcomes studies to further evaluate this PSV advisory system, such as a study of its usefulness in patients with more difficult forms of respiratory failure.
Footnotes
- Correspondence: Michael J Banner PhD RRT, Department of Anesthesiology, University of Florida College of Medicine, Box 100254, Gainesville FL 32610. E-mail: mbanner{at}anest.ufl.edu.
-
The authors have disclosed a relationship with Respironics and Convergent Engineering.
-
Steven Bonett RRT presented a version of this paper at the 54th International Respiratory Congress of the American Association for Respiratory Care, held December 13-16, 2008, in Anaheim, California.
-
See the Related Editorial on Page 359
- Copyright © 2011 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}