

Introduction
Community-acquired necrotizing pneumonia caused by methicillin-resistant Staphylococcus aureus (MRSA) has been reported with increasing frequency in children.1 MRSA pneumonia can be complicated by pleural effusion, empyema, pneumatoceles, respiratory failure, and bronchopleural fistula.1,2 Maintaining adequate gas exchange with conventional mechanical ventilation is often problematic in patients with pneumonia complicated with bronchopleural fistula. In this setting, high-frequency oscillatory ventilation (HFOV) may be more effective than conventional mechanical ventilation because it avoids cyclic stretching of lung and pleural tissue, thus increasing the likelihood that the bronchopleural fistula will spontaneously seal.3,4 We present the case of a previously healthy 8-month-old infant with community-acquired-MRSA pneumonia complicated by bronchopleural fistula, who failed conventional mechanical ventilation and was subsequently successfully supported with HFOV.
Case Summary
An 8-month-old, 7.5-kg female was admitted to the hospital with bilateral pneumonia requiring oxygen at 2 L/min via nasal cannula to maintain SpO2 ≥ 92%. Within 18 hours of hospitalization there was worsening of the right-lung infiltrates, and soon thereafter she developed a right-sided tension pneumothorax (Fig. 1), which was decompressed with a chest tube.
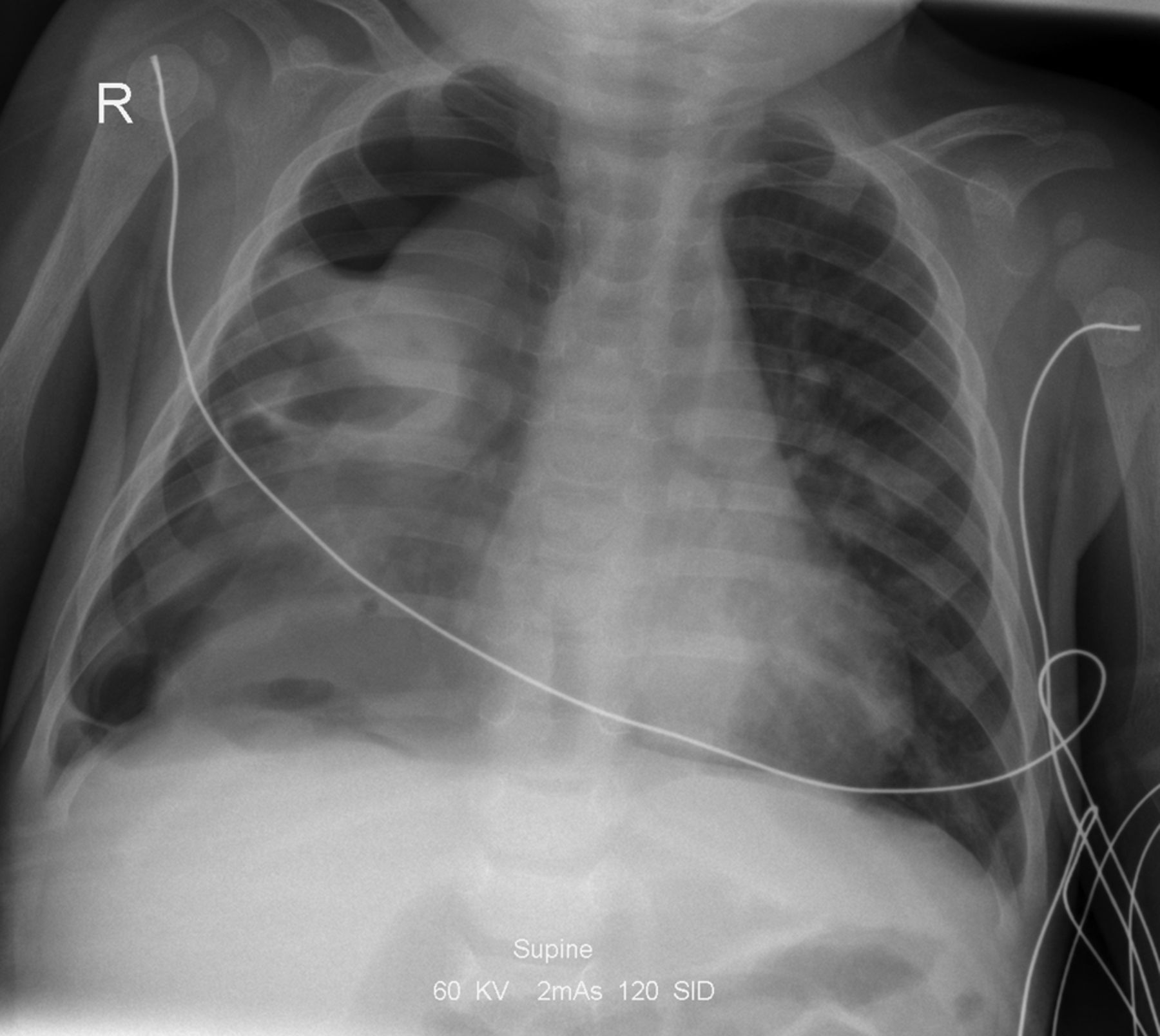
Chest radiograph within 18 hours of hospitalization shows right-lung infiltrates.
Three hours later she required intubation (size 4 uncuffed endotracheal tube [ETT]) due to progressive tachypnea (respiratory rate 85 breaths/min) and refractory hypoxemia. Initial ventilator settings were pressure-controlled continuous mandatory ventilation (CMV), peak inspiratory pressure (PIP) 20 cm H2O, PEEP 5 cm H2O, and FIO2 0.35. Within a short time it was necessary to increase FIO2 to 0.7, PIP to 28 cm H2O, and PEEP to 8 cm H2O to maintain SpO2 ≥ 93% and arterial pH > 7.30. The mean airway pressure on conventional mechanical ventilation was 15 cm H2O. Cultures of tracheal aspirate, pleural fluid, and blood were all positive for MRSA within 36 hours of hospitalization.
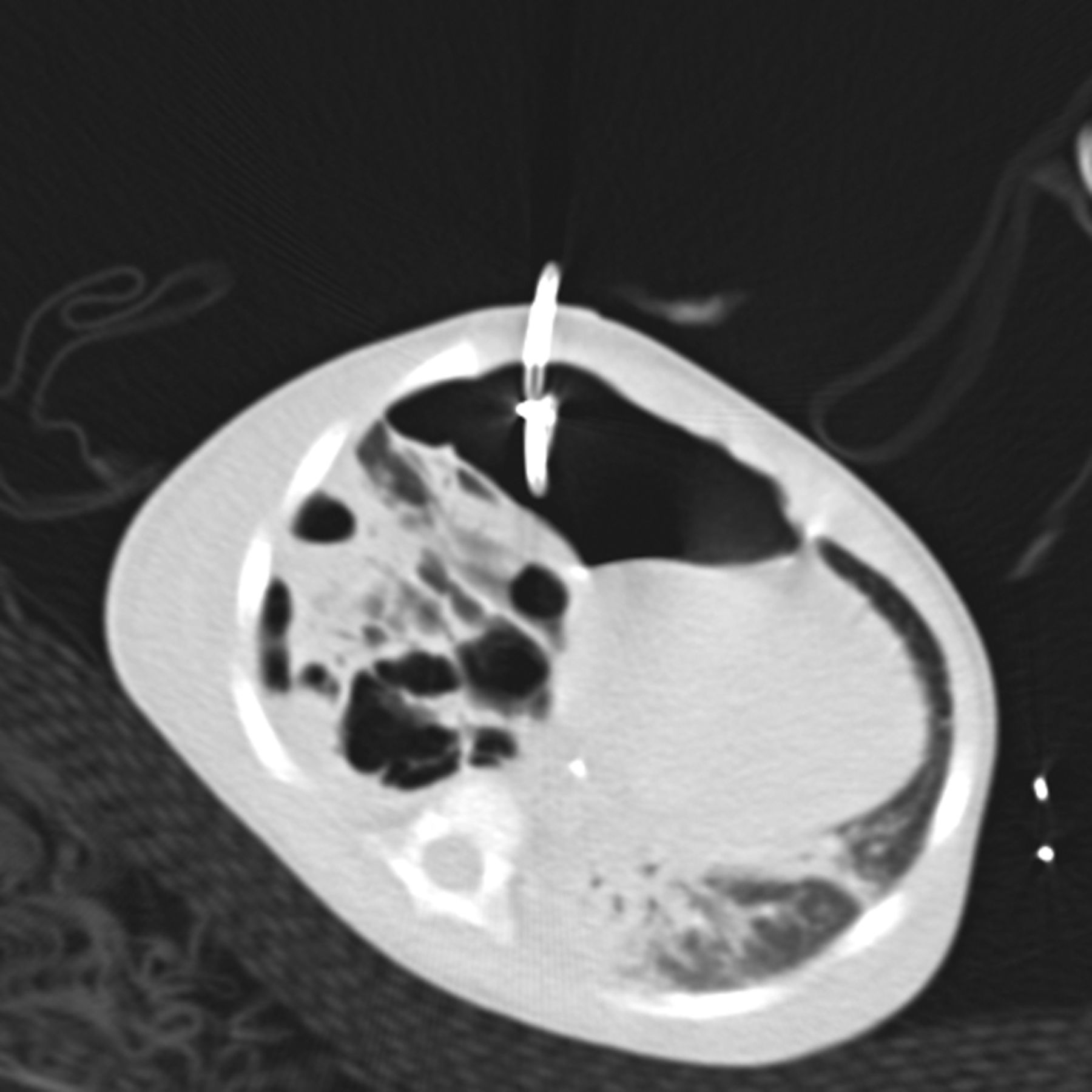
Over the subsequent 48 hours she exhibited episodes of desaturation to 80% and hypercarbia, which were not responsive to ventilator adjustments on conventional mechanical ventilation, or ETT suctioning. Echocardiogram showed no evidence of pulmonary hypertension; however, chest computed tomography revealed multiple pneumatoceles in the right hemithorax, with mediastinal shift to the contralateral side. She also exhibited significant hypotension, despite fluid therapy and inotropic support with intravenous epinephrine infusion. Two consecutive pigtail drains were inserted under computed-tomography guidance, and the drains substantially shrank the pneumatoceles (Fig. 2). Chest computed tomography also revealed extensive air-space disease consistent with necrotizing pneumonia.

Computed tomogram shows extensive air-space disease consistent with necrotizing pneumonia.
There was air leak with each ventilator breath in all the chest drainage systems, suggesting the presence of bronchopleural fistula. Since she was intubated with an uncuffed ETT, it was not possible to ascertain the exact volume of air leak from the chest tubes. Because the left lung was less extensively involved, we attempted a trial of unilateral (left) lung ventilation, by advancing the ETT intothe left main bronchus, using a flexible bronchoscope, but this was unsuccessful: SpO2 fell below 60%, without recovery until the ETT was pulled back into the lower trachea.
At this point we concluded that conventional mechanical ventilation could not adequately support her oxygenation and ventilation, so we conducted a trial of HFOV (3100A, SensorMedics, Yorba Linda, California), initiated at mean airway pressure of 18 cm H2O, frequency 6 Hz, and amplitude adjusted to maintain arterial pH > 7.30. The initial mean airway pressure was set 3 cm H2O greater than the mean airway pressure on conventional mechanical ventilation, consistent with the low-volume strategy recommended for management of air-leak syndromes with HFOV.5 Shortly after initiation of HFOV, SpO2 was ≥ 93% on FIO2 ranging from 0.3 to 0.6, and arterial pH was 7.31.
Over the subsequent 2 weeks she had episodes of substantial respiratory acidosis, which were managed with judicious use of intravenous sedation (midazolam and fentanyl), neuromuscular blockade (cisatracurium), increased amplitude (as high as 90 cm H2O), and/or decreased respiratory frequency (as low as 5 Hz). Mean airway pressure was lowered as tolerated, to decrease the risk of barotrauma and promote closure of the bronchopleural fistula. We adjusted the amplitude to maintain PaCO2 in the range 50–70 mm Hg and arterial pH ≥ 7.30. The ETT was suctioned every 4 hours as needed, with an in-line suction catheter. We avoided frequent suctioning and disconnection from the HFOV, to minimize alveolar derecruitment. When deemed necessary, we used a post-suctioning recruitment maneuver (increased the mean airway pressure to 20 cm H2O for 30 s, followed by reduction to the pre-suctioning level). Enteral nutrition (120 kcal/kg/d) was via nasogastric tube throughout the period of mechanical ventilation.
On HFOV day 21 the air leak from the chest drains had resolved for 48 hours, and we attempted transition to conventional mechanical ventilation (synchronized intermittent mandatory ventilation [SIMV]), but the attempt failed due to persistent hypoxemia (PaO2/FIO2 91 mm Hg) and the requirement for relatively high PIP (27–30 cm H2O) on SIMV. The chest radiograph at this time showed diffuse alveolar disease.
On HFOV day 29 she successfully transitioned to pressure-controlled SIMV, with PIP 18 cm H2O, PEEP 5 cm H2O, FIO2 0.35, respiratory rate 25 breaths/min, and pressure support 7 cm H2O. The chest tube and pigtail drains were removed one at a time, over 2 days. She was extubated 4 days later and placed on oxygen via high-flow nasal cannula (Vapotherm, Stevensville, Maryland), at 5 L/min. That oxygen flow was decreased over 4 days and then discontinued to room air.
During her illness she received a 4-week course of intravenous antibiotics (vancomycin and clindamycin for 2 weeks, and clindamycin and rifampin for 2 weeks). Repeat cultures of pleural fluid, blood, and tracheal aspirates were all negative 3 weeks following institution of intravenous antibiotics. She was successfully transferred from the pediatric intensive care unit to a pediatric ward on hospital day 37 and was discharged home in good condition on hospital day 39.
Discussion
Bronchopleural fistula is an open and aberrant communication between some portion of the bronchial tree and the pleural space, through which inspired gas enters the pleural space.4,6 Persistent bronchopleural fistula during mechanical ventilation can lead to pneumothorax and ventilation-perfusion mismatch.6 Since much of the inspired volume exits through the fistula rather than going to the alveoli, alveolar ventilation may profoundly decrease and cause moderate to severe respiratory acidosis.6
Pierson et al reported that the majority of 39 adult patients with bronchopleural fistula following traumatic lung injury could be treated with conventional mechanical ventilation in either the volume controlled CMV or volume controlled intermittent mandatory ventilation mode.6 However, the necrotizing nature of the pneumonia associated with community-acquired-MRSA7 may present a more difficult therapeutic challenge than bronchopleural fistula uncomplicated by infection—hence the failure of conventional mechanical ventilation and the need for HFOV in our patient.
HFOV has been successfully used in infants and children with acute respiratory failure associated with several types of air-leak syndrome, including pneumomediastinum and cystic lung disease.8–11 Furthermore, anecdotal reports suggest that HFOV may be effective in adults with bronchopleural fistula.3,4 Ha et al reported a 55-year-old with empyema who developed bronchopleural fistula following decortication.4 There was substantial air leak via the bronchopleural fistula with the high PIP on conventional mechanical ventilation, but HFOV was associated with much less air leak and improved oxygenation and ventilation in that patient.4 Poulin et al reported similar results in a 41-year-old female with lung cancer who developed bronchopleural fistula following pneumonectomy.12
Creel et al reported a case series of 11 children (age range 3–15 y) with community-acquired MRSA pneumonia admitted to a pediatric intensive care unit over a 6-year period; however, they did not report any cases of bronchopleural fistula or use of HFOV.13
We believe our patient was an unusual case of an infant with community-acquired MRSA pneumonia complicated by empyema and bronchopleural fistula. Conventional ventilation failed, but HFOV supported her until the bronchopleural fistula spontaneously closed. In this critically ill infant with necrotizing pneumonia and bronchopleural fistula, we selected a pH lower limit of 7.3 (rather than closer to 7.2) and an SpO2 lower limit of 93% (rather than upper-80s), which are higher than those accepted by most other institutions.5,8,9 Acceptance of more liberal lower limits for pH (a greater degree of permissive hypercapnia) and SpO2 in our patient might have allowed for lower peak and mean airway pressures, which might have decreased the risk of barotrauma.5,8,9
Measurement of exhaled volumes and estimation of alveolar ventilation are inaccurate in the presence of air leak with an uncuffed ETT. In retrospect, use of an appropriate-size cuffed ETT might have benefited our patient, since low-pressure, high-volume cuffs are associated with minimal complications,14 and would have allowed a more accurate estimation of the degree of air leak while the bronchopleural fistula was present. However, while a cuffed ETT would have allowed leak measurement, it probably would not have changed our patient's course of treatment.
Our patient was kept on HFOV for an additional 9 days following apparent resolution of the bronchopleural fistula. The first attempt to transition to conventional ventilation failed due to refractory hypoxemia caused by diffused alveolar disease and the need for relatively high PIP on conventional ventilation. At that point we continued HFOV for 2 reasons. First, although the bronchopleural fistula had resolved, we were not certain if the necrotic process that caused the fistula had resolved, so we feared fistula reoccurrence with the higher PIP of conventional ventilation. Second, the chest radiograph at that time showed persistent diffuse alveolar disease, and we were particularly concerned about exacerbating that process and the risk of pulmonary interstitial emphysema. Thus, the prudent course seemed to be continued HFOV to promote healing and resolution of both the fistula8,9 and the diffuse alveolar disease.15
Teaching Points
This case emphasizes the potential benefit of HFOV in an infant with air leak secondary to bronchopleural fistula associated with necrotizing pneumonia. Several therapeutic options have been reported for the management of bronchopleural fistulas in adults, including independent lung ventilation,16,17 interventional bronchoscopy, and closure of the bronchopleural fistula with various devices or materials,18–20 but those approaches were technically not possible in our patient.18–20 Our patient was not a candidate for lobectomy, because the necrotizing pneumonia process was not limited to one lobe.18–20 Furthermore, our trial of unilateral lung (left lung) ventilation failed, which left HFOV as the most logical intervention to deal with the failure of conventional ventilation.
HFOV may benefit patients with severe alveolar disease by avoiding cyclic stretching of the lungs and the development of pulmonary interstitial emphysema. The use of HFOV to treat pulmonary interstitial emphysema, in both infants21 and adults,15 has long been established. Further, a review of both animal and human studies strongly suggests that HFOV is protective in situations where development of diffuse alveolar disease is likely.22
Footnotes
- Correspondence: Rashed A Hasan MD, Pediatric Critical Care Services, Mercy Children's Hospital, University of Toledo, 2213 Cherry Street, Toledo MI 43608. E-mail: rashedh48{at}gmail.com.
-
The authors have disclosed no conflicts of interest.
- Copyright © 2011 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}