

Article Figures & Data
Figures
- Fig. 1.
Characteristics of a pressure-supported breath. In this example, the baseline pressure (ie, PEEP) is set at 5 cm H2O, and the pressure support is set at 15 cm H2O. The inspiratory pressure is triggered at point A by a patient effort, resulting in an airway pressure decrease. The rise to pressure (line B) is provided by the initial flow into the airway. If the initial flow is excessive, the initial pressure exceeds the set level (B1). If the initial flow is low, there is a slow rise to pressure (B2). The plateau of pressure support (line C) is maintained by control of flow. A smooth plateau indicates appropriate flow responsiveness to patient demand. Termination of pressure support occurs at point D and should coincide with the end of neural inspiration. If breath termination is delayed, the patient may actively exhale (the pressure rises above the plateau) (D1). If breath termination is premature, the patient may have continued inspiratory efforts (D2). (Adapted from Reference 18, with permission.)
- Fig. 2.
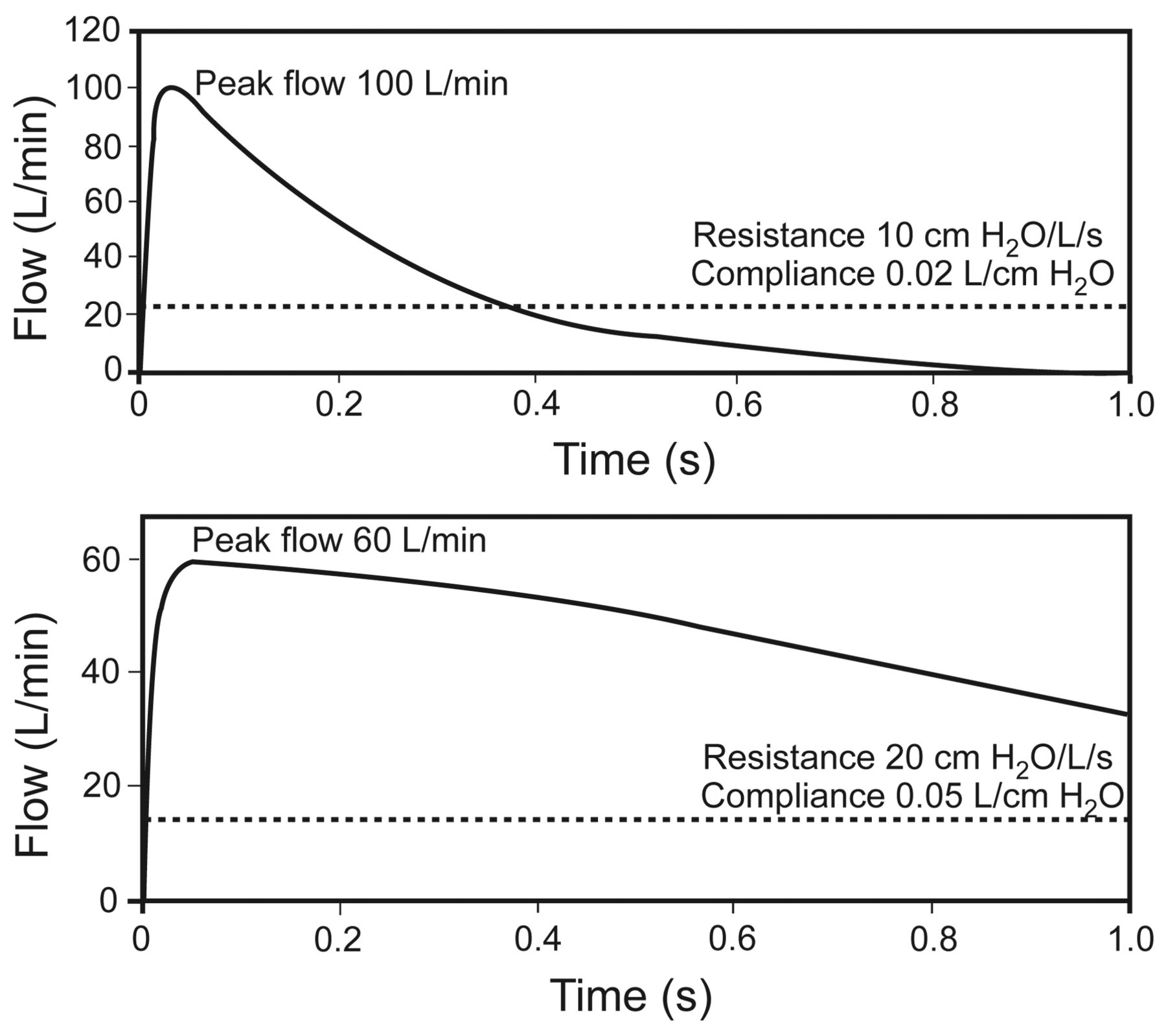
Effect of respiratory mechanics on cycling of pressure support from inhalation to exhalation. Flow cycling is set at 25% of the peak flow, as illustrated by the broken line. The upper panel represents the respiratory mechanics of a patient with restrictive lung disease. The lower panel represents the respiratory mechanics of a patient with obstructive lung disease. In each case the neural inspiratory time is 1.0 second. The breath terminates prematurely in the patient with restrictive lung disease, but the breath is prolonged in the patient with obstructive lung disease. Also note that the peak flow is greater in restrictive lung disease, and the pressure decrease is more rapid in restrictive lung disease. (Adapted from Reference 19.)
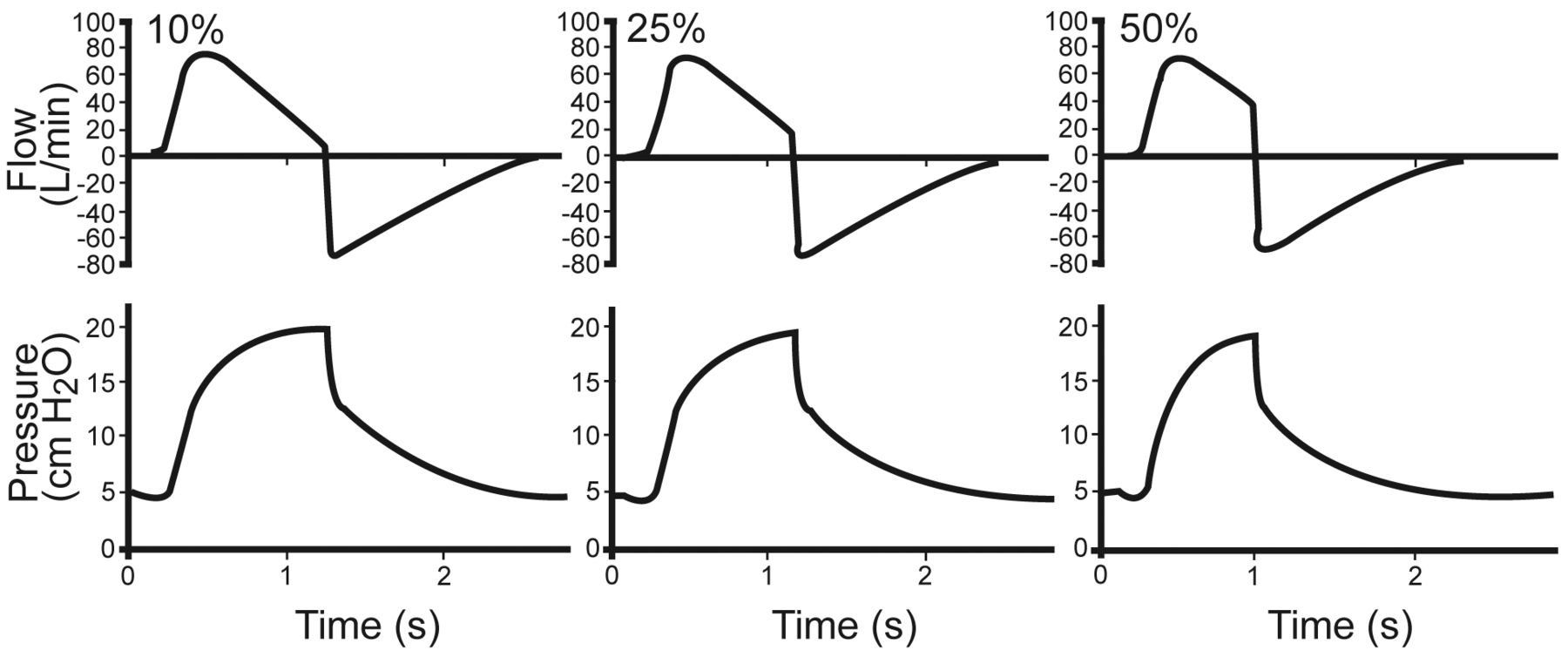
- Fig. 3.
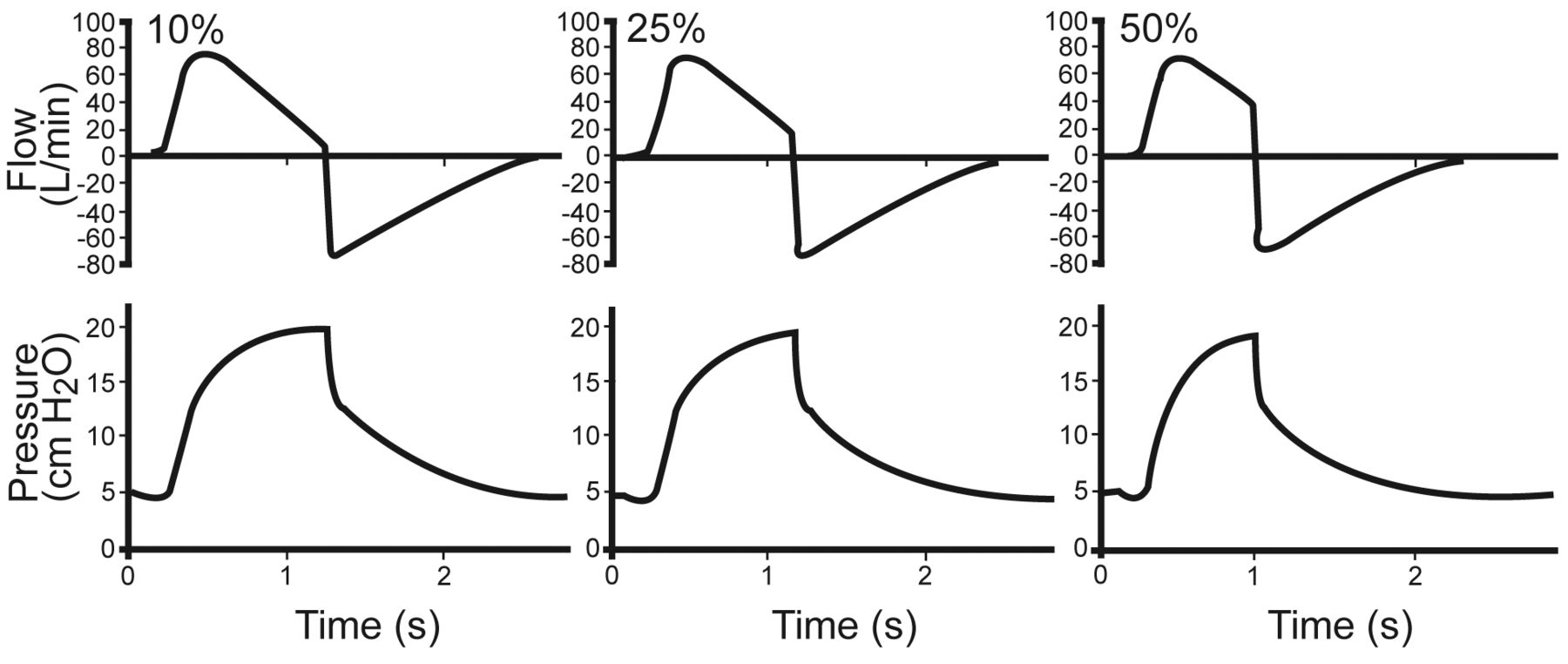
Lung model waveforms with flow cycling at 10%, 25%, and 50%, with a Puritan Bennett 840 ventilator set on pressure support 15 cm H2O and PEEP of 5 cm H2O. The lung model settings were resistance 5 cm H2O/L/s, compliance 0.05 L/cm H2O. (Adapted from Reference 19.)
- Fig. 4.
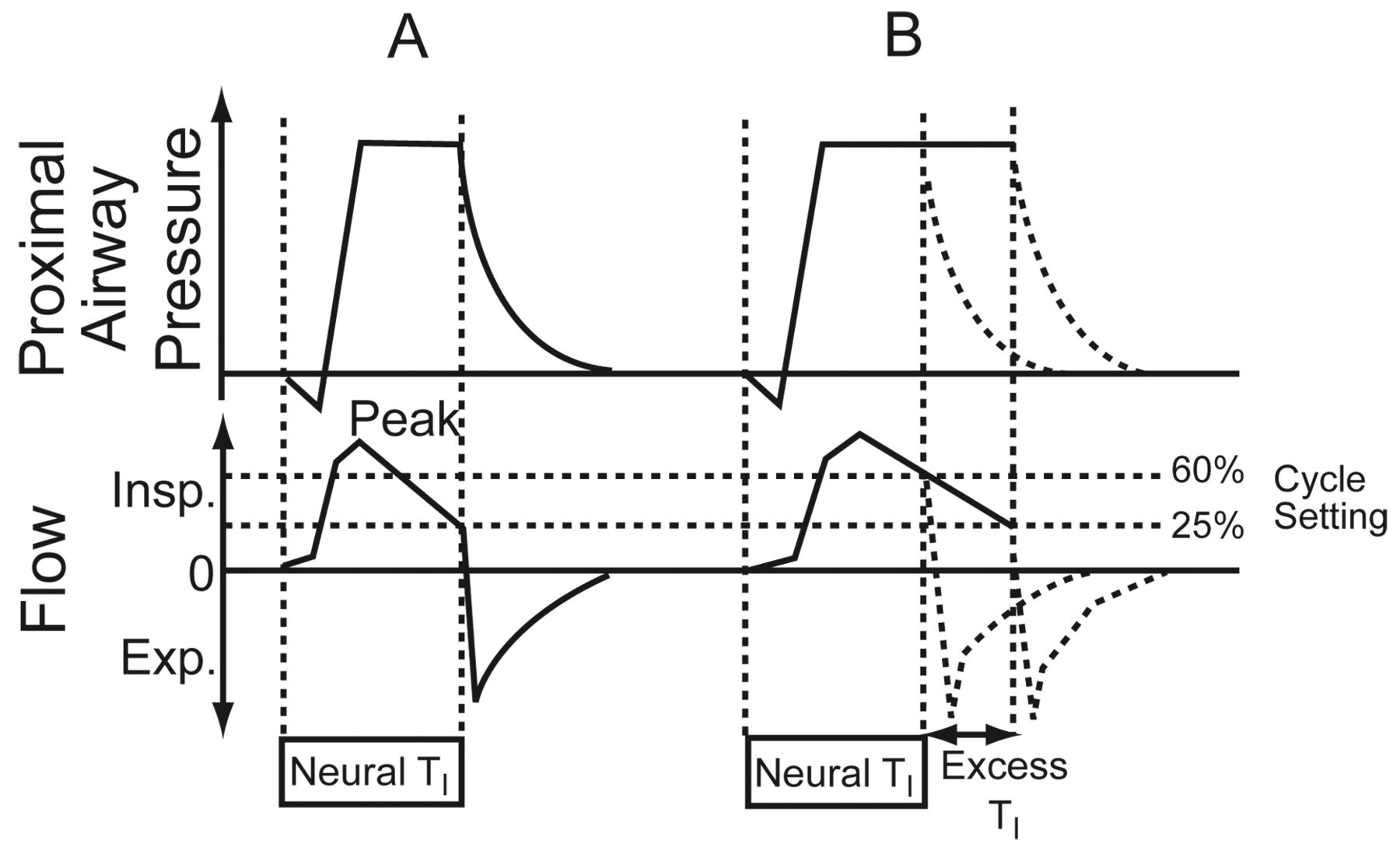
Airway pressure and flow graphics illustrate delayed cycling. A: Normal respiratory mechanics. The cycle setting is 25% of peak inspiratory flow. Cycling is ideal, as indicated by the fact that the inspiratory flow decreases to the 25% cycling level at the end of the patient's neural inspiratory time (TI). B: Obstructive respiratory mechanics. The change in the inspiratory flow curve leads to the 25% level being reached later, well after the end of the neural TI. The duration of delayed cycling is represented by the excess TI. Increasing the cycle setting to 60% of peak inspiratory flow corrects this problem, and cycling occurs at the end of neural TI. Insp = inspiration. Exp = expiration. (Adapted from Reference 22, with permission BioMed Central.)
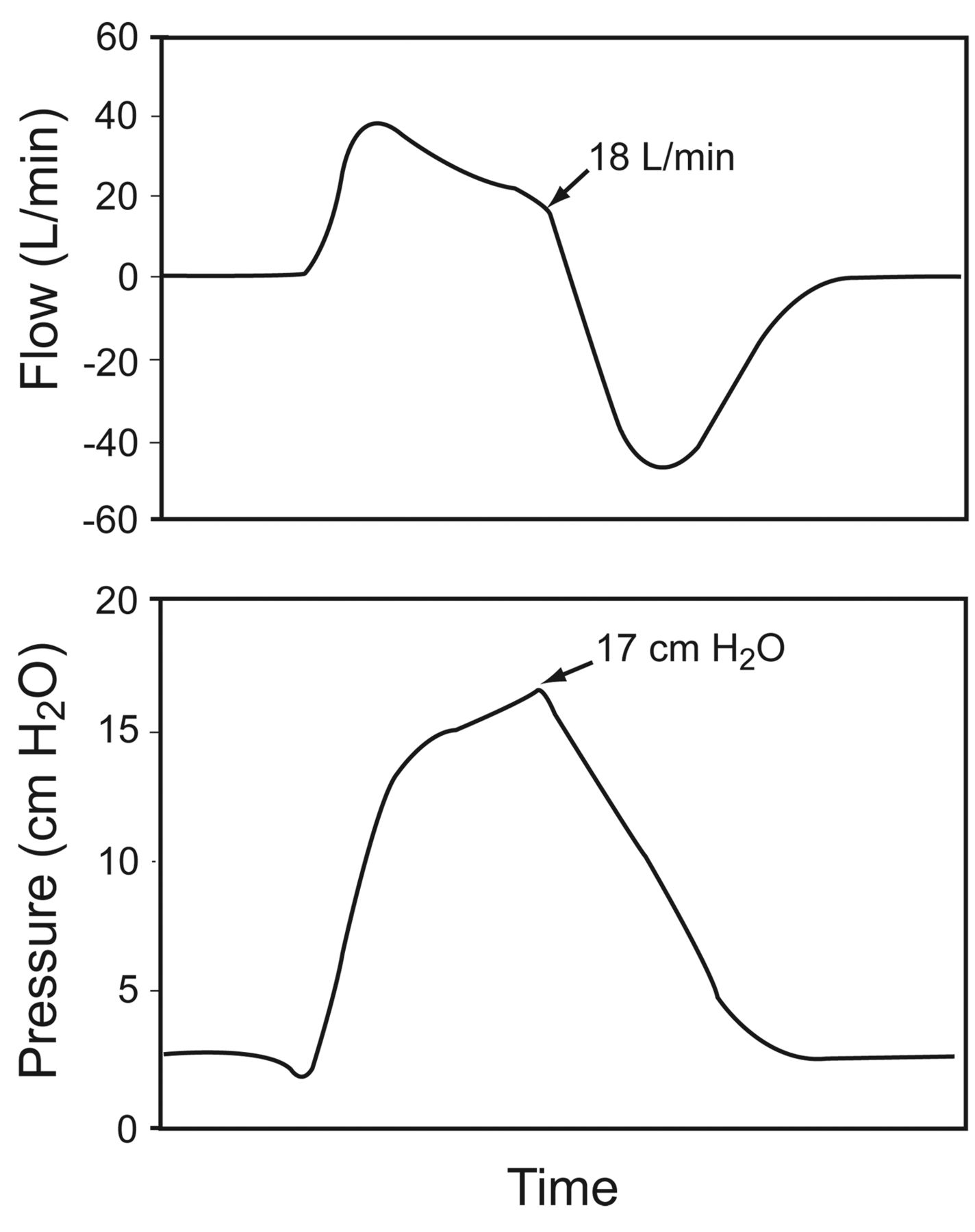
- Fig. 5.
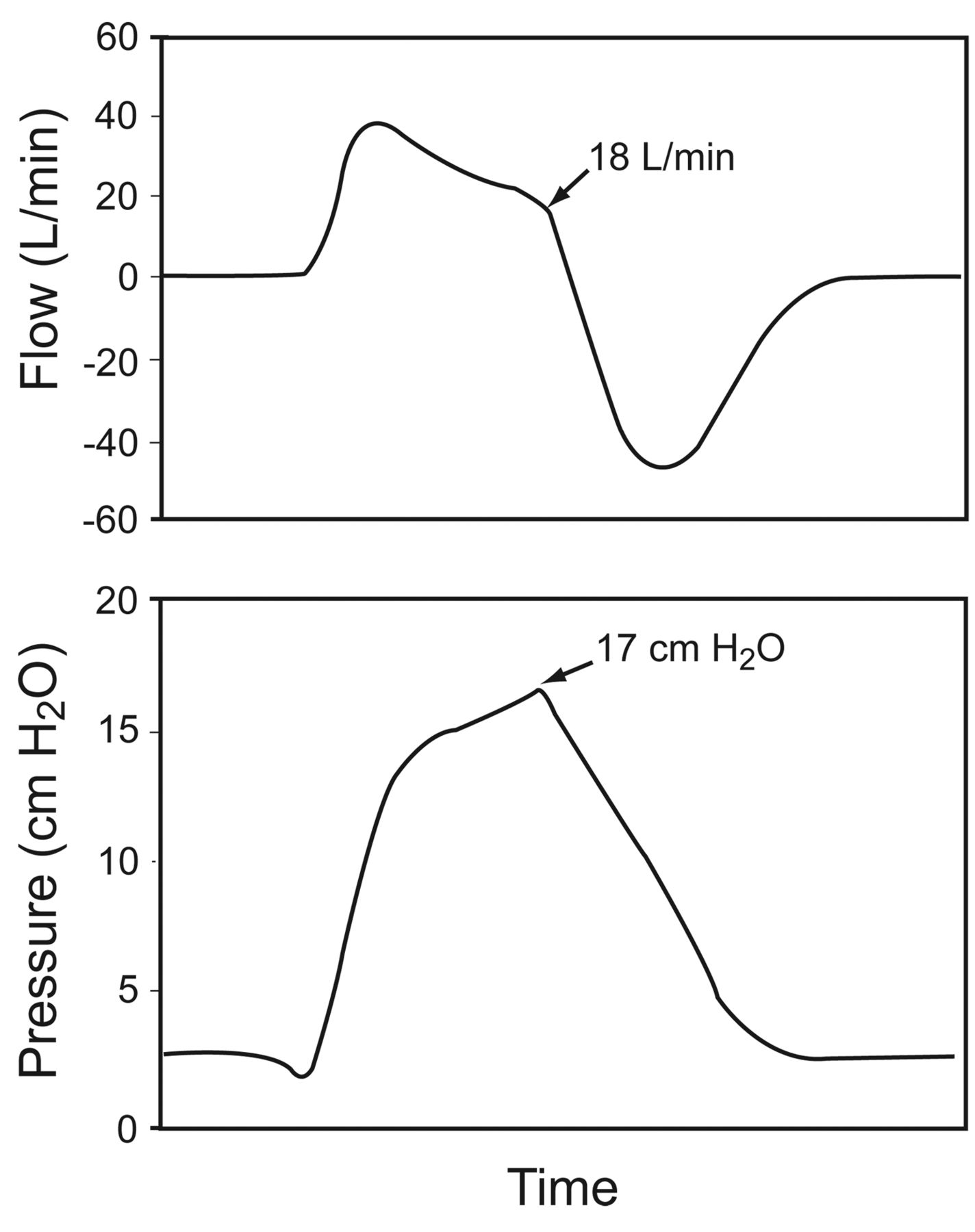
An example of delayed cycling during pressure-support ventilation of a patient with COPD, on a Puritan Bennett 7200 ventilator, which has a flow-termination of 5 L/min during pressure-support ventilation at 12 cm H2O. The ventilator cycles at 18 L/min. The pressure increase above the set pressure-support level causes the ventilator to pressure-cycle in response to the patient's active exhalation. (Adapted from Reference 25.)
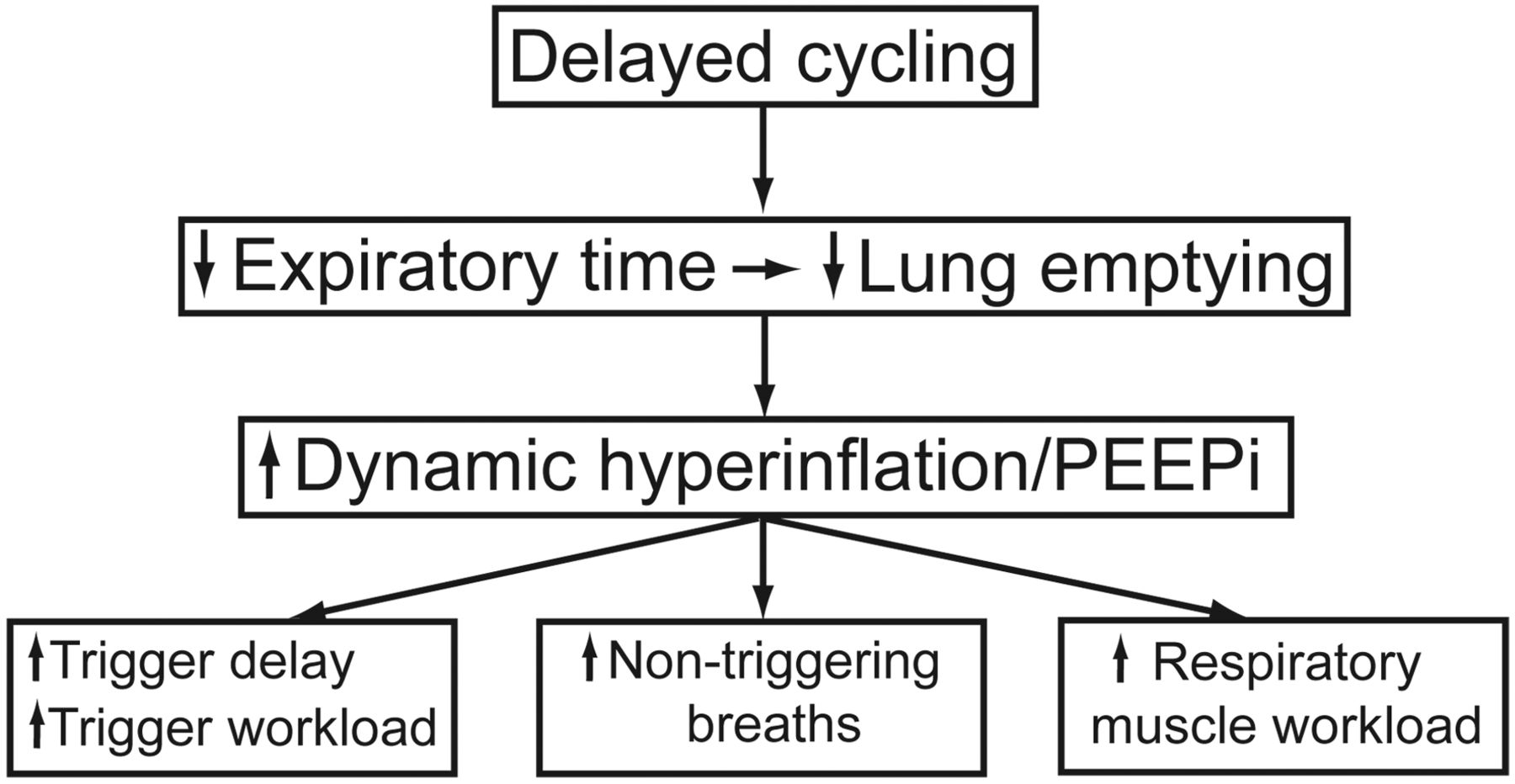
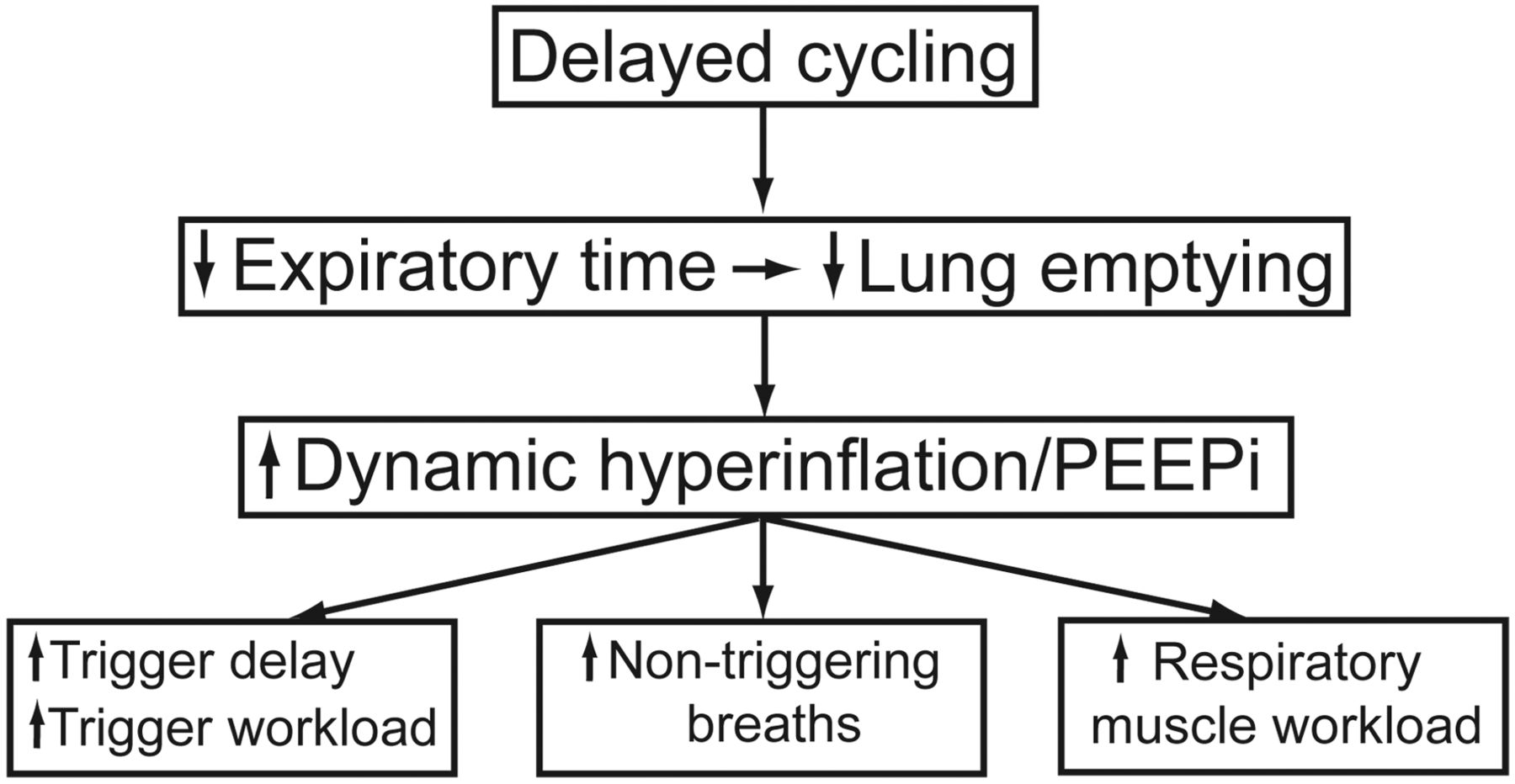
- Fig. 6.
Consequences of delayed cycling. PEEPi = intrinsic PEEP. (Adapted from Reference 22, with permission BioMed Central.)
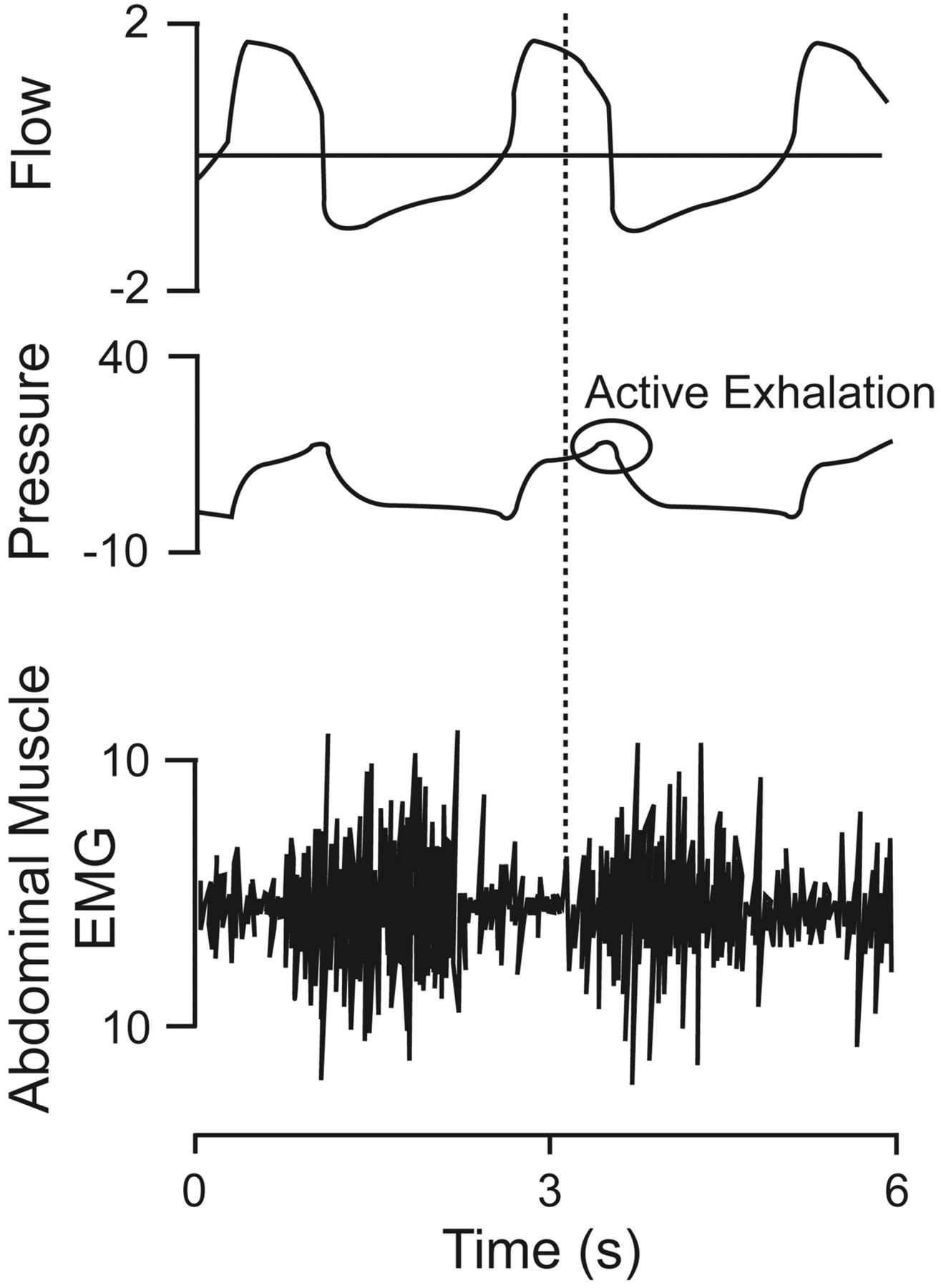
- Fig. 7.
Flow, airway pressure, and transversus abdominis electromyogram (EMG) waveforms from a mechanically ventilated patient with COPD receiving pressure-support ventilation at 20 cm H2O. The onset of expiratory muscle activity (vertical dotted line) occurred when mechanical inflation was only partly completed, as indicated by the onset of expiratory muscle activity. Active exhalation caused an increase in airway pressure at end-exhalation, causing the ventilator to pressure-cycle rather than flow-cycle. (Adapted from Reference 29, with permission.)











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}