

Abstract
BACKGROUND: An increasing number of patients require prolonged mechanical ventilation (PMV), which is associated with high morbidity and poor long-term survival, but there are few data regarding the incidence and outcome of PMV patients from a community perspective.
METHODS: We retrospectively reviewed the electronic medical records of adult Olmsted county, Minnesota, residents admitted to the intensive care units at the 2 Mayo Clinic Rochester hospitals from January 1, 2003, to December 31, 2007, who underwent tracheostomy for PMV.
RESULTS: Sixty-five patients, median age 68 years (interquartile range [IQR] 49–80 y), 39 male, underwent tracheostomy for PMV, resulting in an age-adjusted incidence of 13 (95% CI 10–17) per 100,000 patient-years at risk. The median number of days on mechanical ventilation was 24 days (IQR 18–37 d). Forty-six patients (71%) survived to hospital discharge, and 36 (55%) were alive at 1-year follow-up. After adjusting for age and baseline severity of illness, the presence of COPD was independently associated with 1-year mortality (hazard ratio 3.4, 95% CI 1.4–8.2%).
CONCLUSIONS: There was a considerable incidence of tracheostomy for PMV. The presence of COPD was an independent predictor of 1-year mortality.
Introduction
An increasing number of patients require mechanical ventilation, for various reasons, and there has been a proportional increase in patients also needing prolonged mechanical ventilation (PMV). PMV accounts for about 10% of all mechanically ventilated patients.1,2 Although these patients represent a smaller proportion of intensive care unit (ICU) patients, they consume substantial ICU resources.3 Studies from referral centers have found poor long-term survival among PMV patients, with 1-year mortality of 56–71%.1,4–7 Of those who are transferred to long-term care hospitals 52% die within the first year of follow-up.8 Considering the high morbidity, mortality, and cost of PMV,9,10 there is an increasing interest in identifying PMV patients who are at higher risk of death. Data from a community-based perspective could help limit the referral bias inherent in the epidemiologic studies from critical-care sources.11
The purpose of this study was to determine the incidence and the contemporary prognosis associated with PMV in Olmsted county, Minnesota. We took advantage of the fact that virtually all healthcare in Olmsted county is provided by just 2 providers, and only the Mayo Clinic offers critical-care services. With data from Olmsted county we can conduct detailed studies of etiology and outcome of critical illness in a defined geographic population with unrestricted access to mechanical ventilation, including PMV.
Methods
The Mayo Clinic institutional review board approved the study protocol and waived the informed-consent requirement. As required by Minnesota law, we excluded patients who had previously denied authorization for the use of their medical records for research. This was a retrospective cohort study, performed at Mayo Clinic, Rochester, Minnesota. We reviewed electronic medical records from residents of Olmsted county, ≥ 18 years of age, admitted to ICUs at the 2 Mayo Clinic Rochester hospitals from January 1, 2003, to December 31, 2007 who underwent tracheostomy for anticipated or established PMV and/or who had failed multiple ventilator-weaning attempts.12
According to the 2000 United States census, the population of Olmsted county was 124,277, 50.9% female, 90.3% white, and 10.7% age ≥ 65 years. The patients were admitted to one of the 8 adult Mayo Clinic ICUs, which include medical, surgical, and cardiac care units, with a total of 154 beds. Olmsted county age-group-specific ICU admission and utilization rates were previously reported.13 Olmsted county residents were identified via their home zip codes at ICU admission.
Patients who underwent tracheostomy were identified according to the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9 CM, code 31.1 temporary tracheostomy). We reviewed the electronic medical records to confirm the indication for temporary tracheostomy (respiratory failure with anticipated or PMV) and to collect data on demographics, comorbidities, and clinical and laboratory variables that could be related to long-term prognosis. The incidence of tracheostomy for PMV was age-adjusted according to the 2000 United States standard population.14 Mortality was assessed by reviewing the medical records and the Olmsted county electronic death certificates.
We measured severity of illness with the Acute Physiology and Chronic Health Evaluation (APACHE) III at ICU admission.15 We used standard clinical definitions to define comorbidities: COPD,16 diabetes mellitus,17 trauma,18 neuromuscular disease (acute or chronic),19 major surgery,20 and cumulative Charlson score.21
We also used standard definitions to determine the presence or absence of ICU complications, including acute lung injury22 and shock.23 If a patient had multiple tracheostomies, only the data from the first admission were used for statistical analysis.
Statistical Analysis
Continuous data are expressed as median and interquartile range (IQR). Categorical variables are expressed as counts and percentages. We compared the characteristics of patients who survived more than 1 year versus less than 1 year with the Wilcoxon rank-sum test, chi-square test, or Fisher's exact test, as appropriate. We calculated the total number of days on mechanical ventilation from the initiation of mechanical ventilation until the patient was weaned, but excluded patients who were continued on mechanical ventilation following hospital discharge. We used survival analysis methods to assess time-to-event data, and calculated 1-year survival from the initiation of mechanical ventilation. We used Cox proportional regression to identify predictors of survival. Pertinent variables were selected based on both clinical and statistical variables or according to previous epidemiologic studies, clinical judgment, and missing data. Variables that were associated with adverse 1-year outcome in univariate analysis (P < .1) were considered for multivariate Cox proportional regression model analysis. Statistical significance was set at P = .05 for all hypotheses. Statistical analyses were performed with statistics software (JMP 7, SAS Institute, Cary, North Carolina).
Results
Six-hundred ninety-two Olmsted county residents received invasive mechanical ventilation (≥ 12 h) during the study period. One-hundred eighteen patients had the ICD 9 code for temporary tracheostomy. The 52 patients who received tracheostomy for head and neck carcinoma or airway protection were excluded.
Sixty-five patients, 39 male, median age 68 years (IQR 49–80 y), underwent tracheostomy for PMV, resulting in an age-adjusted incidence of approximately 13 (95% CI 10–17) per 100,000 person-years at risk for the population of Olmsted county. One patient had tracheostomy performed twice for the purpose of PMV during the study period. Fifty-one (77%) of the tracheostomies were surgical. The median number of days on mechanical ventilation was 24 days (IQR 18–37 d) and the median time from initiation of mechanical ventilation to tracheostomy was 10 days (IQR 7–14 d). Forty-six patients (71%) survived to hospital discharge, and 36 (55%) were alive at 1-year follow-up. Survival was similar in patients who were ventilated for more than versus less than 21 days (16/26 vs 20/39, P = .19 via log-rank test). Only 3 survivors did not have a subsequent follow-up visit after 1 year, and their vital status was ascertained from the Olmsted county electronic death certificates. Table 1 describes the survivors and non-survivors.
Survivors Versus Non-survivors at One Year
Five patients, including 4 with neuromuscular diseases, were continued on mechanical ventilation after hospital discharge, and 4 of them survived 1 year. None of those patients was liberated from mechanical ventilation during 1-year follow-up. Nineteen patients (29%) died in hospital (median hospital stay 34 d, IQR 24–77 d), 16 (84%) of them met the diagnostic criteria for acute lung injury. Of the 10 patients who died after hospital discharge, 4 had a cerebrovascular event and 3 developed new respiratory failure (Table 2). Median survival after hospital discharge in those 10 patients was 48 days (IQR 28–73 d).
Causes of Death After Hospital Discharge
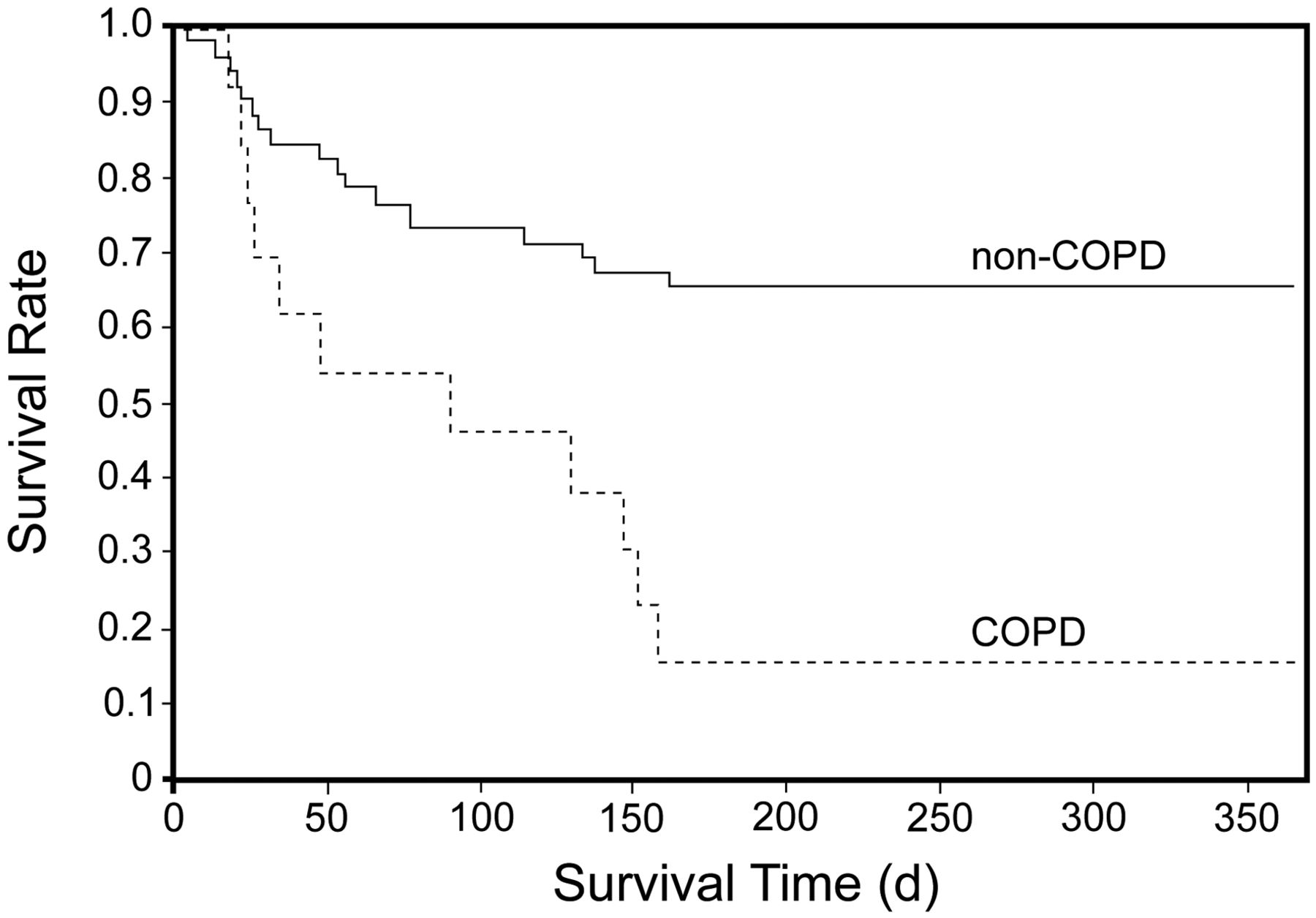
After adjusting for APACHE III hospital predicted mortality in a Cox proportional hazard analysis, both age (hazard ratio [HR] 1.7, 95% CI 1.3–2.4) and the presence of COPD were independently associated with lower 1-year survival (hazard ratio 3.4, 95% CI 1.4–8.2) (Table 3 and Fig. 1). Of the 13 patients with COPD, pulmonary function test results were available from 11 (mean percent-of-predicted FEV1 48%, range 17–64%). Two patients had very severe, 5 had severe, and 4 had moderate COPD, according to the Global Initiative for Chronic Obstructive Lung Disease16 criteria. The presence of comorbidities (chronic heart failure, diabetes, or hemodialysis) did not influence the long-term outcome.
Factors Associated With One-Year Survival

Kaplan-Meier curve of 1-year survival in patients with versus without COPD, who required prolonged mechanical ventilation (P = .006 via log-rank test).
Discussion
There was a considerable incidence of tracheostomy for PMV in Olmsted county, Minnesota. In addition to age, underlying COPD was associated with worse long-term survival. The 1-year mortality rate was lower than most previous reports5,24–26 but similar to recent studies27,28 that included outside referral populations. Potential explanations include contemporary improvements in clinical practice, the availability of medical care for the population of Olmsted county, and the exclusion of referral bias. One of the limitations in comparing the long-term outcomes reported in different studies is a lack of a uniform definition of PMV, which has ranged from ≥ 4 days to > 21 days. Some studies2,3 used tracheostomy placement to identify PMV patients, but those patients might not reach the chronic phase of critical illness (defined as the presence of mechanical ventilation on day 21).29 We believe that this is unlikely to have a confounding effect on our data, since outcomes were similar in our patients who were ventilated < 21 days versus > 21 days.
The majority of non-survivors died before hospital discharge. Among hospital survivors, those with unfavorable outcome died within the first 3 months after hospital discharge. The 6-month survival did not differ from 1-year survival (see Fig. 1). Patients with neuromuscular diseases, although they more likely to continue mechanical ventilation after hospital discharge (4 of 7 patients), had a relatively low mortality, consistent with a previous study.30 In contrast, a large prospective study of patients discharged from a respiratory unit after PMV found a high mortality rate in patients who were not weaned from the ventilator, and neurological comorbidity was an independent predictor of weaning success.31
Similar to other studies,4,5,24,28,32 age was a significant predictor of 1-year survival, but, in contrast to those reports, COPD was also an independent predictor of 1-year mortality. This is not surprising, since both the in-hospital and 1-year mortality in patients with COPD who require mechanical ventilation is substantial.33 COPD is an independent predictor for duration of mechanical ventilation, and 60% of COPD patients in a recent study experienced weaning failure.34 COPD was the most frequent premorbid respiratory diagnosis in ventilator-dependent patients referred to long-term care hospitals.35 COPD was also found to be an independent risk factor for long-term mortality in patients admitted to a specialized weaning center, but the analysis was restricted to hospital survivors.36 Other data on patients treated at home with tracheostomy and intermittent positive-pressure ventilation also reported COPD to be independently associated with mortality.37 Pilcher et al observed a higher post-discharge long-term mortality rate in COPD patients, compared to neuromuscular and surgical patients, but the difference was nonsignificant in multivariate analysis.30 The differences regarding predictive value of COPD on long-term survival of PMV patients could be due to the fact that patients with COPD are not always offered, or choose not to undergo, invasive mechanical ventilation because of poor prognosis.38 In addition, unlike studies that found no association between COPD and mortality in PMV patients,3,28,32 COPD diagnosis in our study was confirmed by a pulmonary function test in the majority of cases.
There has been an increasing recognition of PMV patients as a subgroup of ICU patients with high-level care needs, and an effort has been made to try to identify predictors of outcome. The scrutiny has focused on factors associated with baseline severity of illness and factors present on hospital discharge. A recently reported prognostic model based on variables associated with a severity of illness at day 21 of mechanical ventilation (use of vasopressors, hemodialysis, platelet count ≤ 150 × 109/L, and age ≥ 50 y) proved to be an efficient tool for predicting 1-year outcome. This could be due to the fact that their proposed variables28 reflect the severity of acute critical illness, as most of the non-survivors die in the first few months of follow-up, and death of those patients could be related to unresolved medical issues in the course of their critical illness. Severity of illness on admission and pre-morbid functional status are associated with worse short-term mortality, whereas age and comorbidities assessed with the Charlson comorbidity score reflect negatively against long-term survival.7,32 The fact that a new respiratory failure was responsible for the death of only 30% of the patients who died after hospital discharge probably reflects additional comorbidities. Several studies have found more favorable outcome in trauma patients and patients with neuromuscular diseases.7,30,36,39
One of the major limitations of this study is associated with difficulties inherent to the small number of patients and its retrospective nature. The study was conducted in a single tertiary-care center, and the results may not generalize to other settings. The variables at hospital discharge, such as presence of neuromuscular weakness or neurocognitive dysfunction following ICU discharge, could not be evaluated. The small number of patients requires caution when interpreting the results. Another limitation is that we used tracheostomy to detect patients who required PMV, which excluded patients who did not undergo tracheostomy because of high severity of illness and poor prognosis.
Conclusions
A considerable number of critically ill Olmsted county residents underwent tracheostomy for PMV. In addition to previously established predictors of long-term survival (age and severity of illness), the chronic conditions that related to underlying cause of mechanical ventilation (ie, COPD, neuromuscular disease, trauma) should be taken into account when assessing possible outcomes.
Footnotes
- Correspondence: Ognjen Gajic MD MSc, Division of Pulmonary and Critical Care Medicine, Mayo Clinic, 200 First Street SW, Rochester MN 55905. E-mail: gajic.ognjen{at}mayo.edu.
-
This research was partly supported by National Institutes of Health grant HL78743–01A1.
-
Dr Kojicic presented a version of this paper at the 105th International Conference of the American Thoracic Society, held May 15–20, 2009, in San Diego, California.
See the Related Editorial on Page 1859
- Copyright © 2011 by Daedalus Enterprises Inc.









{kind=link}