

Abstract
OBJECTIVES: The primary objective of this retrospective study was to evaluate whether abnormal predicted postoperative variables and predicted postoperative product are useful in predicting postoperative complications. The secondary objective was to assess whether an abnormal diffusion heterogeneity index is associated with increased postoperative complications.
METHODS: In this retrospective study we evaluated the medical records of 57 patients who underwent lung resection for lung cancer. Calculations of the predicted postoperative variables were done using preoperative testing data, including the extent of the resected lung segments. Predicted postoperative product was obtained by multiplying the predicted postoperative percent-of-predicted FEV1 by the predicted postoperative percent-of-predicted single-breath diffusing capacity of the lung for carbon monoxide (DLCO). The measured product was obtained by multiplying FEV1 by DLCO. We derived diffusion heterogeneity index from measurements of the single-breath DLCO with the 3-equation method, as a measure of the heterogeneity of the distribution of gas exchange in the lung.
RESULTS: Patients with complications had lower predicted postoperative FEV1 (P < .001), lower predicted postoperative DLCO (P < .001), lower predicted postoperative maximal oxygen uptake (P < .001), lower predicted postoperative increase in percent-of-predicted DLCO at 70% work load from at-rest percent-of-predicted DLCO (ΔDLCO%) (P < .001), lower predicted postoperative product (P < .001), and lower measured product (P = .004). Interestingly, diffusion heterogeneity index increased with exercise in all patients with complications but decreased with exercise in all patients without complications.
CONCLUSIONS: The predicted postoperative variables, predicted postoperative product, measured product, and diffusion heterogeneity index are potentially useful predictors of complications in candidates for lung resection.
- diffusing capacity
- exercise testing
- lung resection
- predicted postoperative product
- preoperative evaluation
- spirometry
Introduction
Lung-function testing, including FEV1 and single-breath diffusing capacity of the lung for carbon monoxide (DLCO), has been used in assessing patients with non-small-cell lung cancer.1,2 Some studies have suggested that DLCO should be assessed routinely in candidates for major pulmonary surgery, regardless of spirometry findings.3,4 More recently, the predicted postoperative FEV1 and predicted postoperative DLCO, estimated via preoperative lung-perfusion scanning and assessment of the contribution of the resected lung to overall function,5 were shown to have predictive value for postoperative complications following lung resection. The product of predicted postoperative percent-of-predicted FEV1 and predicted postoperative percent-of-predicted DLCO (the so-called predicted postoperative product), may be a useful value that combines the important elements of both measurements.6
The effects of diffusion heterogeneity on DLCO measurements was recently described.7 Graham et al developed an index to quantify diffusion heterogeneity (the diffusion heterogeneity index).8 The overall 3-equation DLCO uses all of the information measured during inhalation, breath-holding, and exhalation to calculate the average diffusing capacity of the entire lung. The alveolar gas sample consists of all of the gas exhaled following dead-space washout. This large sample of alveolar gas is then divided into 4 equal-volume samples and the data are re-analyzed 4 times, with a separate 3-equation DLCO calculated for each of the 4 smaller samples. The diffusion heterogeneity index is a measure of how much the DLCO measured in the 4 small samples differs from the DLCO measured in the large sample. In a perfectly homogeneous lung, the diffusion heterogeneity index would be zero. In a normal, healthy subject the diffusion heterogeneity index is typically near zero.8 Smokers with normal DLCO and normal FEV1 have an elevated diffusion heterogeneity index.
The primary objective of this retrospective study was to evaluate whether abnormal predicted postoperative variables and predicted postoperative product are useful in predicting morbidity and mortality following lung resection. The secondary objective was to determine whether abnormal diffusion heterogeneity index is associated with increased postoperative complications following lung resection.
Methods
This study was approved by the University of British Columbia Clinical Screening Committee for Research and Other Studies Involving Human Patients. All patients gave informed consent before participating. The experimental protocol was the same as in our previous study.9
Subjects
Retrospectively, we evaluated all patients with a diagnosis of non-small-cell lung cancer who underwent thoracotomy for lung resection at Vancouver General Hospital, during an 8-month period. The preoperative data were recorded, and the postoperative course of the patients was followed carefully with detailed assessment. We evaluated DLCO during exercise before lung resection with the 3-equation DLCO method. Since the 3-equation method can determine DLCO accurately without the need for breath-holding in the single-breath maneuver, this method is useful in evaluating DLCO during moderate to high intensity exercise, in which prolonged breath-holding is difficult.9 We related changes in DLCO during exercise to postoperative complications.
Predicted Postoperative Value
The calculation of the predicted postoperative value variable was described in previous studies10,11:
where S is the number of resected segments (10 in the right lung, and 9 in the left lung), and N is the number of nonfunctional or obstructed segments in the resected lung, determined from the preoperative chest radiograph, chest computed tomogram, and bronchoscopy. For more than 75% obstruction of a segment, N is taken as 1; for obstruction of 50–75%, N is taken as 0.5; and milder obstruction is ignored.12 The predicted postoperative product is the product of predicted postoperative percent-of-predicted FEV1 and predicted postoperative percent-of-predicted DLCO. We defined the measured product as the product of measured preoperative percent-of-predicted FEV1 and measured preoperative percent-of-predicted DLCO.10
Diffusion Heterogeneity Index
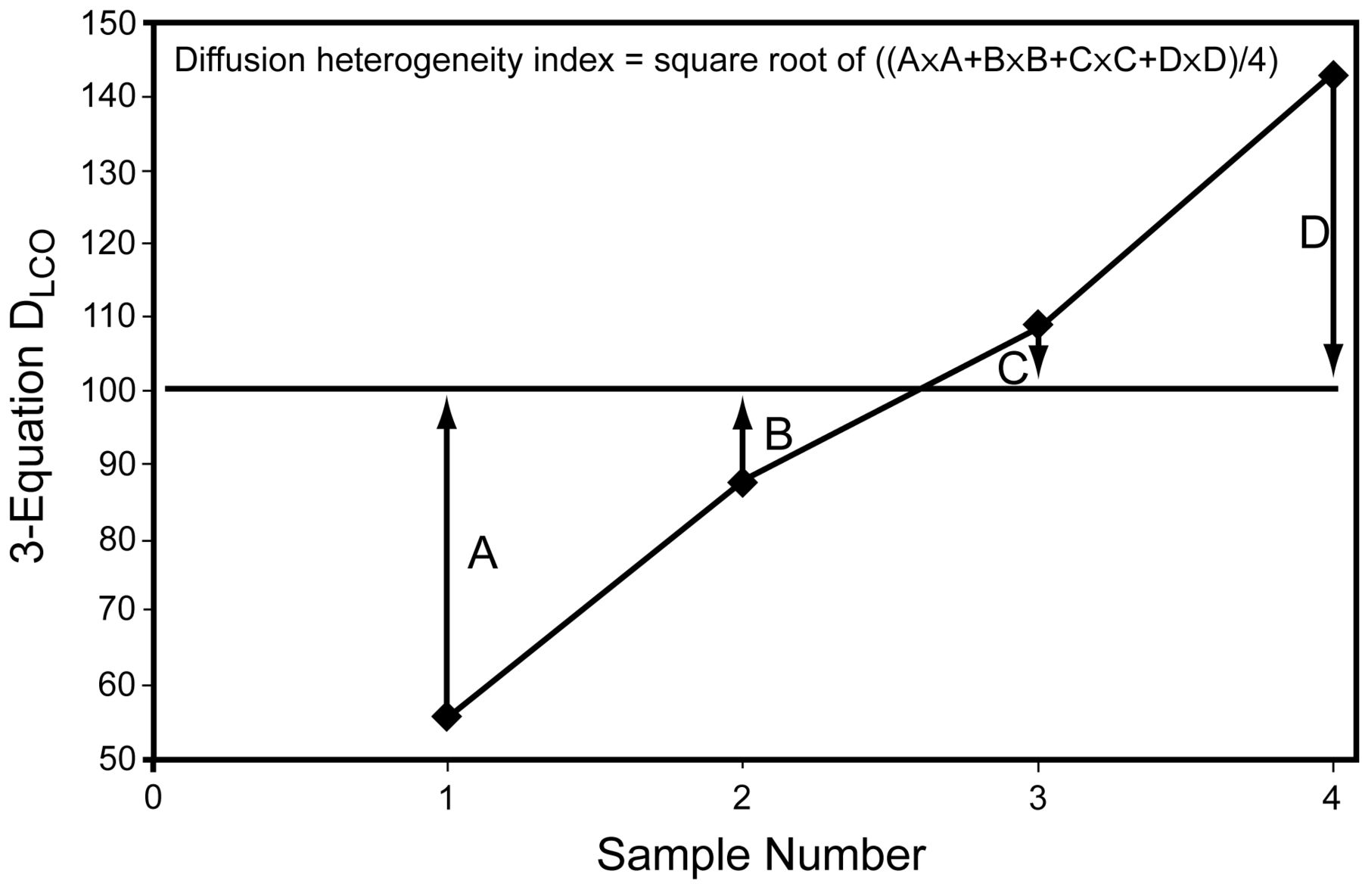
The diffusion heterogeneity index reflects the degree to which DLCO values calculated from 4 equal-volume alveolar gas samples deviate from the DLCO from the entire alveolar gas sample, by measuring the root-mean-square difference8 of the normalized DLCO values (Fig. 1). Since lung regions that are better ventilated empty earlier in exhalation, DLCO from 4 separate samples show DLCO differences. The 3-equation method is needed because it can analytically compensate for the size and timing of the alveolar sample and does not introduce errors in DLCO when sample collection is delayed.8 For a perfectly homogeneous lung, the diffusion heterogeneity index is zero. The diffusion heterogeneity index increases as the heterogeneity of diffusion in the lung increases.

Normalized 3-equation values for the diffusing capacity of the lung for carbon monoxide (DLCO), calculated from 4 equal alveolar gas samples by expressing them as a percentage of DLCO calculated from the total alveolar gas sample. Points A, B, C, and D denote the difference between the 4 normalized values calculated from the 4 equal alveolar gas samples, respectively, and the normalized DLCO from the total alveolar gas sample (indicated by the horizontal line). The root mean square difference of the 4 samples is the diffusion heterogeneity index.
Postoperative Complications
Two thoracic surgeons did all the thoracotomies and pulmonary resections. The patients' postoperative courses were followed carefully, with detailed assessment and recording of complications. We classified postoperative in-hospital complications into mortality, cardiovascular, and pulmonary morbidity.10
Statistical Analyses
We analyzed the data with statistics software (Excel 2007, Microsoft, Redmond, Washington, and SPSS 17.0, SPSS, Chicago, Illinois). We determined the means and standard deviations for the whole group and for patients with and without complications. We compared continuous variables with the 2-tailed Student t test, and categorical variables with the chi-square test. We analyzed multiple variables with stepwise logistic regression,13 to investigate the relative usefulness of the combination of different variables for predicting postoperative complications. Differences between groups were considered significant if P < .05. We calculated the receiver operating characteristic curves of these variables for overall complications, and the area under the receiver operating characteristic curve.14 We used the receiver operating characteristic curve to define the best cut points for the variables in relation to postoperative complications. Further validation of our cut points should be performed prior to clinical use.15,16 Sensitivity and specificity for each variable were determined.14 We compared the area under the receiver operating characteristic curves with the method of Hanley and McNeil.17
Results
The 57 patients had a mean age of 64 ± 10 y; 39 (68%) were men, and 18 (32%) were women. Mean height was 170 ± 10 cm, and mean weight was 74 ± 15 kg. Twenty-four patients (42%) were smokers, and their mean smoking history was 55 ± 30 pack-years. Twenty-two (39%) were ex-smokers, and their mean smoking history was 34 ± 24 pack-years. Eleven patients (19%) had never smoked. Twenty-four patients (41%) had a diagnosis of COPD. The surgeries were 10 pneumonectomies, 2 bi-lobectomies, 32 lobectomies, 6 segmentectomies, 4 wedge resections, and 3 thoracotomies without lung resection.
Table 1 shows the preoperative lung-function data. The predicted postoperative percent-of-predicted FEV1 was 66 ± 22%. Thirty-three patients had mild or moderate ventilatory obstruction. The predicted postoperative percent-of-predicted DLCO was 60 ± 19%. Thirty patients had mild or moderate DLCO impairment. Maximal exercise capacity was reduced in 36 patients. The predicted postoperative maximum oxygen uptake was 15 ± 4 mL/kg/min. To adjust for differences in sex, age, and height in different patients, we express DLCO values (at rest and exercise) as percent-of-predicted at-rest DLCO. We measured the change in DLCO at 70% work load above at-rest DLCO (ΔDLCO). The predicted postoperative ΔDLCO was 20 ± 16%, and there was significant inter-patient variability in ΔDLCO.
Preoperative Lung-Function Data
Postoperative complications occurred in 19 patients (33%), and included mortality in 2 (4%) (both from pulmonary edema), cardiovascular morbidity in 12 (21%), and pulmonary morbidity in 13 (23%). Arrhythmia (atrial fibrillation in 10 patients, and ventricular premature contraction in 1 patient) was the major cardiovascular morbidity, occurring in 19% of all the patients. Two patients had pulmonary edema and one had shock. Pneumonia was the major pulmonary morbidity, occurring in 7 patients (12% of all the patients). Five patients had atelectasis, 4 developed respiratory insufficiency, and 2 required ventilatory support and re-intubation.
The patients with complications were older than those without complications (70 y vs 61 y, P = .005); were more frequently diagnosed with COPD (14/19 vs 10/38, P = .003); had more pack-years of smoking (60 vs 50, P = .01). Table 2 lists preoperative lung-function variables in relation to complications. Interestingly, patients with complications had higher diffusion heterogeneity index (P = .02), higher diffusion heterogeneity index during exercise (P < .001), and higher change in diffusion heterogeneity index (P = .006) (see Table 2). Moreover, the diffusion heterogeneity index during exercise was larger than the at-rest diffusion heterogeneity index in the patients with complications, but the diffusion heterogeneity index during exercise was smaller than the at-rest diffusion heterogeneity index in the patients without complications. The diffusion heterogeneity index increased with exercise in the patients with complications, but it decreased with exercise in the patients without complications.
Preoperative Lung-Function Variables in Relation to Complications
Table 3 shows the β coefficient and intercept values for the preoperative variables; it appears that all 9 predictors, as indicated by significant P values, are potentially useful for overall complications prediction. Multiple-variable analyses via backward stepwise logistic regressions showed that predicted postoperative ΔDLCO% remained at the end of the run after the models combining all 9 different variables.
β Coefficient and Intercept Values From the Regression Equations for the Preoperative Variables' Prediction of Postoperative Complications*
The largest area under the receiver operating characteristic curve was calculated from predicted postoperative ΔDLCO% for overall complications (Fig. 2), and the difference was statistically significant from that of the other variables. Table 4 compares the postoperative complications with cut points for the preoperative variables.
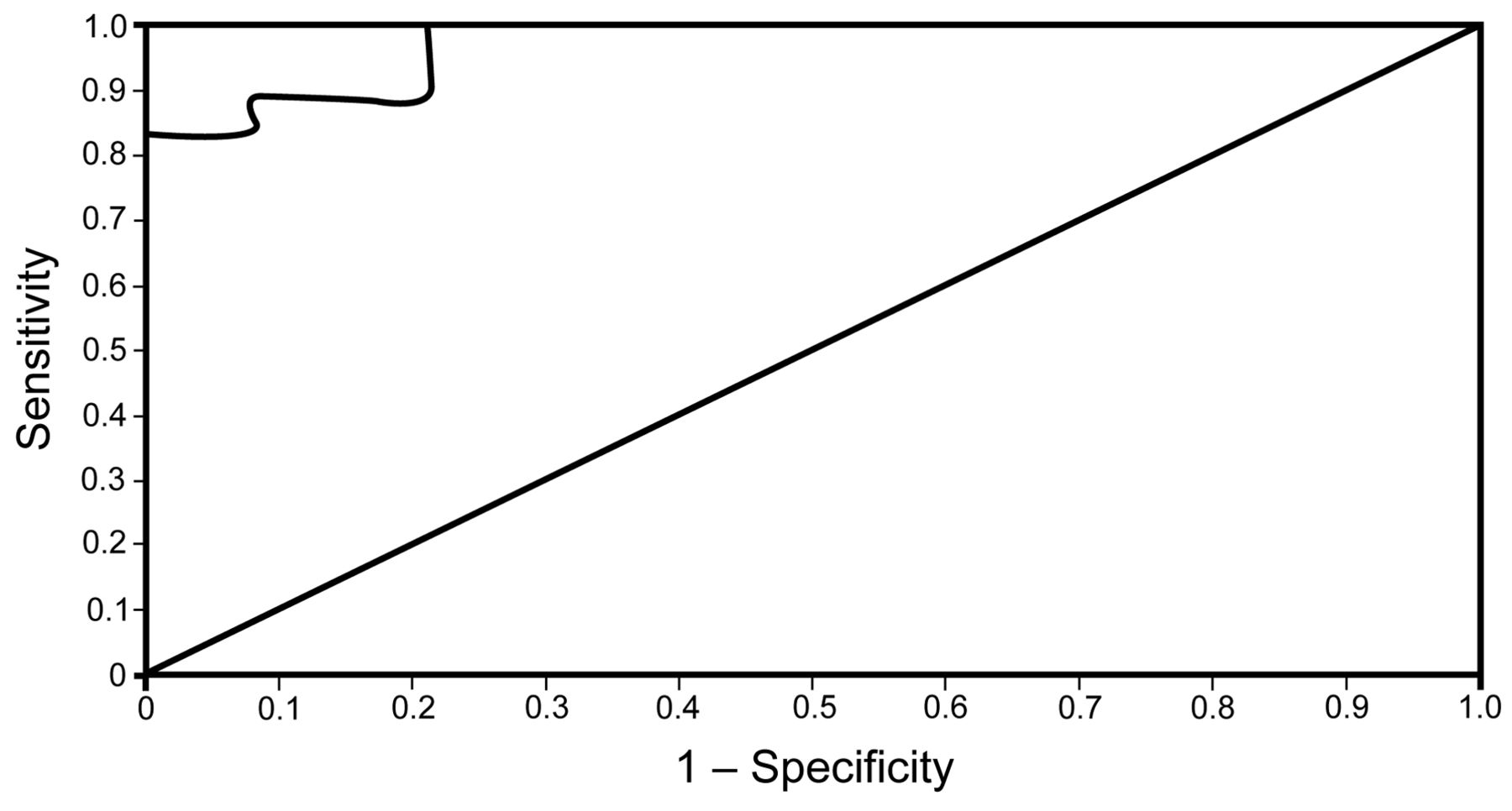
Receiver operating characteristic curve of preoperative variables for prediction of overall complications. The straight line is the line of identity for a test without any discrimination. The area under the receiver operating characteristic curve of predicted postoperative (70% work load) DLCO% was 0.97. The best cut point was 14%, at which sensitivity was 89% and specificity was 92%.
Comparison of Postoperative Complications Using Cut Points of Preoperative Variables
When the change in diffusion heterogeneity index was analyzed as a categorical variable, such that an increase in diffusion heterogeneity index with exercise was classified as a negative result and a decrease in diffusion heterogeneity index with exercise was classified as a positive result, then the sensitivity and specificity were both 100%, since all patients with postoperative complications had a positive preoperative tests, and all patients without complications had a negative preoperative test.
Discussion
We have evaluated the role of some new indices (predicted postoperative values, predicted postoperative product, measured product, and diffusion heterogeneity index) in the preoperative evaluation of candidates for lung resection. The main finding of our previous study was that patients with complications had only a limited increase in DLCO during exercise, expressed as percent-of-predicted at-rest DLCO, compared to patients without complications. The present results show that all these new indices are potentially useful in predicting complications (see Tables 2, 3, and 4) and that the best cut point for predicting complications was 14% in predicted postoperative ΔDLCO% (see Table 4 and Fig. 2).
In this study the postoperative complication rate was 33% and the mortality rate was 4%. Those findings are similar to recent reports,18 and the mortality rate of 5% in our review of 151 pneumonectomy patients,1 and are considered acceptable. Cardiac arrhythmia was the major cause of morbidity. But pulmonary edema was the major cause of mortality in this study, suggesting having a similar finding in our retrospective review.1 Pulmonary edema and cardiac dysrhythmias may be induced by the supraphysiological stresses imposed on the heart and lung during surgery and postoperatively, due to hyperperfusion of the remaining pulmonary vascular bed.
Studies with quantitative radionuclide lung scanning19,20 are useful in preoperative evaluation. Pierce et al6 found that a new index, designated the predicted postoperative product, obtained by multiplying the percent-of-predicted postoperative FEV1 by the percent-of-predicted postoperative DLCO, has the strongest ability for predicting mortality. The predicted postoperative product is a new concept that includes values of ventilatory function (FEV1), gas transfer (DLCO), lung perfusion (lung scan), and the resected lung into a single index. Because the predicted postoperative product uses percent-of-predicted rather than absolute FEV1 and DLCO values, it can apply to patients of either sex across a wide range of age and height. The predicted postoperative product allows a patient with a value below the threshold for one criterion based on predicted postoperative FEV1 or predicted postoperative DLCO to be accepted for surgery on the basis of a good value in the other. Only a few of our patients had quantitative radionuclide lung scans, but we calculated the predicted postoperative values for FEV1 and DLCO from the surgical excision of functional lung segments, using the modified formula of Nakahara et al.11 Predicted postoperative FEV1 determined in that manner was used in a recent study.21 We also used this formula to calculate predicted postoperative DLCO, predicted postoperative oxygen uptake, and predicted postoperative ΔDLCO. The predicted postoperative values for FEV1 and DLCO enabled us to calculate the predicted postoperative product from the preoperative data in all patients. In this study the calculated predicted postoperative product was useful in predicting postoperative complications. All predicted postoperative variables were also useful predictors for postoperative complications. Recently, a study also showed that predicted postoperative product, predicted postoperative DLCO, and American Society of Anesthesiology (ASA) score are independent predictors of a need for postoperative ICU admission.22
DLCO and exercise are good predictors of postoperative complications. The predicted postoperative ΔDLCO% can reflect DLCO and its response to exercise testing, suggesting that it is a potentially useful predictor of postoperative complications. The at-rest DLCO is sensitive enough to detect emphysema, but not sensitive enough to detect mild emphysema.23 Thus, in the face of mild disease with slight reduction in alveolar capillary surface, the remaining capillaries, with their ability to distend, might be recruited to replace capillaries involved in the emphysematous lesion, yielding a normal DLCO.24 In those patients, measuring DLCO during exercise may detect the abnormally reduced alveolar capillary surface and improve the sensitivity of DLCO for detecting emphysema, as suggested by Gelb et al.25 In the present study we defined a new useful index, the measured product, obtained by multiplying the preoperative percent-of-predicted FEV1 by the preoperative percent-of-predicted DLCO to predict postoperative complications.10,26 The measured product has advantages similar to that of the predicted postoperative product, and the measured product was also useful in predicting postoperative complications.
The patients with complications in our study were more likely to have COPD, more pack-years of smoking, and to be older than the patients without complications. In our previous study the clinical variables were found to be good for predicting postoperative complications.9 The diffusion heterogeneity index is elevated in smokers, and is correlated with age in smokers and pack-years of smoking.27 Smoking causes abnormalities including ground-glass attenuation, micronodules, and diffuse emphysematous changes.28 Inflammation and fibrosis in small airways probably account for the elevated diffusion heterogeneity index in smokers.27 Increasing breath-hold time improves gas mixing in the lung, which decreases heterogeneity and hence decreases the diffusion heterogeneity index.7 Therefore, the diffusion heterogeneity index might be higher due to shorter breath-holding (because of dyspnea) in those who developed complications, but this potential effect was minimized because the target breath-hold time at rest was only 2 seconds.9
During exercise the diffusion heterogeneity index increased in patients with complications and decreased in patients without complications. Since DLCO is measured at maximal lung volume, both at rest and during exercise, the change in DLCO is more likely to be due to a change in perfusion rather than ventilation. If there is general recruitment of pulmonary capillary blood during exercise, then diffusion will become more homogeneous and diffusion heterogeneity index will decrease.29 On the other hand, if blood flow increases preferentially to existing perfused units during exercise, then diffusion becomes more concentrated in one region, and hence more heterogeneous, with a consequent increase in diffusion heterogeneity index. Therefore, an increase in diffusion heterogeneity index with exercise may be an indicator that the lung's response to stress will be toward hyperperfusion of lung units with consequent edema and cardiac dysrhythmias. This may explain the performance of the preoperative change in diffusion heterogeneity index in predicting postoperative complications.
Limitations
We used prophylactic interventions to decrease the risk of perioperative morbidity and mortality, including smoking cessation, breathing training, antibiotics, expectorants, bronchodilators, and weight reduction. Intraoperative management included limited anesthesia and thoracotomy time, intermittent hyperinflation to prevent atelectasis, better control of secretions, prevention of aspiration, and maintenance of bronchodilation. Postoperative measures included incentive spirometry, mobilization of secretions, early ambulation, cough encouragement, and adequate pain control.
Conclusions
The predicted postoperative variables (predicted postoperative product, measured product, and diffusion heterogeneity index) are potentially useful predictors for preoperative evaluation of candidates for lung resection, but these findings need to be confirmed in larger prospective studies.
Acknowledgments
We thank Kenneth Evans MD and Richard Finley MD for help in recruiting patients; Jim Potts PhD and Sundeep Rai MSc for their advice and help with the 3-equation DLCO technique; Sverre Vedal MD for supervising some of the exercise tests and for helpful advice; Hui-Wen Lin PhD for his help with the statistical analysis and figures; and Winston Shen MD for editing assistance.
Footnotes
- Correspondence: Jeng-Shing Wang MD MSc, Division of Respirology, Antai Medical Care Cooperation, Antai Tian-Sheng Memorial Hospital, No. 166 Min-Shiang Street, Kaohsiung 800, Taiwan. E-mail: wangjs6{at}hotmail.com.
-
This research was partly supported by a grant from the British Columbia Medical Services Foundation, which provided the analyzer and computer for the 3-equation DLCO; and by the Tuberculosis and Chest Disabled Veterans Association, which funded the purchase of the exercise equipment. Dr Wang was partly supported by a fellowship from the British Columbia Lung Association, and by the Vancouver General Hospital Foundation. This study was performed as part of Dr Wang's master's thesis in experimental medicine, University of British Columbia, Vancouver, British Columbia, Canada.
-
The authors have disclosed no conflicts of interest.
- Copyright © 2011 by Daedalus Enterprises Inc.









{kind=link}
{kind=link}