

Abstract
OBJECTIVE: To assess the endotracheal temperature and humidity and clinical effects of 2 models of a new heat and moisture exchanger (HME): Rplus, which has regular breathing resistance, and Lplus, which has lower breathing resistance.
METHODS: We measured endotracheal temperature and humidity in 10 laryngectomized patients, for 10 min each, with and without the HMEs. We sequentially tested 4 HME models (all Atos Medical, Hörby, Sweden), in randomized order: Rplus, Lplus, Provox Normal (the HME we regularly use and which we considered the reference HME), and Stomvent (an older HME model). We also assessed the short-term clinical and practical effects of the Rplus and Lplus in a prospective 3-week trial with 13 laryngectomized patients.
RESULTS: Rplus and Lplus had better humidification than Provox Normal (6.8 mg H2O/L, 4.3 mg H2O/L, and 3.7 mg H2O/L, respectively, P < .001), and no significant temperature difference. During the 3-week study period, 7 of the 13 patients reported noticeably lower mucus production with Rplus and Lplus.
CONCLUSIONS: Rplus and Lplus had better heating and humidification than Provox Normal. Although Stomvent also performed well, its design is less convenient for laryngectomized patients. Further HME improvement is still warranted and should focus on improving the HME's heating capacity.
Introduction
In laryngectomized patients, inspired air is not conditioned and filtered by the upper airways, because breathing occurs through the tracheostoma and the upper airways are bypassed. This bypass leads to the inspiration of relatively cold and dry air, and to the loss of water and heat through the stoma during expiration. This in turn increases the viscosity of airway mucus, which compromises normal mucociliary function and eventually leads to damage of the mucociliary epithelium.1–5 As a consequence, laryngectomized patients have chronic pulmonary complaints, including frequent involuntary coughing spells, excessive sputum production, and the need for repeated daily forced expectoration to clear viscous airway mucus.6
Some 20 years ago the first heat and moisture exchanger (HME) was developed for laryngectomized patients, to compensate for the loss of heating and humidification by the upper airways. The first-generation HMEs used corrugated paper as the core material, and regular HME use significantly reduced pulmonary complaints and improved quality of life.6–8 Subsequent-generation HMEs were developed, initially to improve patient adherence to therapy, by making the HME easily replaceable and independent of the peristomal fixation adhesive,9 and to improve the tracheostoma digital occlusion port that allows phonation.10 However, regular HME use does not always eliminate pulmonary complaints, possibly because the HME is not a full-fledged substitute for the upper airways and does not provide the physiologic endotracheal temperature and humidity attained in normal individuals.11–13
Heating and humidification by an HME is based on the condensation of expired moisture on the HME's core material (foam or paper impregnated with a hygroscopic salt such as calcium chloride). One of the limiting factors in HME design for laryngectomized patients is the HME's size, which should be small enough for the patient to wear comfortably. Therefore, in comparison to anesthesiology HMEs used during intraoperative or intensive-care mechanical ventilation, a smaller amount of the condensation material must be used (Fig. 1), with consequently less heating and humidifying capability. Because of evaporative cooling there is even a slight but important decrease in end-inspiratory temperature with the Provox Normal and the Provox HiFlow (Atos Medical, Hörby, Sweden) (−1.5°C and −1.0°C, respectively).14–17

The studied heat and moisture exchangers (HMEs). Top left: Standard HME used in anesthesiology and intensive care. Top right: Stomvent, with integrated adhesive. Bottom left: Provox Normal. Bottom middle: Rplus. Bottom right: Lplus.
Breathing resistance plays a more profound role in HMEs for laryngectomees than in anesthesiology HMEs. The breathing resistance of a laryngectomee HME should be comfortable, to promote adherence to therapy. The breathing resistance of the Provox Normal, which we regularly use, is generally well tolerated,9,18 but an even lower breathing resistance would be preferable, especially during physical activity or when used in combination with a cannula.
Two new HME models (Atos Medical, Hörby, Sweden), Rplus, which has regular breathing resistance, and Lplus, which has lower breathing resistance, were designed based on in vitro and in vivo knowledge from the Provox HME. The Rplus and Lplus were designed to increase the heating and humidification capacity while keeping the dimensions and breathing resistance in the same range as previous-generation HMEs. One engineering difference of the Rplus and Lplus is that, instead of using a spring for the speaking valve mechanism, the Rplus and Lplus use the recoil effect of a piece of foam sponge, which allows for more hygroscopic material within the given cassette space (Fig. 2). In laboratory experiments the humidification capacity of Rplus and Lplus appeared to be better than the previous-generation laryngectomy HMEs; however, in vitro measurements do not necessarily represent in vivo behavior,17 so we designed an in vivo study to investigate endotracheal temperature and humidity with the Rplus and Lplus, and to assess their clinical feasibility and effects. We compared the Rplus and Lplus to the Stomvent (the first corrugated paper HME for laryngectomized patients; Atos Medical, Hörby, Sweden) and the Provox Normal, to improve our understanding of the effects of the different designs on heating and humidification capacity, and to develop suggestions for further HME improvement.

The Provox Normal (left) uses a spring mechanism for the speaking valve, whereas Rplus uses the recoil of the hygroscopic foam material.
Methods
This study was approved by the Protocol Review Board of the Netherlands Cancer Institute, and written informed consent was obtained from all patients.
Heat and Moisture Exchangers
We compared Provox Normal (which has well known heat and moisture exchanging capacity)19–21 and Stomvent (an older model HME with a different design), to Rplus (which has a normal breathing resistance) and Lplus (which has a lower breathing resistance, comparable to that of the Provox HiFlow, which we did not test in this study).20 We considered the Provox Normal the reference HME. Table 1 shows the in vitro moisture loss and pressure drop, according to ISO9360-2;2001.1
Moisture Loss and Pressure Drop
All 4 HMEs are hygroscopic and passive and do not include antimicrobial agents. The hygroscopic salt is calcium chloride, with no preservatives. The volume of an HME is < 5 mL, so the dead space can be ignored, and the breathing resistance depends on the HME (see Table 1). All of the tested HMEs can be (re)placed with a separate peristomal adhesive or trachea cannula, except with the first-generation Stomvent, in which it is integrated in its adhesive base plate, and can only be replaced in total. To facilitate air-tight occlusion for speech with a voice-prosthesis, the Stomvent is conical, whereas with the Provox Normal phonation is achieved by pressing down the cover with a finger. In the Rplus and Lplus the occlusion port that allows phonation has a different valve mechanism, which is based on the recoil pressure from a foam sponge, instead of a spring, as in the Provox Normal and Provox HiFlow.
Endotracheal Temperature and Humidity
In 10 male laryngectomized patients (median age 70 y, age range 56–81 y) we measured tracheal temperature and humidity and pulmonary function. All the patients were physically able to participate, and although we did not specifically have it as an inclusion criterion, all were regular HME users. All the patients had received radiotherapy, had quit smoking, and were in long-term follow-up (median 8.0 y post-laryngectomy, range 1.9–19 y).
During the measurements, the patient was seated in a chair and asked to breath calmly. We punched a small hole in the peristomal HME adhesive, through which we passed the distal tip of the sampling catheter of the airway climate explorer, a device (described elsewhere17) custom-made for intra-tracheal temperature and humidity measurement. The 5-mm catheter probe was connected to a fast humidity sensor (RS92K, Vaisala Oyj, Helsinki, Finland). Both the catheter and the sensor housing were internally heated to 40°C to prevent condensation in the catheter or sensor. Temperature was measured by a thermocouple (MLT1402 T-type Ultra Fast Thermocouple Probe (IT-23), ADInstruments, Oxfordshire, United Kingdom) (response time 5 ms, accuracy ±0.1°C), which was just inside the distal tip of the catheter. Tracheal gas was drawn through the catheter at a constant 0.6 L/min.
The catheter tip was stabilized about 1 cm behind the opening of the trachea, to minimize intra-patient variability.19 Each measurement session included five 7-min sampling periods, separated by 5-min rest breaks. One sampling period was with open stoma breathing (ie, without HME), and the other four were with the 4 studied HMEs: Provox Normal, Stomvent, Rplus, and Lplus. The 5 sampling periods were performed in randomized sequence.
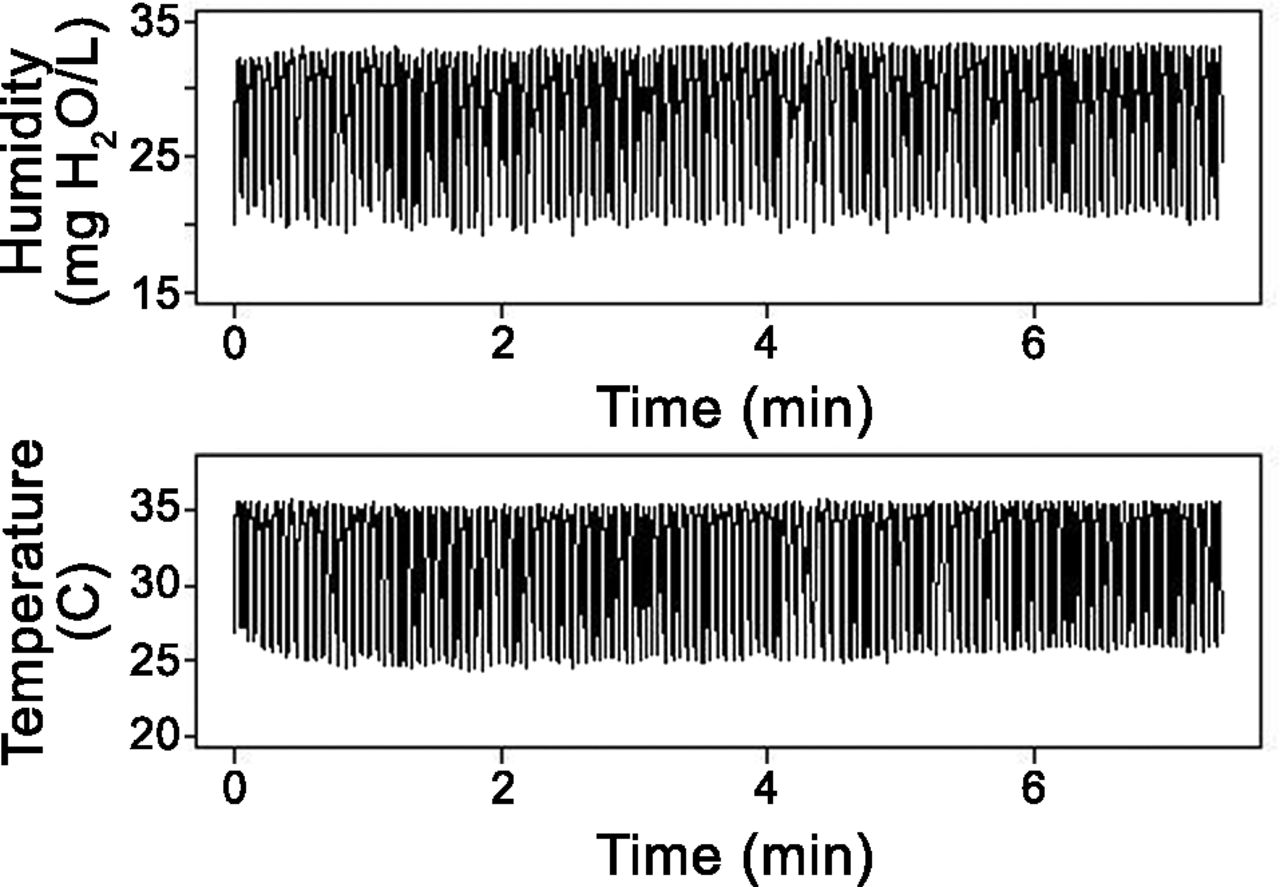
The first 5 min of each sampling period was an equilibration period, though the equilibrium condition may be reached much sooner (Fig. 3).19 All measurements were performed in room climate conditions, which we monitored with a calibrated temperature and humidity sensor (Testo, Almere, The Netherlands).

Humidity and temperature of tracheal gas from the moment of covering the open stoma with a Provox Normal heat and moisture exchanger. Equilibrium is usually reached within one minute.
Short-Term Prospective Clinical Feasibility
We separately investigated the short-term clinical and practical aspects of the Rplus and Lplus in a prospective observational feasibility study of patient comfort, experience, and adherence. We included 13 laryngectomized patients (12 male, 1 female, median age 62 y, age range 49–83 y). Four patients also participated in endotracheal temperature and humidity measurements. All the patients had received radiotherapy (9 preoperatively, and 4 postoperatively), had quit smoking, were in long-term follow-up (median 11 y post-laryngectomy, range 2−16 y), and were regular HME users. Four patients used the Provox Normal, three used the Provox HiFlow, three used the Provox Normal daily and the Provox HiFlow during physical exercise, and three used the Provox FreeHands HME (with automatic speaking valve) in alternation with the Provox Normal. With the exception of one patient, they all used HME day and night.
All the patients received both the Rplus and Lplus, and were instructed to use them during a 3-week period, in the same way they were accustomed to using the Provox Normal and/or Provox HiFlow. On the first day we assessed speech recordings with both the patient's accustomed HME and either the Rplus or the Lplus. We had each patient read aloud a standard Dutch text and produce an /a/ at a comfortable loudness 3 times for as long as possible, to measure maximum phonation time, first with their accustomed HME (Provox Normal or Provox HiFlow; if the patient was accustomed to the FreeHands HME, the Provox Normal was used instead). Then we repeated the phonation test with Rplus (instead of Provox Normal) or Lplus (instead of Provox HiFlow). An independent speech therapist compared and subjectively analyzed the recordings. At the end of the 3-week period, we used a study-specific questionnaire to ask the subjects about adherence to HME use, ease of use, and effects on voice and breathing.23
Data Processing, Data Analysis, and Modeling of Temperature and Humidity
Good-quality temperature and humidity measurements were available from all but one patient, whose breathing was so irregular without HME that individual breaths could not be identified, so we excluded that patient's data from the without-HME-breathing period. Our data processing and analysis methods were described previously.19 We analyzed the data from the last 2 min of each 7-min sampling period. The end-inhalation time points were identified with a peak-detection algorithm (Peaks Splus) in the statistics software (Splus 6.2 pro, Tibco, Somerville, Massachusetts).19 We used the inhalation and exhalation midpoints to calculate the duration of the inspiratory phase, the expiratory phase, and the entire respiratory cycle (Fig. 4). Breaths that had a minimum-versus-maximum humidity difference of less than 2 mg H2O/L were assumed to be due to cardiac oscillations17 and were merged with the adjacent breath. We graphically displayed the data as a check of the breath-identification procedure. We recorded the end-inspiratory and end-expiratory temperature and humidity.

Example of temperature and humidity of tracheal gas over 2 breaths. The total breath duration is defined as the time between the starts of 2 successive exhalations. The inspiratory time and expiratory time are approximated as the time between the midpoints of inhalation and exhalation.
We compared the end-inspiratory temperature, end-expiratory temperature, inspiratory time, expiratory time, and total breath duration data with a linear mixed-effects models, with a random patient intercept. We applied the inverse transform to the expiratory time to better approximate the normal distribution. All the results are presented in the original scale, and we applied the delta method to estimate the standard errors on the same scale. We anticipated that room temperature would influence end-inspiratory temperature, but the range in room temperature was too small for that association to be determined, so room temperature was not included in the model. We expected inspiratory humidity to depend exponentially on inspiratory time because of the sensor's response time, which is not sufficiently short, compared to the inspiratory time, so we used a non-linear exponential-decay mixed-effects model to simultaneously analyze inspiratory and expiratory humidity. This model estimated the initial humidity values, the decay rate (which represents the reaction time, in seconds), and the asymptotic humidity minimum at an infinitely long inspiratory time. The asymptotic humidity minimum was linearly related to room humidity. Using the estimated inspiratory time from the mixed-effects model for the inspiratory time, the clinically observed inspiratory humidity is calculated as:
This formula represents the exponential decay of inspiratory humidity as a function of inspiratory time with the reaction time (decay rate) from the maximum humidity toward the asymptotic humidity minimum, corrected for room humidity. The asymptotic humidity minimum, initial humidity, and inspiratory time are all dependent on HME type, with patient as the random grouping variable.24 The reaction time (decay rate) is dependent only on HME type (ie, fixed for all patients). Because of the cyclic nature of breathing, modeling the inspiratory humidity also provides an estimate for expiratory humidity. In particular the end-expiratory humidity is equal to the initial inhalation humidity (ie, when inspiratory time = 0), so expiratory humidity = initial humidity.
The short-term clinical study was mainly descriptive because of the small sample size and its observational design, so we did not statistically analyze the results.
Results
Room Conditions
The median room temperature was 23.8 ± 0.3°C (range 22.7–23.9°C), the median room absolute humidity was 6.3 ± 0.2 mg H2O/L (range 5.9–6.7 mg H2O/L), and the median room relative humidity was 29.9 ± 1.1% (range 28.5–33.2%).
Inspiratory Time, Expiratory Time, Total Breath Duration, and Tracheal Temperature and Humidity
Table 2 shows the inspiratory time, expiratory time, total breath duration, tracheal temperature, and tracheal humidity data. The mean inspiratory time during open stoma breathing (without HME) was 1.26 s, which was longer than the inspiratory time during breathing with HME (1.04 s, P < .001). There was no difference in inspiratory time between the different HMEs. The total breath duration with the different HMEs corresponded to the breathing frequencies: 17 breaths/min with Provox Normal, 16 breaths/min with Lplus, 17 breaths/min with Rplus, 18 breaths/min with Stomvent), and 18 breaths/min without HME.
Inspiratory and Expiratory Time, Temperature, and Humidity
In comparison with breathing without an HME, all the HMEs increased the inspiratory and expiratory humidity (see Table 2). The Rplus increased inspiratory humidity more than the Provox Normal (6.8 mg H2O/L vs 3.7 mg H2O/L, P < .001). The moisture retention capacity of the Lplus was similar to that of the Provox Normal. The Stomvent and the Rplus had comparable end-inspiratory humidification.
When compared with open stoma breathing, the Provox Normal increased the expiratory humidity by 0.9 mg H2O/L (P < .001), whereas Rplus, Lplus, and Stomvent increased the expiratory humidity by 1.5 mg H2O/L (P < .001), 1.5 mg H2O/L (P < .001) and 1.3 mg H2O/L (P < .001), respectively.
The end-inspiratory temperature with the Rplus, Lplus, and Stomvent were similar to that during open stoma breathing, whereas with the Provox Normal the end-inspiratory temperature decreased by 1.5°C (P < .001). In contrast, in comparison to open stoma breathing, the Rplus, Lplus, and Stomvent increased the end-expiratory temperature slightly but significantly (P < .001), whereas Provox Normal had no significant effect.
The model we used to analyze tracheal humidity is a simplification of a complex reality, so to account for this simplification we studied the model with a manual analysis of the raw data.19 This analysis indicated that the mean end-inspiratory temperature and end-expiratory temperature differed on average by 0.14°C and 0.10°C, respectively, from the corresponding model estimates, and the inspiratory humidity and expiratory humidity differed by 0.24 mg H2O/L and 0.08 mg H2O/L, respectively.
Short-Term Clinical Study
Eleven patients used the Rplus and Lplus, both day and night, for 21 days, while 2 patients quit using the Rplus or Lplus after 2 weeks, due to uncomfortable breathing, compared to their accustomed HME (either Provox Normal or Provox HiFlow). Of the remaining patients, 2 other patients also experienced more difficult breathing with Rplus or Lplus, but had still tolerable breathing. Three patients thought breathing was easier with Rplus or Lplus. Six patients said they found no difference.
Analysis of the speech recordings found a soft squeaking noise at the initiation of closure/release of the phonation valve with the Rplus or Lplus. Otherwise, we found no relevant differences in speaking with the Rplus or Lplus, compared to the patients' accustomed HMEs.
After the 3-week testing period, 7 patients (54%) reported having less mucus production than with their accustomed HME, including one patient who previously did not use an HME at night, but did so during the study period. That patient had the largest reduction in coughing frequency (from 20 times to 5 times daily). Three other patients were able to quantify the reduction of mucus production: one patient reported a decrease in sputum production from 10 times to 3 times daily, one patient from twice daily to not at all, and one patient from once daily to not at all.
Compared to their accustomed HME, 7 patients (54%) preferred the Rplus (3 patients) or Lplus (2 patients), or both (2 patients). Three patients preferred their accustomed HME. Three patients had no preference.
Discussion
Our primary aim was to determine whether the Rplus and Lplus improve heat and moisture exchange capacity, in comparison with Provox Normal or Stomvent, and whether Rplus and Lplus are acceptable to patients in terms of short-term HME effect and clinical applicability. Our results indicate that Rplus and Lplus, which have more hygroscopic material in a similar size cassette, significantly improve heat and moisture exchange capacity. Both Rplus and Lplus performed better than Provox Normal. The Rplus had higher inspiratory humidity than Provox Normal, without the decrease in end-inspiratory temperature that Provox Normal (and also Provox HiFlow) is known to cause.17,19 The Lplus had inspiratory humidity similar to Provox Normal, but without Provox Normal's temperature-lowering effect, which is due to the heat-consuming evaporation of water droplets during inspiration. This was an important argument for the redesign of Provox Normal, and our findings clearly show that Rplus and Lplus do not lower the end-inspiratory temperature. Stomvent, which was the first HME designed for laryngectomees, had surprisingly good humidification and temperature, and was only surpassed by Rplus, with regard to inspiratory humidity.
Rplus had higher inspiratory humidity (6.8 mg H2O/L), which is almost double that of Provox Normal (3.7 mg H2O/L), probably because Rplus has more hygroscopic material in the space formerly taken up by the spring of the speaking valve in Provox Normal and Provox HiFlow. Rplus and Lplus have more hygroscopic material than Provox Normal or Provox HiFlow, but they also have more open pores, so the breathing resistance is comparable to that of the older models. More hygroscopic material increases the amount of water that can be stored and the total heat capacity, which provides warmer inspired air. As shown by Zuur et al,17 the inspired air is almost saturated during the whole inspiration. Only increasing the temperature can further increase the humidity, so a higher inspiratory temperature facilitates a higher inspiratory humidity.
In the present study, Rplus, Lplus, and Stomvent all increased expiratory humidity (about 0.5 mg H2O/L), compared to Provox Normal. It is possible that the higher temperature of the inspired air underlies the increase in expiratory humidity. Warming of inspired air along the respiratory tract moves the isothermal saturation boundary (ie, the point in the trachea at which the air is 100% saturated with water vapor [44 mg H2O/L]) cephalad.24 As the trachea stays warmer over a longer tract during expiration, the exhaled air contains more moisture. The Provox Micron HME, which we tested in a previous study, also increased expiratory humidity (2.0 mg H2O/L) and end-inspiratory temperature (1.1°C), compared to Provox Normal.21 In that study we postulated that there might be a relationship between the better moisture retention and the decreased sputum production that we observed. We reasoned that higher inspiratory and expiratory temperatures could result in optimal conditions over a greater extent of the respiratory tract (caudal from the isothermal saturation boundary), which would lead to less hyperactive mucous and goblet cells and thus reduce mucus production.21
In the present study we found reduced sputum production with Rplus and Lplus in roughly half of the patients. We did not clinically test Stomvent again, because of its practical drawback that replacing the Stomvent requires removing the whole device; it has an integrated adhesive, which makes replacing it cumbersome for the patient and can lead to greater skin irritation.25 Apparently, excessive sputum production (and possibly other pulmonary complaints) may be reduced by improving an HME's heating and the moisture retention, leading to generally improved and conditioned mucosa.
A drawback of Rplus and Lplus is the squeaking noise when the speaking valve is closed. Although our subjects did not mention this problem at the end of the 3-week study period, the squeak, though gentle and hardly audible, should be taken seriously, as it might inconvenience some individuals. Consequently, Rplus and Lplus will not be commercially available until the squeak has been resolved.
The present study offers relevant information for further development of HMEs, which is still needed. Although Rplus and Lplus have important improvements over Provox Normal, they still do not provide the subglottic temperature and humidity achieved by the upper airways during nasal or oral breathing in young and healthy volunteers or in head and neck cancer patients.12
The question arises of what further modifications would improve HME performance, considering the limited space available in an HME for laryngectomized patients. Additional (identical) core material would either increase the resistance or create an unacceptably bulky HME. Further improvement of the total HME performance should therefore focus on improving the heating performance. A good alternative to improving heat capacity without increasing breathing resistance might be the insertion of a pre-heating filter, as was serendipitously found recently in an in vitro assessment of the Provox Micron HME.21
Limitations
First, the results from the feasibility study are observational and represent the opinions of a few patients. Although these results cannot be extrapolated with certainty to a larger patient group, we think they offer important information about the first clinical implications of new HMEs. Second, the speech analysis could not be performed blinded because the squeaking noise of the Rplus and Lplus prevented blinded assessment. Third, the included patients were predominantly males, due to the higher incidence of laryngeal cancer in males.26 On the other hand, sex is not expected to influence endotracheal climate as much as other factors, such as age, radiotherapy, time after surgery, and smoking. Unfortunately, our small sample size does not allow for a meaningful multivariate analysis. Fourth, the model we used to analyze humidity is necessarily a simplification of a complex reality; however, the differences between the model and the manual analysis were never larger than the standard deviations in each variable (see Table 2).
Conclusions
Both Rplus and Lplus showed a considerable improvement over Provox Normal and Stomvent. Although Stomvent is comparable to Rplus, its design makes it less attractive because Stomvent's HME cassette is not replaceable without removing the entire peristomal adhesive. The improvements in the tracheal climate with Rplus and Lplus seem to provide a clinical benefit, as there was reduced sputum production in half of the patients after 3 weeks. Since there is still a gap between the normal subglottic physiological temperature and humidity and that provided by an HME, further improvement of HME design is still warranted, with a focus on improving heat exchange.
Acknowledgments
We thank Marcel van der Horst and Morgan Shehata, formerly affiliated with the Department of Medical Technology Development, Academic Medical Centre, University of Amsterdam, for technical support.
Footnotes
- Correspondence: Frans JM Hilgers MD PhD, Department of Head and Neck Oncology and Surgery, The Netherlands Cancer Institute, Plesmanlaan 121, 1066CX Amsterdam, The Netherlands. E-mail: f.hilgers{at}nki.nl.
-
This research was partly supported by an unrestricted research grant from Atos Medical.
-
The authors have disclosed no other conflicts of interest.
- Copyright © 2011 by Daedalus Enterprises Inc.









{kind=link}
{kind=link}
{kind=link}
{kind=link}