

Abstract
Pulmonary alveolar proteinosis is a rare but potentially treatable disease, characterized by impaired surfactant metabolism that leads to accumulation in the alveoli of proteinaceous material rich in surfactant protein and its component. Novel insights from an animal model aided the discovery of granulocyte macrophage colony stimulating factor (GM-CSF) antibodies as a pathogenetic mechanism in human pulmonary alveolar proteinosis. The vast majority of pulmonary alveolar proteinosis occurs as an autoimmune disease; less commonly, it is congenital or secondary to an underlying disorder such as infection, hematological malignancy, or immunodeficiency. The subacute indolent course of this disease often delays the diagnosis by months to years. Crazy-paving appearance in a geographic distribution is a characteristic feature of this disease visible on high-resolution computed tomography (CT). A definitive diagnosis, however, requires lung biopsy, which typically shows partial or complete filling of alveoli with periodic-acid-Schiff-positive granular and eosinophilic material in preserved alveolar architecture. Patients with minimal symptoms are managed conservatively, whereas patients with hypoxemia require a more aggressive approach. Whole-lung lavage is the most widely accepted therapy for symptomatic pulmonary alveolar proteinosis. Correction of GM-CSF deficiency with exogenous GM-CSF is an alternative therapy. The combination of a systemic treatment (GM-CSF) and a local treatment (whole-lung lavage) augmenting the action of one another is a promising new approach. As the knowledge about this rare disease increases, the role of novel therapies is likely to be better defined and optimized.
Introduction
Pulmonary alveolar proteinosis, first described by Rosen et al in 1958,1 is a rare pulmonary disease with a worldwide distribution. It is a syndrome of altered surfactant homeostasis, characterized by accumulation of periodic-acid-Schiff-positive proteinaceous material in the alveoli. The resultant disturbance leads to clinical manifestation ranging from asymptomatic disease to life-threatening respiratory failure.2 New insights gained from knockout mice models,3–5 nonhuman primates,6,7 and granulocyte macrophage colony stimulating factor (GM-CSF) autoantibodies in human pulmonary alveolar proteinosis suggest a causal role of GM-CSF in the pathogenesis.8,9 Although ongoing studies are still evaluating its role, recent data suggest that exogenous GM-CSF therapy (to treat GM-CSF deficiency) has potential in the treatment of autoimmune pulmonary alveolar proteinosis.10 This review summarizes recent advances in pathogenesis and treatment of this rare but potentially treatable condition.
Methods
For this review we searched the PubMed and Embase databases for reports on the epidemiology, clinical presentation, evaluation, assessment, pathogenesis, and treatment of pulmonary alveolar proteinosis, published in English, up to August 2010. We used free terms, including “pulmonary alveolar proteinosis,” alone and in combination with epidemiology, diagnosis, bronchoalveolar lavage, crazy paving, GM-CSF, autoimmune or idiopathic pulmonary alveolar proteinosis, and whole-lung lavage. We also reviewed the references of primary studies, reviews, case reports, and editorials. All the identified references were reviewed by one of us.
Epidemiology
Because of the rarity of pulmonary alveolar proteinosis, it is difficult to estimate its true incidence and prevalence. Initial studies reported the prevalence of autoimmune pulmonary alveolar proteinosis at 3.7 cases per million; however, recent reports described a higher prevalence of about 6.2 cases per million.9,11,12 That difference in prevalence estimates suggests that the disease has a geographical distribution, but more epidemiological data are required to confirm that suspicion.
In most reported series there has been a male preponderance, with a male-to-female ratio range of 2.1:1 to 2.7:1.12 The usual duration of symptoms prior to diagnosis is around 7–10 months.9,12,13 In a retrospective review of 410 cases, Seymour et al found a median age at diagnosis of 39 years, with the disease manifesting at a later age in the males. They also reported a bimodal pattern, with a peak age frequency in females of 25–40 years.12 Similar age distribution and male preponderance was also reported from China in 281 patients.13 However, in 2 recent reports of 223 and 38 cases from Japan and Korea, respectively, the mean age at diagnosis was 51 and 52 years, with no sex difference.9,14 There was a significantly lower proportion of smokers (57%) in the recent Asian report, than the previously reported prevalence of 72%, which suggests that smoking is only casually associated and that other factors may be involved in the etiology.9,12
Normal Surfactant Physiology
Surfactant phospholipids are synthesized and stored as lamellar bodies in alveolar type II pneumocytes. Upon exocytosis into the alveolar lumen they interact with surfactant proteins and organize into tubular myelin that forms a mono-layer or multi-layer at the air-liquid interface, which reduces the surface tension and prevents alveolar collapse.15 Approximately 70–80% of the inactivated surfactant is taken up by alveolar type II cells for recycling or catabolism. The remaining surfactant is phagocytosed and degraded by alveolar macrophages or enters the lymphatic stream.2 Thus, a balanced production and catabolism tightly regulates the surfactant homeostasis. GM-CSF, which is present in serum and most tissues, binds to its receptors on monocytes, macrophages, and alveolar type II cells to initiate the biological effect.3,16,17 In the lungs, GM-CSF stimulates the terminal differentiation of alveolar macrophages mediated by transcription factor PU.1 to enhance their capacity for uptake and catabolism of surfactant proteins and surfactant phospholipids.18–20 In the presence of high-affinity neutralizing immunoglobulin G (IgG) antibodies against GM-CSF, alveolar macrophages lose their ability for adhesion, chemotaxis, microbicidal activity, phagocytosis, and phagolysosome fusion, leading to disruption of surfactant homeostasis and accumulation within the alveoli.21–24
Pathogenesis of Autoimmune Pulmonary Alveolar Proteinosis
New insights from ultrastructural,25 biochemical,26,27 and functional investigations of bronchoalveolar lavage fluid (BALF) indicate that abnormal clearance, rather than the excessive production, of surfactant is the key mechanism in the pathogenesis of pulmonary alveolar proteinosis.2,28 The seminal discovery that knockout mice deficient in GM-CSF or its receptor developed lung lesions similar to pulmonary alveolar proteinosis, and the reversal of those abnormalities with GM-CSF therapy, suggested a potential role for exogenous GM-CSF.4,5,29 However, the presence of a normal GM-CSF gene and functionally intact GM-CSF receptor with downward signaling strongly argues against the role of absolute deficiency of GM-CSF as the pathogenetic mechanism in human pulmonary alveolar proteinosis.30,31 Subsequently, the discovery of systemic (serum) and local (BALF) neutralizing antibodies against GM-CSF in idiopathic pulmonary alveolar proteinosis but not in healthy controls, resulting in a virtual deficiency of functional GM-CSF, suggested that the pathophysiological abnormality may originate from the generation of autoantibody against GM-CSF.8 The strong association of GM-CSF antibodies in human autoimmune pulmonary alveolar proteinosis is further supported by the recent observation of pathology findings similar to human pulmonary alveolar proteinosis in nonhuman primates (Macaca fascicularis) after passively transferring highly purified GM-CSF autoantibodies from a patient with pulmonary alveolar proteinosis.6,7 Thus, the final common pathway appears to be the deficiency of functionally active GM-CSF. Additionally, the discovery of GM-CSF antibody in an indium tin oxide worker with pulmonary alveolar proteinosis raises the possible role of inhaled agents in the triggering and development of autoimmune pulmonary alveolar proteinosis, though this is speculative and needs confirmation.32
Pathology
The characteristic findings of pulmonary alveolar proteinosis on light microscopy in lung specimens include partial or complete filling of alveoli with diastase-resistant, periodic-acid-Schiff-positive, granular and eosinophilic lipoproteinaceous material, and relatively preserved alveolar architecture (Fig. 1).1 Abnormally enlarged alveolar macrophages and intracellular accumulation of surfactant-like material are also present. Lymphocytic infiltration, fibroblasts, and fibrosis occur occasionally. With anti-surfactant protein A immunostain, substantial accumulation of surfactant protein can be seen in the alveoli.26 Electron microscopic ultrastructural examination of BALF sediment shows amorphous debris and concentrically laminated phospholipid lamellar bodies (Fig. 2).25,33–35

Eosinophilic granular material filling alveolar spaces, with little reaction in alveolar walls (hematoxylin and eosin stain, magnification ×100).

Ultrastructural examination shows whorled lamellated surfactant bodies in the alveolar spaces (eosin-5-maleimide stain, magnification ×6450).
Classification
Pulmonary alveolar proteinosis is classified into 2 main types: congenital and acquired. The acquired form is subdivided into the autoimmune form and the secondary form (ie, due to an underlying disorder). Congenital pulmonary alveolar proteinosis occurs due to mutation in the SFTPB gene entailing a surfactant-protein-B deficiency, gene encoding for ABC transporter A3 and CSF2RB gene encoding GM-CSF receptor β chain.36–38 The majority of congenital pulmonary alveolar proteinoses are transmitted in an autosomal recessive manner.36,39 They characteristically present with an acute onset of rapidly progressive respiratory distress immediately after birth.
The acquired form is the most common in previously healthy adults. Because of the presence of anti-GM-CSF antibodies, the term “autoimmune pulmonary alveolar proteinosis” has been proposed for the idiopathic variety, which constitutes more than 90% of all reported cases of pulmonary alveolar proteinosis.8,9,12,21 Secondary pulmonary alveolar proteinosis is caused by underlying conditions that reduce the number of or functionally impair alveolar macrophages (Table 1).35,40–86
Etiologies of Secondary Pulmonary Alveolar Proteinosis
Clinical Features
The onset of clinical disease is insidious, with a subacute indolent course that often delays the diagnosis by months to years. This delay is secondary to the time required for sufficient surfactant accumulation in the alveoli to impair gas exchange. Dyspnea, isolated or in combination with cough, occurs in a majority of the patients. Occasional patients may also have white and gummy sputum production, weight loss, hemoptysis, or fever.87,88 Physical examination is usually unremarkable, although there may be inspiratory crackles, clubbing, and cyanosis.89 Approximately 10–30% of patients are asymptomatic at presentation,9,14,90 whereas others present acutely with rapid progression to respiratory failure.91–95 Acute and rapid progression can occur because of infection.12 Pneumothorax and cor pulmonale occur rarely.96,97
Diagnosis
Radiology
Chest radiograph typically shows bilaterally symmetrical ill-defined nodular or confluent alveolar filling pattern, with a perihilar or basal distribution,98 but the radiographic pattern can also be asymmetric,99 unilateral,1,100 peripheral, or lobar.1 Absence of cardiomegaly, of pleural effusion, and extent of abnormality disproportionate to the symptoms help exclude pulmonary edema, which is the most common cause of perihilar infiltrates.
High-Resolution Computed Tomography
High-resolution CT shows smooth inter-lobular and intra-lobular septal thickening superimposed on a background of ground-glass opacities, which produces the crazy-paving appearance that is characteristic of pulmonary alveolar proteinosis (Fig. 3).101,102 Accumulation of proteinaceous material in the air space adjacent to inter-lobular septa, and an interstitial fibrotic process, alone or in combination, have been proposed as a mechanism of crazy paving.103,104 The crazy-paving pattern is not pathognomonic of pulmonary alveolar proteinosis, and occurs in other infectious or non-infectious conditions.104–114 The subacute or chronic clinical course, absence of architectural distortion, smooth inter-lobular septal thickening, geographical distribution, and discordance between the clinical and radiological features help differentiate pulmonary alveolar proteinosis from other causes of crazy paving. In a study of 42 patients, Ishii et al115 reported differences in the pattern and distribution of ground-glass opacity on high-resolution CT, which help to differentiate secondary from autoimmune pulmonary alveolar proteinosis. They found a higher occurrence of basal distribution of ground-glass opacity and crazy paving in autoimmune pulmonary alveolar proteinosis; however, the ground-glass opacity tended to be patchy or geographic in autoimmune pulmonary alveolar proteinosis, in contrast to diffuse ground-glass opacity in the secondary variety.115 High-resolution CT is also useful to determine the extent of lung involvement and to assess the disease severity before treatment.102

High-resolution computed tomogram from a patient with pulmonary alveolar proteinosis demonstrates the characteristic crazy-paving appearance.
Bronchoalveolar Lavage
BAL, with its characteristic appearance and ultrastructure, is helpful in the diagnosis.116,117 Grossly the BALF may be milky and opaque, and settles into a thick sediment layer and a translucent supernatant (Fig. 4).118 The BALF contains phospholipids and surfactant proteins A, B, and D, and has relatively lower concentrations of phosphatidylcholine and phosphatidylglycerol.27,119,120 The most striking feature on microscopy is enlarged foamy alveolar macrophages engorged with diastase-resistant, periodic-acid-Schiff-positive intracellular inclusions.121
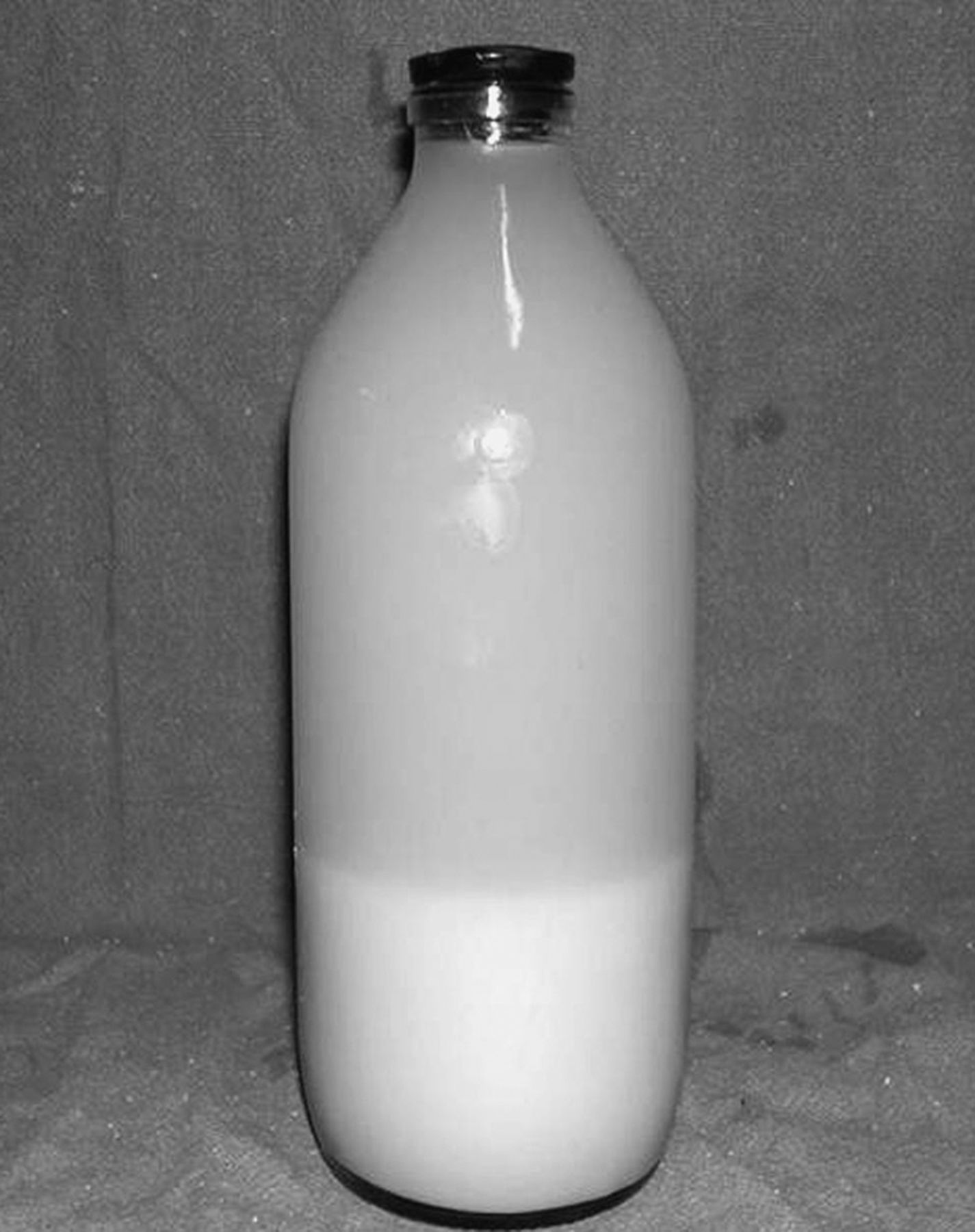
Lung-lavage fluid from a patient with pulmonary alveolar proteinosis layers into a thick sediment and a translucent supernatant.
On electron microscopy, abundant concentrically laminated structures called lamellar bodies are diagnostic of pulmonary alveolar proteinosis (see Fig. 2).25,122 On light microscopy, Papanicolaou stained BALF shows fat globules.116 In one study, a cutoff value of > 18 fat globules per slide was highly suggestive of pulmonary alveolar proteinosis.123 A confident diagnosis of pulmonary alveolar proteinosis can be made with the combination of milky and opaque BALF and characteristic findings on high-resolution CT.12 Tumor markers, mucin-like glycoprotein, and surfactant proteins also occur in the BALF, but their diagnostic utility is limited, as they are also present in other pulmonary diseases.124,125
Tissue Biopsy
The accepted standard for the diagnosis of pulmonary alveolar proteinosis is lung biopsy, via flexible bronchoscopy or surgery.1 Bronchoscopic biopsy can reliably establish the diagnosis and may obviate surgical lung biopsy,9,87,88,90 but, because of the patchy nature of the disease, a false negative result may be seen with bronchoscopic biopsy, with an additional risk of pneumothorax and hemorrhage.126
Granulocyte Macrophage Colony Stimulating Factor Autoantibody
GM-CSF autoantibodies are polyclonal and consist of IgG1, IgG2, and small amounts of IgG3 and IgG4.127 Healthy individuals can have low levels of GM-CSF autoantibodies, but the risk of pulmonary alveolar proteinosis is increased if the GM-CSF antibody level is > 5 μg/mL.7 The latex agglutination test is the most widely used test for the detection of GM-CSF antibodies. It has diagnostic sensitivity and specificity of 100% and 98%, respectively, so it is the test of choice for autoimmune pulmonary alveolar proteinosis.128
Severity Assessment
The clinical course of pulmonary alveolar proteinosis ranges from stable disease with persistent symptoms to progressive deterioration, or, occasionally, spontaneous improvement.9,12,100,129 In addition to the subjective assessment of symptoms, pulmonary function tests, exercise capacity, gas exchange, and serum and bronchoalveolar biomarkers are used to assess disease severity and to guide management decisions.
Pulmonary Function Tests
The most common spirometric abnormality in pulmonary alveolar proteinosis is restrictive defect, manifested by decreased vital capacity and lung volume.9,12,13 Alveolar filling is reflected by a disproportionately reduced diffusing capacity for carbon monoxide.9,13 Following lung lavage these variables improve, which suggests a good correlation with the disease severity.129
Gas Exchange
Hypoxemia without abnormal arterial pH or PaCO2, and increased alveolar-arterial oxygen difference (P(A-a)O2) that widens with exercise are prominent features of pulmonary alveolar proteinosis.9,12,129–131 These abnormalities occur due to intrapulmonary shunting of blood through poorly ventilated alveoli filled with proteinaceous material.130 Post-lavage improvement in these variables makes them convenient for monitoring the disease.129,130
Granulocyte Macrophage Colony Stimulating Factor Autoantibody Titers
Several initial reports suggested a relationship between serum anti-GM-CSF antibody titers and disease activity.132,133 Lin et al found a significant correlation between BALF (but not the serum GM-CSF antibodies) and other severity indicators, and subsequent requirement of therapeutic lung lavage.134 This could be related to compartmentalization leading to differences in BALF and serum antibody levels. Similarly, Seymour et al found no relationship between the serum anti-GM-CSF antibody concentration and disease severity or predicting the response to GM-CSF therapy.135 The neutralizing capacity of the antibody has been stated to be a more accurate marker of disease severity.136
Biomarkers
Abnormalities in the concentrations of proteins synthesized by the respiratory epithelium occur in pulmonary alveolar proteinosis, but their exact role in the severity assessment is uncertain.137 High levels of surfactant proteins, KL-6, and lactate dehydrogenase in serum and BALF have been described as evidence of severe disease.12,138–142 Several investigators have emphasized the value of these biomarkers in the diagnosis and severity assessment,27,142 but, due to their low specificity, they are seldom utilized. Similarly, tumor markers, such as squamous-cell carcinoma antigen, carcinoembryonic antigen, carbohydrate antigen 19-9, and cytokeratin 19 fragments, have been used in assessing pulmonary alveolar proteinosis.143,144 However, the clinical value of measuring these tumor markers in serum or BALF for diagnosis or severity assessment remains inconclusive.124
Treatment
The treatment of pulmonary alveolar proteinosis depends on the etiology (Fig. 5). Treatment of the congenital form depends on the patient's age at presentation, severity of symptoms, and anticipated disease course. In mild disease, supportive treatment may suffice.145 In severe disease, therapy may be individualized. Despite the technical difficulty, whole-lung lavage,146 lung transplantation,147,148 and heart and lung transplantation149 have been reported in congenital pulmonary alveolar proteinosis. The most effective treatment for secondary pulmonary alveolar proteinosis is treatment of the underlying condition.150
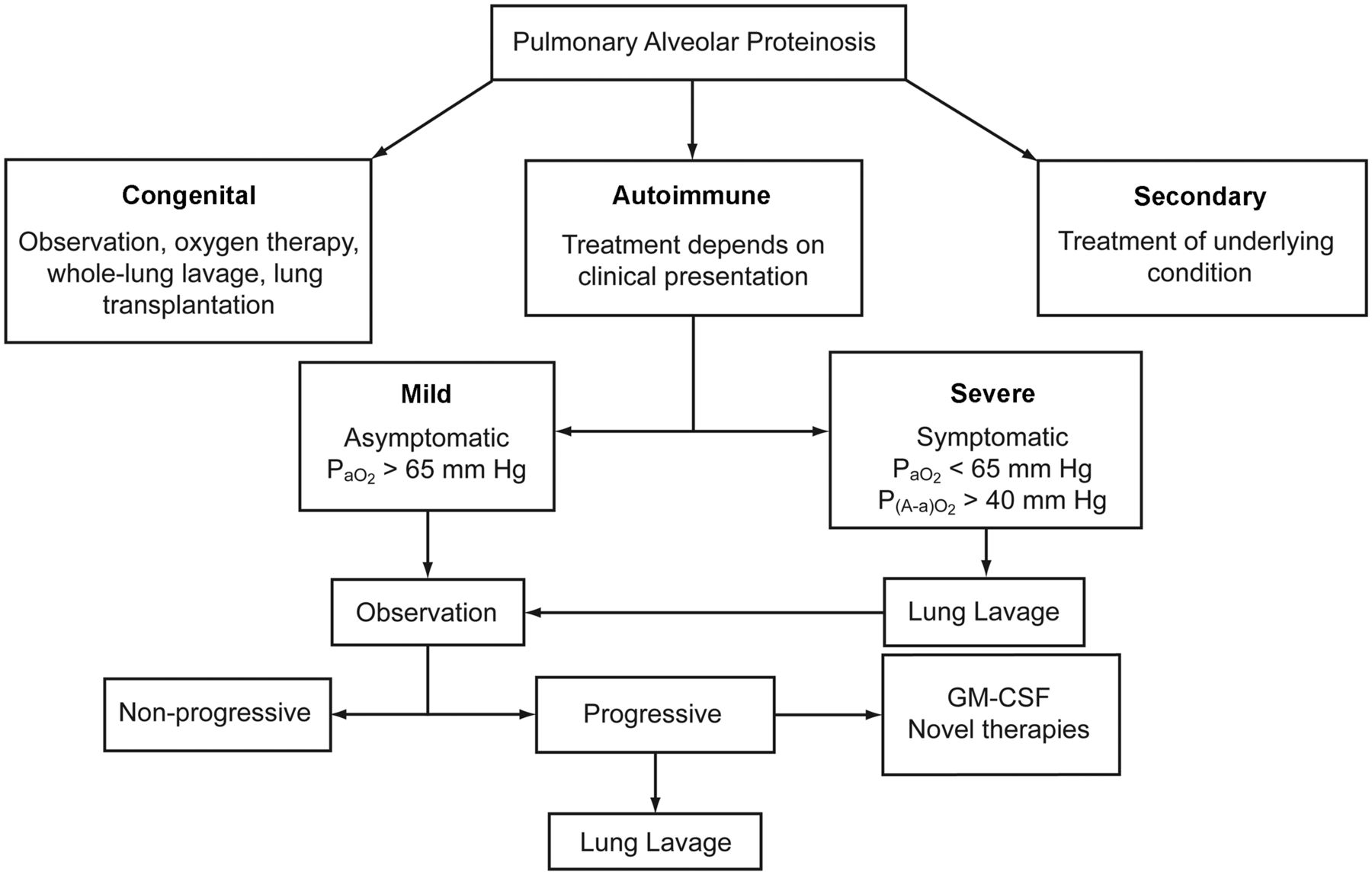
Treatment algorithm for pulmonary alveolar proteinosis. P(A-a)O2 = alveolar-arterial oxygen difference. GM-CSF = granulocyte macrophage colony stimulating factor.
Whole-Lung Lavage
Whole-lung lavage has been the most widely accepted and effective therapy for more than 4 decades. Beginning with “segmental flooding” to physically remove the accumulated material, then extending the procedure to the first successful whole-lung lavage under local anesthesia, Ramirez et al revolutionized the concept of whole-lung lavage in pulmonary alveolar proteinosis.151,152 Over the years this original procedure has been refined and modified to achieve good results with less procedural difficulty and fewer complications.95,126,153–172 The modifications include routine use of general anesthesia,153,154 larger lavage volume,154,155 lobar lavage,162 positional clearance,161 and chest percussion.159,161 Additionally, successful completion of bilateral sequential126 and simultaneous163 whole-lung lavage in the same session has been achieved. Special circumstances such as advanced pulmonary alveolar proteinosis or cor pulmonale may dictate modification of the technique, including hyperbaric oxygen,158 inhaled nitric oxide,167,172 and extracorporeal membrane oxygenation.170 In milder disease, lung lavage may be performed via flexible bronchoscopy in a conscious patient; however, the effectiveness of that procedure is unclear.173,175 Physical therapy (manual percussion, vibration, and chest compression) started during last the two thirds of infusion of saline and continuing till drainage can significantly increase the amount of material removed.159,174 Combination of physical therapy and gravity drainage optimizes the effective removal process. The benefits of whole-lung lavage are related to the physical removal of proteinaceous material and the local anti-GM-CSF antibodies, which restores the migration and phagocytic functions of alveolar macrophages.174–176
The major indication for and timing of whole-lung lavage is symptomatic disease with dyspnea that limits activity and progressive deterioration of arterial oxygenation.98 In some centers, PaO2 < 65 mm Hg, P(A-a)O2 > 40 mm Hg, or a shunt fraction > 10–12% are used as threshold values for therapeutic lung lavage.129,130 Clinical,129,130,177 functional,100,129,177 and radiological178 improvement are seen in approximately 80% of patients after the first whole-lung lavage, and the median duration of benefit can be as long as 15 months, but the majority require repeat lavage.12 Approximately 15% require lavage every 6 months, and lack of response is reported in less than 10%.126,130 Whole lung lavage provides only temporary symptom relief, without correcting the underlying defect, and has the additional disadvantage that it is a complex procedure that may require prolonged general anesthesia and has a risk of pneumonia, sepsis, acute respiratory distress syndrome, and pneumothorax.179–181 Despite these challenges, whole-lung lavage remains the therapy of choice and is associated with significantly better 5-year survival, compared to those who do not receive lavage.12
Exogenous Granulocyte Macrophage Colony Stimulating Factor Therapy
Based on the pathophysiology of pulmonary alveolar proteinosis, treatment aimed at relieving functional GM-CSF deficiency by administering exogenous GM-CSF or suppressing the neutralizing antibody has been utilized simultaneously or even as an alternate to whole-lung lavage. Several reports found favorable response with systemic (subcutaneous) or localized (aerosol) GM-CSF.10,132,136,142,182–191 Prompt improvement with resumption of GM-CSF in patients who relapsed with GM-CSF therapy suggests that disease resolution was not attributable to spontaneous remission and that GM-CSF does have therapeutic activity.183
Response is generally slow after GM-CSF therapy: the majority of patients show P(A-a)O2 improvement of ≥ 10 mm Hg only after 4–6 weeks.181–190 Despite the slower improvement in oxygenation with GM-CSF, the magnitude of therapeutic effect achievable with GM-CSF or whole-lung lavage may be similar.184 The observed delay in response is due to the time required for immature precursor cells to be recruited to the lung and stimulated by GM-CSF to differentiate into functional alveolar macrophages. The predictors of response with GM-CSF are yet to be determined, but one study found pre-treatment variables such as longer time from diagnosis, higher vital capacity, normal serum lactate dehydrogenase level, and higher plasma surfactant-protein-B level to be significantly associated with response to GM-CSF. Similarly, peak eosinophil count following GM-CSF was the only treatment-related variable associated with response.184 GM-CSF is generally well tolerated, but flushing, tachycardia, hypotension, musculoskeletal pain, dyspnea, nausea and vomiting, rigors, involuntary leg spasms, and syncope may occur following the first dose. These symptoms usually last for 10 min and do not recur with subsequent doses.192 Currently, one open-label and one randomized trial of GM-CSF in pulmonary alveolar proteinosis is underway, the results of which will clarify the future standard of therapy.
Novel Therapies
In patients who fail to respond to GM-CSF or whole-lung lavage (or require repeated lavage), novel therapies have been tried.2,193
Plasmapheresis.
Plasmapheresis to reduce the number of anti-GM-CSF antibodies and restore surfactant catabolism in alveolar macrophages is one novel approach. Plasmapheresis promptly improved symptoms, oxygen saturation, and radiographic appearance, with reduction in antibody titer, in one patient who was unresponsive to whole-lung lavage and subcutaneous GM-CSF.132 However, Luisetti et al found that lowering the GM-CSF level from 250 μg/mL to 156 μg/mL was not accompanied by clinical improvement after ten 1.5-L plasma exchanges in autoimmune pulmonary alveolar proteinosis with persistent disease, despite supplemental whole-lung lavage. They concluded that the small reduction in GM-CSF autoantibody level with plasmapheresis is not expected to have a therapeutic effect.194 Whether the combination of a systemic treatment (plasmapheresis) and a local treatment (whole-lung lavage) can act synergistically to lower the production of GM-CSF autoantibodies requires further evaluation.
Biological Therapies.
Reducing autoantibody levels by depleting B lymphocyte is another novel approach. Rituximab, a monoclonal antibody directed against the CD20 antigen of B lymphocytes, has been tested.195,196 Although decrease in anti-GM-CSF activity was evident within 3 months of rituximab infusion, the clinical response was evident only after 9 months.195 The delayed response may be related to recruitment of functional macrophages to the alveoli to stimulate surfactant clearance.
Summary
In the appropriate clinical setting, with typical chest radiographic and high-resolution CT findings, a diagnosis of pulmonary alveolar proteinosis can be established with the help of anti-GM-CSF antibodies and/or BALF and transbronchial lung biopsy. In selected patients, however, open or video-assisted lung biopsy may be required. Asymptomatic patients can be observed with periodic assessment. Patients with milder symptoms can be offered GM-CSF therapy or combined bronchoscopic lung lavage and GM-CSF therapy. In severe cases, whole-lung lavage with a double-lumen endotracheal tube under general anesthesia is the therapy of choice. With advancement of our knowledge of this rare disease, the roles of alternative therapies are likely to be better defined and optimized.
Footnotes
- Correspondence: Ritesh Agarwal MD DM, Department of Pulmonary Medicine, Postgraduate Institute of Medical Education and Research, Chandigarh 160012 India. E-mail: riteshpgi{at}gmail.com.
-
The authors have disclosed no conflicts of interest.
- Copyright © 2011 by Daedalus Enterprises Inc.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.
- 20.↵
- 21.↵
- 22.
- 23.
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.
- 35.↵
- 36.↵
- 37.
- 38.↵
- 39.↵
- 40.↵
- 41.
- 42.
- 43.
- 44.
- 45.
- 46.
- 47.
- 48.
- 49.
- 50.
- 51.
- 52.
- 53.
- 54.
- 55.
- 56.
- 57.
- 58.
- 59.
- 60.
- 61.
- 62.
- 63.
- 64.
- 65.
- 66.
- 67.
- 68.
- 69.
- 70.
- 71.
- 72.
- 73.
- 74.
- 75.
- 76.
- 77.
- 78.
- 79.
- 80.
- 81.
- 82.
- 83.
- 84.
- 85.
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.
- 93.
- 94.
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.
- 106.
- 107.
- 108.
- 109.
- 110.
- 111.
- 112.
- 113.
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.↵
- 119.↵
- 120.↵
- 121.↵
- 122.↵
- 123.↵
- 124.↵
- 125.↵
- 126.↵
- 127.↵
- 128.↵
- 129.↵
- 130.↵
- 131.↵
- 132.↵
- 133.↵
- 134.↵
- 135.↵
- 136.↵
- 137.↵
- 138.↵
- 139.
- 140.
- 141.
- 142.↵
- 143.↵
- 144.↵
- 145.↵
- 146.↵
- 147.↵
- 148.↵
- 149.↵
- 150.↵
- 151.↵
- 152.↵
- 153.↵
- 154.↵
- 155.↵
- 156.
- 157.
- 158.↵
- 159.↵
- 160.
- 161.↵
- 162.↵
- 163.↵
- 164.
- 165.
- 166.
- 167.↵
- 168.
- 169.
- 170.↵
- 171.
- 172.↵
- 173.↵
- 174.↵
- 175.↵
- 176.↵
- 177.↵
- 178.↵
- 179.↵
- 180.
- 181.↵
- 182.↵
- 183.↵
- 184.↵
- 185.
- 186.
- 187.
- 188.
- 189.
- 190.↵
- 191.↵
- 192.↵
- 193.↵
- 194.↵
- 195.↵
- 196.↵
- 197.↵
- 198.
- 199.
- 200.
- 201.
- 202.
- 203.↵









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}