

Abstract
COPD is a complex collection of conditions. All share the feature of limited expiratory air flow. It is a “disease” in the same sense as is “chronic renal failure.” Like most other chronic organ failure “diseases,” COPD has disparate causes, and patients are heterogeneous in their prognosis and response to treatment. Unlike many other diseases, the heterogeneity of COPD is just beginning to be described. A number of large trials funded by the National Institutes of Health and industry promise to refine the classification of COPD. Based on accurate diagnosis of COPD subtypes, novel treatments can be more effectively developed and implemented. The clinical implications of improved understanding of COPD heterogeneity will be better care and outcomes for COPD patients, which will depend on increased diagnostic accuracy and selective administration of treatments.
Introduction
Chronic obstructive pulmonary disease (COPD) has long been recognized as a heterogeneous condition. The classical distinction between so-called “pink puffers” and “blue bloaters” was intended to describe this heterogeneity.1 At least one reason the pink puffer/blue bloater classification has not proved useful clinically is that these descriptions fail to capture the spectrum of heterogeneity present in COPD. Recent studies suggest that COPD is heterogeneous in many ways, including etiology, pathology, physiology, and clinical features. Recent advances in the understanding of this heterogeneity have improved the development and implementation of therapies for COPD patients. Advances in understanding COPD heterogeneity hold the promise for increasingly personalized medicine that can be both more effective and more cost-effective.
Etiology
The most common cause of COPD is cigarette smoking. Smoking, however, is far from the only cause of COPD, with a number of other environmental factors playing important roles. Among these, exposure to environmental toxins, either fumes or particulates, are the most important.1 In some parts of the world, exposure to indoor air pollution, consequent to use of biomass for heating and cooking, is the major etiologic factor for COPD.2,3 In the developed world, particulate air pollution has a substantial adverse effect on lung function.4 Interestingly, the effect of particulates is observed both among smokers and non-smokers. Since the particulate burden present in cigarette smoke vastly exceeds that of air pollution, this suggests that separate mechanisms may be involved, at least to some extent, for cigarette-smoke-induced and air-pollution-induced COPD.
Factors other than exposures to inhaled toxins can also contribute to COPD risk. As many as 20% of asthmatics may develop fixed air-flow limitation over time.5 In these individuals, loss of lung function may be similar to that associated with smoking.6 Low birth weight has been associated with the development of COPD.7,8 While the mechanism is not definitively established, low birth weight is associated with a reduced maximally attained lung function in young adulthood.8 Presumably, compromise of lung development during gestation results in impaired lung growth and subsequent reduction in lung function.9 Lung function is maximal in young adulthood and declines “normally” with age in all individuals.10 Maximally attained lung function is inversely related to the risk for development of COPD. This suggests a lung-development/lung-growth pathway that accounts for increased COPD risk.
Other factors may compromise lung development and growth. In this regard, infants who suffer from bronchopulmonary dysplasia appear to be at risk for developing obstructive lung disease in adulthood.11 As the number of infants surviving early birth has increased, so has the incidence of bronchopulmonary dysplasia. Thus, it is possible that this may become an increasingly common cause of COPD in the future.12 Similarly, childhood infections are associated with compromised lung growth and COPD risk, although not all studies show this association.8,13
Low socioeconomic status is consistently found to be a risk factor for the development of COPD.14–17 The mechanisms are entirely unknown, as most epidemiologic studies “correct” for known risk factors. That is, socioeconomic status appears to be a risk factor independent of smoking status, birth weight, et cetera. Interestingly, low socioeconomic status is also associated with many other adverse health outcomes, and the mechanisms are equally poorly understood.18,19 The mechanism does not appear to be due to absolute wealth or access to healthcare systems, as poor health is seen among individuals with low socioeconomic status in prosperous countries where there is universal access to healthcare, in comparison to good health in individuals with high socioeconomic status in impoverished countries with dysfunctional healthcare systems.
Nutritional inputs probably contribute to the development of COPD, as they do to many other diseases. Starvation, per se, can contribute to the development of emphysema. This has been established both in animal studies20,21 and from human observations. Specifically, individuals with anorexia have evidence of emphysema, as assessed via computed tomography.22 In addition, young otherwise healthy individuals who died of starvation during the famine in the Warsaw ghetto in the second world war were observed to have severe emphysema at autopsy.23 Vitamin D deficiency has been associated with reduced lung function.24 To what degree starvation or other nutritional problems contribute to COPD etiology among general populations remains unknown.
Finally, genetic factors contribute to the development of emphysema.25 Genome-wide association studies, which can relate chromosomal loci to phenotypes, have identified a number of regions and potential candidate genes that are associated with COPD. For statistical reasons, genome-wide association studies can only ascertain the impact of relatively common variants within a population. Thus, the best established genetic factor related to COPD, alpha-1 antitrypsin deficiency, which is present in about one individual in 2,000 and accounts for about 2% of cases of emphysema, is generally undetectable via genome-wide association study. Other relatively rare candidate genes would also be undetected. Although there is not uniform consensus, other methods, including association studies, have identified additional candidate genes for COPD.26,27 The importance of these potential genetic risk factors remains to be fully established.
It is likely that genetic factors will interact in important ways, both among themselves and with environmental exposures. Thus, many individuals with alpha-1 antitrypsin deficiency who do not smoke maintain normal lung function, although some develop emphysema.28 Alpha-1-antitrypsin-deficient individuals who smoke, however, are at dramatically increased risk to develop emphysema. It is likely that complex interactions between the many genetic factors that impact emphysema and the environmental factors that contribute to risk will, at an etiologic level, result in a large number of different “causes” of COPD.
Pathology and Physiology
Several pathologic processes lead to structural changes that compromise expiratory air flow and, therefore, contribute to COPD.1,29,30 These pathologic processes may be present to variable degrees within a given individual, thus resulting in considerable pathologic heterogeneity.
Chronic bronchitis is defined as the excessive production of expectorated sputum. Sputum production, per se, however, is not strongly associated with air-flow limitation.31 Plugging of small airways with mucus may play a role, particularly in severe disease.32 Similarly, accumulation of secretions may compromise lung function during exacerbations.1 The major mechanism by which chronic bronchitis is thought to lead to air-flow limitation is by causing peribronchiolar fibrosis in small airways.32,33 In this regard, like all forms of fibrosis, fibrotic airways contract, thus narrowing the airway lumen. Consistent with this, airway circumference is reduced in patients with COPD and is an excellent anatomic correlate of air-flow limitation.34,35 In addition, the severity of airway fibrosis assessed histologically is associated with COPD severity.32 The cough and sputum production and the peribronchiolar fibrosis and airway narrowing are believed to be two separate consequences of the inflammatory process that characterizes chronic bronchitis. This relationship may account for the inconsistent association of air-flow limitation with the symptoms of cough and sputum production.
Emphysema is characterized by destruction of alveolar walls. This results in air-flow limitation because of the mechanisms that maintain small airway patency during expiration.29 The small airways, which have no supporting cartilage, maintain patency by two mechanisms. First, nearby alveolar walls are attached directly to small airways and can, by this relationship, tether them open. Destruction of the alveolar attachments results in loss of support, permitting airway collapse. Destruction of alveolar wall and loss of alveolar attachments have been related to air-flow limitation in emphysema.36 In addition, small airways maintain patency due to intra-luminal pressure.29 Pressure within the lumen of small airways is generated by the elastic recoil of alveolar structures. Loss of lung elastic recoil, which develops following alveolar wall destruction, results in collapse of small airways, particularly with forced exhalation.
In contrast to asthma, in which airway smooth muscle is hyper-reactive, airway smooth muscle tone in COPD patients is not markedly increased.37 Nevertheless, there is some airway tone, and relaxation of airways can improve expiratory air flow. Since airway smooth muscle tone can be targeted with currently available medications, whereas lung elastic recoil and peribronchiolar fibrosis cannot, this results in the interesting paradox that first-line therapy for COPD patients is aimed at the least important pathologic process contributing to air-flow limitation.
While expiratory air-flow limitation is readily measured with spirometry, this fails to capture the full physiologic impact of the pathologic processes in the lung. For example, individuals with COPD are variably susceptible to the development of dynamic hyperinflation,38,39 which ensues whenever respiratory rate increases, and there is insufficient time for the lungs to empty fully after each breath. As a result, each breath results in further hyperinflation of the lungs. With increasing volume, expiratory air flows generally increase so that a new equilibrium, at a higher lung volume, can be achieved. Because more mechanical work is required to breathe at higher volumes, this is believed to be a major cause of dyspnea among COPD patients.39
Dynamic hyperinflation, however, depends not only on air-flow limitation, but on the heterogeneity of air-flow limitation. Specifically, individuals whose lungs are inhomogeneous with respect to expiratory air-flow limitation will have some areas that are relatively normal and other areas that are relatively severely compromised. As respiratory rate increases, the normal areas may be able to empty fully, but the abnormal areas will hyperinflate. If very severe, the hyperinflated areas can compromise the ability of the normal areas to function, by preventing their full inflation. This is probably one mechanism that accounts for the markedly varying symptoms among individuals with similar air-flow limitation as assessed with spirometry. Similarly, inhomogeneities in the distribution of ventilation and perfusion can contribute to hypoxemia. The differences among individuals in the heterogeneity of ventilation-perfusion relationships probably accounts for differences in gas exchange among individuals with similar air-flow limitation.
Clinical Features
Patients with COPD differ in other pulmonary and extra-pulmonary manifestations of the disease. For example, while exacerbations generally increase as FEV1 declines, some individuals experience relatively frequent events, whereas in others exacerbations are relatively rare.40 Individuals who experience frequent exacerbations are at increased risk for poor outcomes and may respond differently to selected therapies.41
Patients with COPD are at increased risk to manifest extra-pulmonary morbidities than are similar-age smokers who do not have COPD (Table 1).42 These associated morbidities are often the major clinical problems faced by COPD patients. Current concepts suggest that an underlying inflammatory process may be the feature that links COPD to these comorbid conditions. Whether patients with COPD and specific comorbid conditions should be treated in special ways remains to be determined. However, recognizing that comorbidities are present is crucial, because optimal patient care requires that they be appropriately addressed.
Comorbidities Associated With COPD
Approaches to Describing COPD Heterogeneity
Recognizing that the FEV1 only partially captures the clinical syndrome of COPD suggests that additional measurements are required. Several approaches have been used to try to determine which additional measurements would be useful in this regard. Factor analysis is a statistical technique in which a group of variables that are determined in a population are related to each other. Variables that are strongly related to each other are not independent. In contrast, variables that are not related to each other presumably reflect different aspects of the population. By assessing how factors are related to each other, it is possible to identify factors that describe independent aspects of a population to provide a quantitative estimate of how well these factors accomplish that task. Several approaches to factor analysis have been undertaken for COPD.43–46 All these studies were limited by the way the population was selected and the variables collected. Nevertheless, several studies had similar findings (Table 2).47 Several studies of larger, more broadly selected individuals that will be assessed with more clinical measurements are in progress and are likely to provide improved insight into the factors required to describe the COPD population.
Key Variables in Principal Component Studies in COPD
That multiple independent measurements are required to describe a COPD population suggests that a single measure does not fully capture disease severity. Based on this concept, an index that combines multiple independent measurements should be a better prognostic measure than individual parameters. The BODE (body mass index, air-flow obstruction, dyspnea, exercise capacity) index is based on this concept and is a better predictor of mortality in the COPD population than any of its components.48 While the BODE index takes advantage of COPD heterogeneity, it combines different measurements into a single number and does not describe the heterogeneity per se.
A statistical approach to evaluate the heterogeneity of a population is cluster analysis.44 In this analysis, a population that can be described with a set of variables is assessed to determine if the variables clump into groups. This approach has been used to identify subsets of a variety of diseases, including asthma.49 This analysis has been applied to relatively small samples of COPD patients.43,50 Similar analyses are expected from the large ongoing observational studies in COPD.
Clinical Implications of COPD Heterogeneity
The ability to define heterogeneity within a COPD patient population permits the development and implementation of treatments that are specific for subpopulations. This strategy has, of course, been utilized for some time. Oxygen therapy, for example, is appropriate for individuals who are severely hypoxemic, but not for those with normal oxygenation.1 Defining clinical heterogeneity is crucial for the implementation of other therapies as well.
The National Emphysema Treatment Trial was a large randomized prospective clinical trial that compared volume-reduction surgery to medical management51 and found that for individuals with inhomogeneous disease, failure to respond to rehabilitation and a diffusing capacity of the lung for carbon monoxide (DLCO) of < 25%, surgical therapy is far superior to medical management with respect to survival, health status, and lung function. In contrast, for individuals with diffuse disease and good exercise capacity, outcomes are significantly better with medical management. Thus, characterization of several features that are heterogeneous in the COPD population is crucial in determining appropriate therapy.
Ascertaining COPD heterogeneity can also assist with development of new therapies. The development of roflumilast is particularly informative. Roflumilast is a phosphodiesterase 4 inhibitor.52 Agents of this class block the activity of phosphodiesterase 4, one of a family of enzymes that catalyze the breakdown of the nucleotides cyclic adenosine monophosphate and cyclic guanosine monophosphate. Phosphodiesterase 4 is present in the inflammatory cells believed to play crucial roles in COPD pathogenesis. Importantly, inhibition of phosphodiesterase 4 activity has anti-inflammatory effects in vitro and in animal studies. On this basis, phosphodiesterase 4 agents have undergone testing in human COPD populations. The roflumilast development program was based on demonstrating a beneficial effect on lung function and a reduction in exacerbation frequency. A consistent, although modest, effect was observed on lung function, as might be expected from an anti-inflammatory agent.53,54 In contrast, in neither of the initial phase-3 studies was there a significant effect on exacerbation frequency, although there was a trend.41,54 Post hoc analyses suggested that the ability of roflumilast to reduce exacerbation frequency was limited to a subset of COPD patients.41 This subset was characterized by individuals who had symptoms of chronic bronchitis and a history of exacerbations. This post hoc analysis led to additional phase-3 clinical trials that targeted that subset of COPD patients. Importantly, those studies demonstrated a significant benefit in exacerbation reduction,55 so roflumilast has now been approved in both the United States and Europe for the treatment of a subset of patients with COPD. It is likely that many other mechanistically based treatments in COPD will be beneficial in a portion of the COPD patient population. Identification of the appropriate target population will be crucial for drug development programs.
Implementation of Therapy
Identification of appropriate responding populations is also crucial to the use of therapies in practice. Just as volume-reduction surgery is helpful for some but contraindicated in others, drug therapy is likely to be beneficial in some and useless (or worse) in others. The ability to identify meaningful groups in this regard is an important aspect of personalized medicine. It is also an important strategy to reduce healthcare costs.
Diagnostic and Therapeutic Costs: The Paradox
Implementation of more sophisticated diagnostic testing has the potential to reduce healthcare costs. This seeming paradox—spending more results in less expense—depends on the effectiveness of the treatment within the population. That is, if a treatment is effective in all individuals in a population, it is reasonable to give everyone the treatment, and diagnostic tests are unnecessary. On the other hand, if a treatment is effective in a subgroup (Fig. 1), if everyone is treated, costs will be engendered by a large number of people who will not derive any benefit. In fact, if they suffer adverse events from the treatment, costs may further increase. A diagnostic test can reduce the costs of implementing a treatment by decreasing the number of people who are inappropriately treated. This has the potential for more than offsetting the costs of the diagnostic test, resulting in a net savings. This results in an interesting paradox, in that the costs for treating some individuals may go up, but the costs for the population may decline.
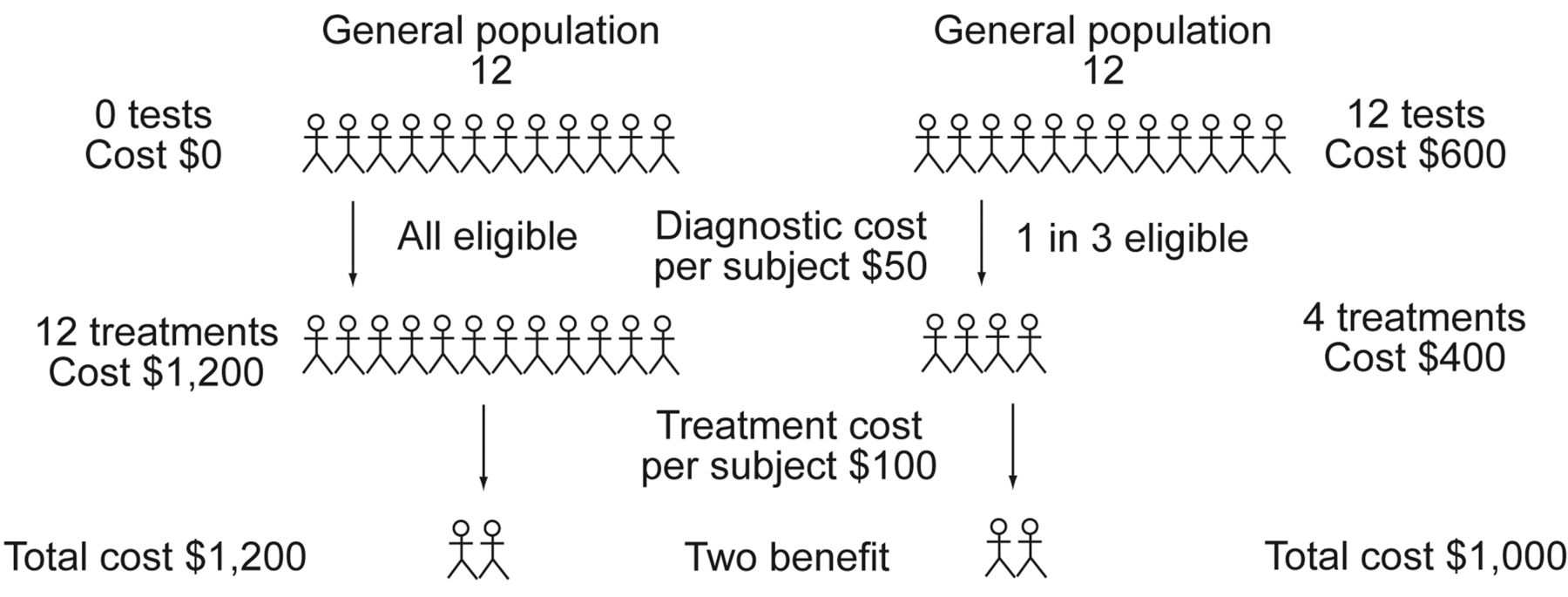
Effect of adding a diagnostic test and costs on overall costs. With no diagnostic tests, the cost of treating a population of 12 with a treatment cost of $100 per patient is $1,200. If the number-needed-to-treat is 6 (a relatively favorable ratio for many currently used treatments) only 2 patients benefit. Implementing a diagnostic test that costs $50 per patient adds $600 to the overall management. However, if it eliminates from consideration for treatment subjects so that number-needed-to-treat is 2, only $400 is spent on treatment, and the overall costs are reduced. Note that the cost per treated person increases from $100 to $150.
Overall Implications and Summary
COPD is a condition defined and characterized by a single physiologic limitation: decreased expiratory air flow. The causes and processes that lead to this abnormality are extremely heterogeneous. As might be expected, the clinical consequences are heterogeneous as well. Diagnostic techniques that can define the heterogeneity of the COPD population are now being applied in sufficiently large studies that the heterogeneity of COPD can be understood. Several of the recent advances in clinical COPD management have depended crucially on the ability to implement appropriate diagnostic strategies and define subgroups of COPD patients. It is almost certain that the heterogeneity of the COPD population will be increasingly refined. As this happens, diagnostic tests will be increasingly applied to the COPD population, and treatments will be increasingly personalized. This approach offers much hope for the COPD patient population and a challenge for the COPD care community.
Footnotes
- Correspondence: Stephen I Rennard MD, Division of Pulmonary, Critical Care, Sleep & Allergy, 985910 Nebraska Medical Center Omaha, Omaha NE 68198-5910. E-mail: srennard{at}unmc.edu.
-
Dr Rennard presented a version of this paper as the 26th Philip Kittredge Memorial Lecture at the 56th International Respiratory Congress of the American Association for Respiratory Care, held December 6–9, 2010, in Las Vegas, Nevada.
-
Dr Rennard has disclosed relationships with ABIM, Adelphi Research, Almirall/Forest, APT, AstraZeneca, Boehringer Ingelheim/Pfizer, BoomCom, Capital Research, CommonHealth, Decision Resources, Easton Associates, Equinox, Forest (Cory Paeth), Fulcrum, Gerson Lehman, GSK Eclipse, Guidepoint, Informed, Insyght, MedImmune, Novartis, Oriel, Pearl, Pfizer (Varenicline), PharmaVentures, Prescott, Propagate Pulmonary Reviews, Roche, Schering Plough, Smith Research, Talecris, UBC, the American College of Osteopathic Physicians, Asan Medical Center, American Thoracic Society, the COPD Foundation, Creative Education Concepts, Information TV, Nycomed, Otsuka, University of Washington, University of Alabama-Birmingham, Nabi, and Merck.
- Copyright © 2011 by Daedalus Enterprises Inc.









{kind=link}