

Abstract
BACKGROUND: Muscle oxygenation correlates with systemic oxygen uptake (V̇O2) in normal subjects; however, whether this relationship exists in COPD patients remains unclear. The purpose of this study was to investigate the influence of skeletal muscle oxygenation on V̇O2 during exercise in patients with COPD.
METHODS: Eight subjects performed an incremental cycle ergometer exercise test. We measured ventilation and pulmonary gas exchange with a metabolic measurement system. We also continuously monitored SpO2, and measured tissue oxygen saturation (StO2) in the vastus lateralis with continuous-wave near-infrared spectroscopy. We calculated the muscle oxygen extraction rate (MOER) based on SpO2 and StO2. In addition, we calculated Pearson correlation coefficients to examine the relationships between the V̇O2 obtained during exercise testing and the mean values of SpO2, StO2, heart rate (HR), and MOER for each 30-second interval of the tests. Finally, we analyzed the relationships between the peak V̇O2 and the slopes of HR/V̇O2, SpO2/V̇O2, StO2/V̇O2, and MOER/V̇O2.
RESULTS: With the increasing exercise intensity, many subjects showed a gradual decrease in StO2 and SpO2, but a gradual increase in HR and MOER. V̇O2 was negatively correlated with StO2 and SpO2, and was positively correlated with HR and MOER. However, peak V̇O2 was not correlated with any of the slopes.
CONCLUSIONS: V̇O2 is highly influenced by oxygen utilization in exercising muscles, as well as by blood oxygenation levels and cardiac function. However, the impact of skeletal muscle utilization during exercise on peak V̇O2 varied greatly among the subjects.
- COPD
- oxygen uptake
- oxygen utilization
- skeletal muscle oxygenation
- near-infrared spectroscopy
- muscle oxygen extraction rate
- rehabilitation
- exercise test
Introduction
The exercise tolerance of COPD patients is limited by ventilation and gas exchange, and by cardiac, skeletal muscle, and respiratory muscle dysfunctions.1,2 Early dyspnea and ventilatory insufficiency have traditionally been viewed as the main causes of such exercise intolerance.1 Many studies have shown that hyperinflation typically worsens air-flow obstruction and decreases exercise capacity.1–3 However, some patients are capable of performing many exercises despite having severe air-flow limitations.4 Leg fatigue is also commonly experienced during peak exercise in patients with COPD.5 These observations indicate that peripheral muscle alterations, such as poor oxidative capacity, atrophy, and weakness, increase the susceptibility to contractile fatigue and are common in patients with COPD.6–9
In 1997 the American Association of Cardiovascular and Pulmonary Rehabilitation, and the American College of Chest Physicians published the first evidence-based guidelines on pulmonary rehabilitation.10 Since this report, several additional guidelines on pulmonary rehabilitation have been published.11–13 These guidelines recommend lower extremity exercise training for improving the exercise tolerance of patients with COPD. It has been shown that unsupported endurance training of the upper extremities is beneficial for patients with COPD and should be included in pulmonary rehabilitation programs. In contrast, the existing evidence does not support the routine use of inspiratory muscle training, anabolic drugs, or nutritional supplementation for pulmonary rehabilitation.12,13 Collectively, these publications11–13 indicate that skeletal muscle function is important for improving exercise tolerance.
Recent developments in near-infrared spectroscopy (NIRS) have made it possible to noninvasively measure in vivo changes in oxygenated hemoglobin (oxy-Hb), deoxygenated Hb (deoxy-Hb), and total Hb of tissues.14 NIRS has previously been used to assess changes in blood volume, the balance between oxygen delivery (DO2) and O2 consumption in skeletal muscles, and tissue oxygenation during exercise. A number of studies have used NIRS to evaluate skeletal muscle in patients with heart and muscular diseases, diabetes mellitus, as well as lung disease.15 Patients with COPD have faster dynamics of muscle deoxygenation than their age-matched controls.16,17 Studies have also shown that muscle oxygenation in patients with COPD during exercise can be improved by bronchodilators,18 heliox (mixture of 79% He and 21% O2),19 and proportional assist ventilation.20 These NIRS-based observations suggest that a relationship exists between respiratory muscle work and peripheral muscle oxygenation in patients with COPD. It has been reported that NIRS-generated muscle oxygenation measurements correlate with systemic oxygen uptake (V̇O2) levels in normal subjects.21 However, whether this relationship exists in COPD patients with skeletal muscle dysfunction remains unclear. Accordingly, the purpose of this study was to better understand the influence of skeletal muscle oxygenation, heart rate (HR), and SpO2 on V̇O2 during exercise in patients with COPD.
QUICK LOOK
Current knowledge
Muscle oxygenation correlates with systemic oxygen consumption in normal subjects, but the relationship between muscle oxygenation and oxygen consumption in patients with COPD is not well described.
What this paper contributes to our knowledge
In patients with COPD, oxygen consumption is highly influenced by oxygen utilization in exercising muscles, blood oxygenation level, and cardiac function. The relationship between muscle oxygenation and peak oxygen consumption varies widely in this population.
Methods
Subjects
Eight male subjects with moderate to very severe COPD participated in this study. Individuals were diagnosed with COPD according to the Global Initiative for Obstructive Lung Disease (GOLD) criteria (FEV1/FVC < 70% and FEV1 percent predicted < 80%).13 The related COPD symptoms were stable at the time of the study, and no participants suffered from any cardiovascular, neurological, skeletal muscle, or other conditions that could alter their capacity to perform or influence the exercise test. The medical ethics committee at Kio University, Koryo-cho, Japan, approved the design of this study. All participants provided written informed consent. The characteristics of the subjects included in the study are shown in Table 1.
Characteristics of 8 Male Subjects With COPD
Study Design
Body anthropometry was performed, and measurements of resting lung function were obtained. Dyspnea was assessed using the Medical Research Council (MRC) breathlessness scale, consisting of 5 statements that describe nearly the entire range of respiratory disabilities, from no disability (grade 1) to complete incapacity (grade 5).22 All subjects were subjected to a symptom-limited incremental cycle ergometry test. A flow chart of this study is shown in Figure 1.

A flow diagram of this study. BMI = body mass index. MRC = Medical Research Council dyspnea score. V̇O2 = oxygen uptake. HR = heart rate. Oxy-Hb = oxyhemoglobin. Deoxy-Hb = deoxyhemoglobin. StO2 = tissue oxygen saturation. MOER = muscle oxygen extraction rate.
Pulmonary Function Tests
Spirometry was performed using a hand-held spirometer (AS-502, Minato Medical Science, Osaka, Japan), according to published recommendations.23 The data evaluated consisted of FVC, FEV1, and the Tiffeneau index (FEV1/FVC). Recorded values were compared with the values predicted for the adult Japanese population.24
Exercise Test
We carried out all tests on subjects under close medical supervision, and monitored the subjects' cardiac activities with electrocardiogram. We used an electromagnetically braked cycle ergometer (232CXL, Combi, Tokyo, Japan), with a pedal revolution rate of 50 revolutions/min. The subjects performed incremental exercises using the modified protocol of the American Thoracic Society/American College of Chest Physicians guidelines,25 which consisted of exercising at 10 W for 1 min, with the exerted work load increased thereafter by an additional 10 W every min until the subject reached voluntary exhaustion. We determined the subjects' V̇O2 levels (expressed as the mean mL/kg/min) breath by breath with a computerized metabolic cart (AE280S, Minato Medical Science, Osaka, Japan). Moreover, the peak V̇O2 was defined as the mean during the last 30 s of the highest work load achieved by the subject. We continuously estimated SpO2 (every 30 s) via pulse oximetry (Pulsox-M24, Konika-Minolta, Tokyo, Japan). We continuously measured HR of subjects with electrocardiogram.
Kinetics of Peripheral Muscle Oxygenation
During the exercise test we measured the kinetics of peripheral muscle oxygenation in the right vastus lateralis muscle of subjects, using a laser tissue blood oxygen monitor (BOM-L1TRW, Omegawave, Tokyo, Japan). Specifically, the NIRS probe was placed on the muscle approximately 14–20 cm from the knee joint. This instrument uses 3 light emitting diodes (wavelengths 780, 810, and 830 nm) and calculates the relative tissue levels of oxy-Hb, deoxy-Hb, and total Hb, according to the Beer-Lambert law. The absorption coefficients of Hb were based on previously reported data.26 The individual values were proportional to the Hb levels, which suggests that oxy-Hb, deoxy-Hb, and total Hb were mostly expressed in μmol/L.
We expressed the Hb concentrations in arbitrary units because they do not represent actual physical volumes. We calculated tissue blood oxygen saturation (StO2) from the oxy-Hb and total Hb values with the following formula:
For measurements, the distances between the incident point and the 2 detectors were 30 mm and 15 mm, which were selected because a previous study showed that the maximum measuring depth for the tissue blood volume and its oxygenation of the intra-soft tissue were approximately 15 mm and 30 mm from the surface of the skin, respectively.27 To demonstrate that subcutaneous fatty tissue had little influence on the intramuscular hemodynamics and oxygenation measurements, we performed a differential calculation from the measurements of the detectors. The detectors were fixed with tape after being shielded with a rubber sheet and vinyl. These data were imported into a personal computer at a sampling frequency of 10 Hz via an analog-to-digital converter (NR500, Keyence, Osaka, Japan). The integrated and mean values from 30-second intervals were calculated using the analog-to-digital converter's software (Wave Logger 1.03, Keyence, Osaka, Japan). The mean was calculated by dividing these values by the integral time.
Muscle Oxygen Extraction Rate
Oxygen transport variables included DO2, V̇O2, and the oxygen extraction rate (OER). It has been established that DO2 is determined by arterial oxygen content (CaO2) and cardiac output, whereas V̇O2 is determined by CaO2, venous oxygen content (CVO2), and differences in cardiac output. OER is determined by the ratio of DO2 to V̇O2.28 In this study, CaO2 and CVO2 were calculated from SpO2, venous blood saturation (SVO2), PaO2, and mixed venous oxygen pressure (PvO2) with the following formulas:
The terms (0.003 × PaO2) and (0.003 × PvO2) are typically negligibly small, particularly because OER is calculated using the following formula:
Moreover, in this study we calculated the MOER using the formula:
Statistical Analysis
Data analysis was performed using statistics software (SPSS 19.0, SPSS, Chicago, Illinois). The Kolmogorov-Smirnov test was used to evaluate the data distribution. We performed analyses with Pearson correlation coefficients (r) to examine the relationships between the V̇O2 values from the exercise test and the means of oxy-Hb, deoxy-Hb, total Hb, StO2, SpO2, HR, or MOER for each 30-second interval during the test. After we confirmed significant correlations between V̇O2 and HR, SpO2, StO2, or MOER, we obtained the slopes of HR/V̇O2, SpO2/V̇O2, StO2/V̇O2, and MOER/V̇O2 from the regression analysis. In some subjects, SpO2 was not normally distributed, but we performed the same analysis in order to estimate regression slopes in this study. We also analyzed the relationships between the peak V̇O2 and the slopes of HR/V̇O2, SpO2/V̇O2, StO2/V̇O2, and MOER/V̇O2 using Pearson correlation coefficients. A P value of less than .05 was considered statistically significant.
Results
Kinetics of Peripheral Muscle Oxygenation During an Exercise Test
In many of the subjects in this study, both the deoxy-Hb and total Hb levels gradually increased with exercise intensity, either immediately or during the test. In contrast, the levels of both oxy-Hb and StO2 gradually decreased during the test (Fig. 2). However, the oxy-Hb, deoxy-Hb, and StO2 levels changed somewhat during the test in subjects 2 and 6.
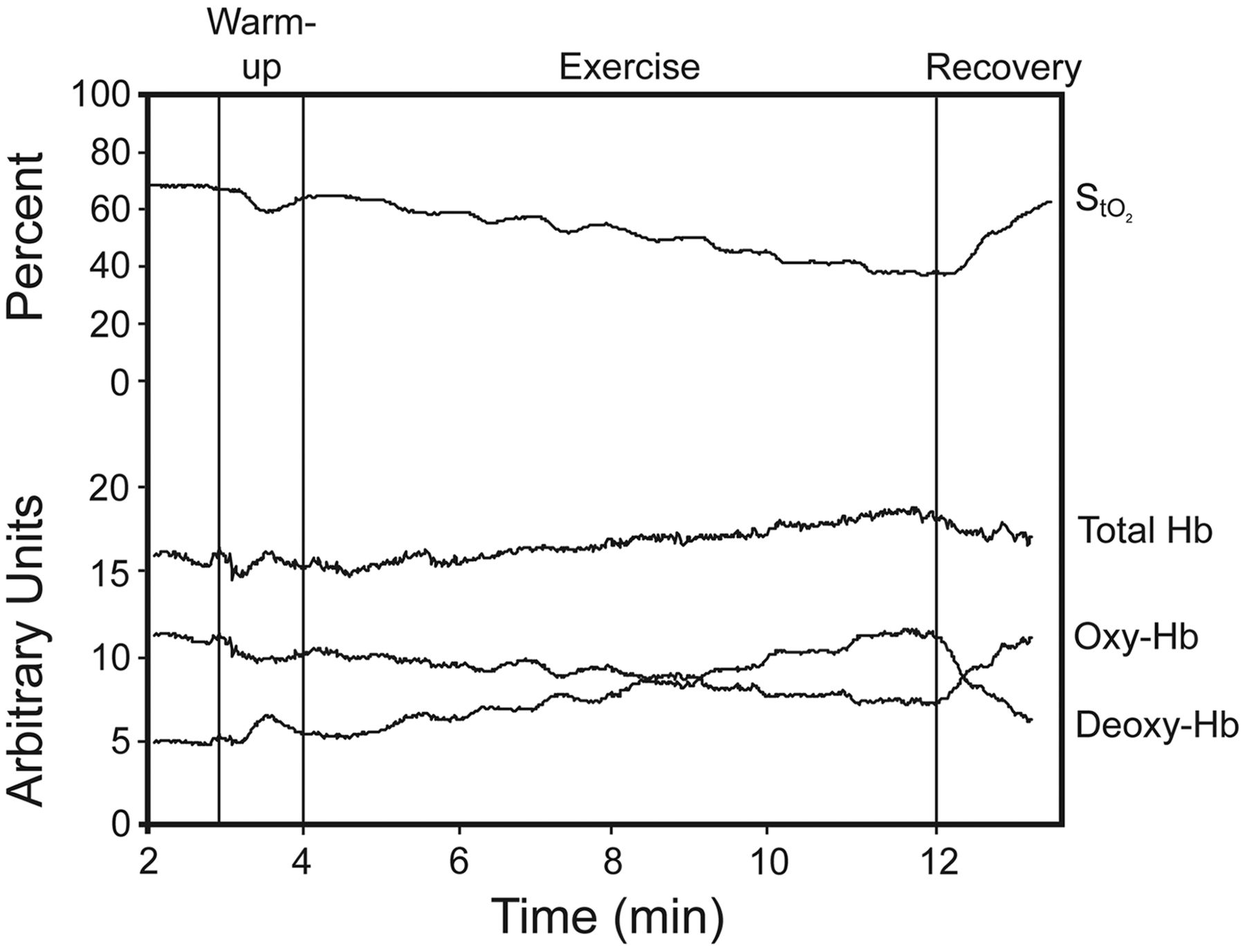
Typical tracing of changes in tissue oxygen saturation (StO2), oxyhemoglobin (oxy-Hb), deoxyhemoglobin (deoxy-Hb), and total Hb during exercise.
Relationships Between V̇O2 and Peripheral Muscle Oxygenation, Heart Rate, and SpO2
We calculated the relationships between V̇O2 and oxy-Hb, deoxy-Hb, total Hb, StO2, MOER, HR, and SpO2 per 30 seconds during the exercise test for each subject, using primary regression. V̇O2 was negatively correlated with StO2 (r = −0.473 to −0.979, P = .001 to .047) and SpO2 (r = −0.599 to −0.977, P = .001 to .029). In contrast, V̇O2 was positively correlated with deoxy-Hb (r = 0.706 to 0.978, P < .001), total Hb (r = 0.598 to 0.952, P = .001 to .039), MOER (r = 0.557 to 0.965, P = .001 to .047), and HR (r = 0.903 to 0.991, P < .001) of subjects. We found no obvious relationship between V̇O2 and oxy-Hb; in some individuals, there was a marked negative correlation in these parameters (r = −0.655 to −0.977, P = .001 to .029), but there was no apparent correlation in subjects 2 (r = 0.068) or 6 (r = −0.209) (Table 2).
Correlation Coefficients Between V̇O2 and Muscle Oxygenations, Heart Rate, and SpO2
Relationships Between Peak V̇O2 and the Slopes of HR/V̇O2, SpO2/V̇O2, StO2/V̇O2, and MOER/V̇O2
We also examined the relationships between V̇O2 and the slopes of HR/V̇O2, SpO2/V̇O2, StO2/V̇O2, and MOER/V̇O2. The influence of V̇O2 on the HR/V̇O2 slope is partially expressed in the cardiac response, the SpO2/V̇O2 slope in the respiratory response, and the StO2/V̇O2 and MOER/V̇O2 slopes in the muscle response. peak V̇O2 did not correlate with any of the slopes (Fig. 3). In subject 1 the HR/V̇O2, SpO2/V̇O2, and StO2/V̇O2 slopes were high and the MOER/V̇O2 slope was low, compared with most of the other subjects. However, in subject 2 the HR/V̇O2, SpO2/V̇O2, and StO2/V̇O2 slopes were low and the MOER/V̇O2 slope was high. Figure 4 displays the relationships between V̇O2 and HR, SpO2, StO2, and MOER for the different types of subjects (subjects 1 and 2). We determined that the severity of air-flow limitation was similar in both subjects, but peak V̇O2 was greater in subject 1 than in subject 2 (see Table 1). The slopes of HR/V̇O2 and SpO2/V̇O2 were lower, but MOER/V̇O2 was relatively higher in subject 1 than in subject 2.

Relationships between peak oxygen uptake (V̇O2) and the slope of heart rate/V̇O2, SpO2/V̇O2, StO2/V̇O2, and MOER/V̇O2. The muscle oxygen extraction rate (MOER) was calculated as (SpO2 − StO2)/SpO2 × 100(%). StO2 = tissue oxygen saturation. ○ Subject 1. ● Subject 2. △ Subject 3. ▴ Subject 4. □ Subject 5. ■ Subject 6. ◊ Subject 7. ⧫ Subject 8.

Relationships between oxygen uptake (V̇O2) and heart rate (HR), SpO2, tissue oxygen saturation (StO2), and muscle oxygen extraction rate (MOER) for typical subjects. ○ Subject 1: age 71 y, % predicted FVC 69.3%, % predicted FEV1 36.1%, peak V̇O2 17.0 mL/kg/min. ● Subject 2: age 74 y, % predicted FVC 65.5%, % predicted FEV1% 38.2%, peak V̇O2 10.9 mL/kg/min. The MOER was calculated as (SpO2 − StO2)/SpO2 × 100 (%). The severity of air-flow limitation was similar in both subjects, but peak V̇O2 was greater in Subject 1 than in Subject 2. The slopes of HR/V̇O2, SpO2/V̇O2 and StO2/V̇O2 were lower, but MOER/V̇O2 was relatively higher in Subject 1 than in Subject 2.
Discussion
Kinetics of Peripheral Muscle Oxygenation During an Exercise Test
The work rate of normal subjects is increased during exercise, and muscle oxygenation either remains constant near resting levels initially or decreases.29 With an increasing work rate, tissue oxygenation decreases linearly or exponentially below the resting value, followed by a leveling off as the person reaches exhaustion.30 These changes indicate there is a larger increase in oxygen extraction than in arterial blood flow during ramp load. In this study, most subjects with COPD exhibited similar changes (see Fig. 2). These results indicate that the balance between DO2 and O2 utilization in exercising muscle in subjects with COPD is similar to that in normal subjects. However, in 2 of the 8 subjects with COPD (subjects 2 and 6) there was little change in muscle oxygenation during exercise, and these subjects also had low MOERs (see Fig. 3).
Patients with COPD have been reported to have faster dynamics of muscle deoxygenation than their age-matched controls.16,17 Chiappa et al17 reported that the time constant ratio of O2 uptake to mean response time of deoxy-Hb concentration was significantly greater in patients with COPD after the performance of heavy-intensity exercise. It has been suggested that patients with COPD have slower kinetics of microvascular O2 delivery and impaired cardiovascular adjustments. Studies have also shown that muscle oxygenation in patients with COPD during exercise can be improved by bronchodilators,18 heliox,19 and proportional assist ventilation,20 all of which reduced the rate of onset of dynamic hyperinflation and diminished respiratory muscle work. These findings suggest that a fraction of the available cardiac output can be redirected from respiratory muscles to the peripheral muscles, as a consequence of respiratory muscle unloading; and that decreased muscle oxygenation during exercise may be due to insufficient DO2 in patients with COPD.
Some studies, however, show that blood flow in respiratory muscle is progressively reduced with increasing exercise intensity31; that blood flow redistribution from respiratory muscle to exercising muscle does not occur with heliox32; and that supplemental O2 does not improve muscle oxygenation, despite improved central O2 delivery in patients with COPD.33 These observations suggest that factors other than insufficient DO2 cause decreased muscle oxygenation during exercise in patients with COPD.
Another study showed that muscle oxygenation was decreased after endurance training34 and tapering,35 due to improved oxygen utilization in exercising muscle. Thus, it is important to differentiate between decreasing muscle oxygenation that is caused either by decreasing DO2 or increasing oxygen utilization.
In this study we found little change in the muscle oxygenation of subjects with COPD during exercise, and subjects 2 and 6 had low MOERs. These changes likely reflect the presence of an increased oxygen supply for covering decreased muscle oxygen extraction during the ramp load. Since there was little decrease in SpO2 in these subjects, we concluded that the oxygen supply may have been mostly provided by the arterial blood flow for increased oxygen uptake during exercise. This might compensate for the insufficient muscle oxygen utilization during exercise in these subjects.
Relationships Between V̇O2 and Peripheral Muscle Oxygenation
It has been reported that V̇O2 positively correlates with deoxy-Hb and total Hb, whereas it negatively correlates with oxy-Hb and StO2, during cycle ergometry in normal subjects.21,36 Furthermore, V̇O2 is reportedly negatively correlated with exercise muscle oxygenation during running.37 In this study we observed a similar relationship between V̇O2 and NIRS data in subjects with COPD (see Table 1), which suggests that the kinetics of muscle oxygenation reflect V̇O2 in both COPD and normal subjects.
V̇O2 is dependent upon the difference between arterial and venous oxygenation levels, as well as blood flow. Since a higher percentage of total blood flow is diverted to skeletal muscles during maximum exercise,38 it appears that the MOER is related to the OER. Thus, we found V̇O2 was significantly correlated with HR, SpO2, and MOER for each subject in this study.
Relationships Between peak V̇O2 and the Slopes of HR/V̇O2, SpO2/V̇O2, StO2/V̇O2, and MOER/V̇O2
Many studies have examined skeletal muscle dysfunction in patients with COPD.6,9,39 Peripheral muscle dysfunction may be attributed to deconditioning induced by inactivity, systemic inflammation, oxidative stress, blood gas disturbances, corticosteroid use, or reductions in muscle mass. In this study we found that peak V̇O2 was not correlated with any of the slopes of HR/V̇O2, SpO2/V̇O2, StO2/V̇O2, and MOER/V̇O2 (see Fig. 3). It is likely that the slopes were limited by ventilation due to arterial desaturation, because they had low peak V̇O2 with a low slope of SpO2/V̇O2 in subjects 4 and 7. However, subject 2 had low peak V̇O2 without a low slope of SpO2/V̇O2. The relationship between peak V̇O2 and the MOER/V̇O2 slope varied greatly. This relationship varied with the severity of skeletal muscle dysfunction in the subjects. Because they had low MOER/V̇O2 slopes, subjects 2 and 6 apparently had severely impaired muscle oxygenation dysfunction. In contrast, subjects 1 and 3 had high MOER/V̇O2 slopes, and therefore most likely had no or lightly impaired dysfunction.
Previous studies revealed muscle oxygen utilization was greater in patients with COPD than in unaffected subjects.40–42 This increase may be a compensatory mechanism for insufficient muscle oxygen supply during exercise in patients with severe COPD. It has been reported that peripheral skeletal muscle oxygenation is not compromised in patients with COPD during submaximal exercise, and suggested that limitations in exercise capacity are most likely a result of muscle disuse and poor lung function.43 Puente-Maestu et al reported that high-intensity training improves muscle oxygen capacity and oxygenation recovery kinetics, due to the increased presence of oxidative enzymes in patients with COPD.44
In the present study the MOER/V̇O2 slope varied greatly, which may indicate that various activity levels exist in patients with COPD. As shown in Figure 4, the HR/V̇O2 and SpO2/V̇O2 slopes were lower, but MOER/V̇O2 was relatively higher, in subject 1 than in subject 2. However, peak V̇O2 was greater in subject 1 than in subject 2 (see Table 1). These results suggest that V̇O2 was influenced by muscle oxygen utilization rather than cardiac function in subject 1, whereas subject 2 showed the opposite trend. Thus, the major factor of the cardiopulmonary response during exercise that differs between these subjects is possibly the muscle oxygen utilization function.
If a patient exhibits a decline in V̇O2 due to skeletal muscle dysfunction (eg, subject 2), skeletal muscle training may be the better management strategy from a rehabilitation standpoint. However, if a patient exhibits a decline in V̇O2 due to oxygen desaturation (eg, subject 1), supplemental oxygen may be the better management strategy, in addition to instructions for breathing control and relaxation techniques for improving exercise endurance.
We recognize that our study has limitations. We evaluated muscle oxidative function using StO2 and MOER for NIRS in the regional skeletal muscles, not in all exercising muscles, which is not ideal, since it has been shown that the oxidative response of muscles during exercise differs between exercising muscles.45 We could not accurately analyze muscle oxygenation dynamics and calculate MOER, because SpO2 is not equivalent to oxygen saturation measured from an arterial blood sample (SaO2); StO2 is not an adequate expression of SVO2; and local blood flow, cardiac output, and respiratory muscle V̇O2 were not measured.
Conclusions
Our findings indicate that V̇O2 is highly influenced by oxygen utilization in the exercising muscles, as well as by blood oxygenation levels and cardiac function, in subjects with COPD. However, the impact of skeletal muscle utilization during exercise on peak V̇O2 varied greatly for each subject.
Footnotes
- Correspondence: Kazuyuki Tabira PT PhD, Department of Physical Therapy, Faculty of Health Science, Kio University, 4-2-2 Umami-naka, Koryo-cho, Kitakatsuragi-gun, Nara, 635-0832, Japan, E-mail: k.tabira{at}kio.ac.jp.
This study was supported by joint research grant 18-1 from Kio University, Nara, Japan.
The authors have disclosed no conflicts of interest.
- Copyright © 2012 by Daedalus Enterprises Inc.









{kind=link}
{kind=link}
{kind=link}
{kind=link}