

Abstract
BACKGROUND: The impact of humidification devices on ventilatory and arterial blood gases parameters during noninvasive ventilation (NIV) remains controversial. The aim of the study was to compare the short-term impact of heat and moisture exchangers (HMEs) and heated humidifiers (HHs) during NIV for either hypercapnic or hypoxemic acute respiratory failure.
METHODS: Consecutive subjects receiving NIV were successively treated with HME and HH in randomized order for 30 min each. At the end of each period, arterial blood gases were measured and ventilatory parameters were recorded.
RESULTS: Eighty-one subjects were enrolled, of whom 52 were hypercapnic (with or without acidosis) and 29 hypoxemic. Minute ventilation was greater with the HME, in comparison with the HH (15 [12–18] vs 12 [10–16] median [interquartile range], P < .001), while PaCO2 was increased when using HME, indicating a dead space effect. This effect was observed in all subjects, but was more pronounced in hypercapnic subjects (PaCO2 62 ± 17 mm Hg with HME vs 57 ± 14 with HH, P < .001). In a subgroup of 19 subjects with respiratory acidosis, alveolar hypoventilation improved only with the HH. The amplitude of the dead space impact was a function of the degree of hypercapnia.
CONCLUSIONS: Use of an HME decreased CO2 elimination during NIV, despite increased minute ventilation, especially in hypercapnic subjects.
- noninvasive ventilation
- humidification
- heated humidifiers
- heat and moisture exchangers
- dead space
- alveolar hypoventilation
- acute respiratory failure
- COPD
Introduction
Noninvasive ventilation (NIV) delivered via a face mask reduces the need for endotracheal intubation and the subsequent risk of morbidity and mortality.1–3 NIV is particularly useful in patients with acute hypercapnic exacerbations of COPD.1,4,5 NIV failure, which has been reported in 20–50% of patients,6,7 is ascribed to inadequate CO2 removal8–12 and poor tolerance of the technique.6,7
It is well established that gases delivered through an endotracheal tube must be humidified, because dry inspired gases have deleterious effects.13,14 This statement is not so clear during NIV.15 However, there are several arguments favoring the use of humidification during NIV. First, the complications related to dry gases application are very frequent during NIV16 and may reduce tolerance of this technique. When NIV is delivered using a standard intensive-care ventilator, the upper airways are not bypassed, but receive dry inspired gases.17 The upper airways may be unable to humidify these gases adequately, particularly in mouth-breather patients or when high inspiratory flows are used. Another argument is the frequency of bronchial hyper-reactivity among patients requiring NIV,18,19 while dry gases are known to aggravate this state20 and can be used to measure airway responsiveness equally to methacholine and other cholinergic analogues or histamine.21 Two humidifying devices are commonly used with intensive care ventilators: heated humidifier (HH) and heat-and-moisture exchanger (HME). Both devices can adequately humidify inspired gas, even though leaks reduce inspired humidity with HME.17 HME devices are frequently used because of their simplicity and lower cost.22 Since they are placed between the Y-piece and the patient, they add substantial dead space to the circuit, leading to well known dead-space effects during assisted mechanical ventilation,23–25 and can also marginally increase the resistance to flow.26 The negative impacts of HME dead space during NIV were not found in a recently published study27 but have been previously demonstrated in 2 previous physiologic studies, including limited number of subjects.28,29 Jaber et al found that HME was associated with significantly reduced CO2 clearance, compared to HH, in spite of increased minute ventilation.28 We showed that the HME device causes a large increase in work of breathing, compared to HH, as well as an increase in minute ventilation.29 The number of subjects was too small to demonstrate an impact on arterial blood gases in our previous work. We thus addressed this question through a simple clinical study, with no assessment of subject effort, but including a large number of subjects with all degrees of severity or type of respiratory failure.30
QUICK LOOK
Current knowledge
Humidification during noninvasive ventilation impacts patient comfort and tolerance, and physical characteristics of these devices can affect minute ventilation requirements.
What this paper contributes to our knowledge
The use of a heat and moisture exchanger during noninvasive ventilation is associated with reduced carbon dioxide elimination, compared to heated humidification. The effect was more pronounced in patients with hypercapnic respiratory failure, high PaCO2, low tidal volume, and low PEEP.
Methods
The study protocol was approved by an independent review board (Comité d'Ethique de la Société de Réanimation de Langue Française). The subjects were given written information on the protocol and signed a consent waiver.
Subjects
Subjects were recruited in the medical ICU of Henri Mondor hospital over a one-year period. Inclusion criteria were recent dyspnea exacerbation and one of the following: respiratory rate ≥ 25 breaths/min, PaO2 < 60 mm Hg with room air, or arterial pH < 7.38. Exclusion criteria were a need for immediate endotracheal intubation, severe hypoxemia (FIO2 ≥ 0.80 to obtain SaO2 > 90%), respiratory rate < 12 breaths/min, pneumothorax, and hemodynamic instability.
Protocol
Consecutive subjects treated using NIV with pressure support were prospectively recruited. Ventilatory support was provided based on local recommendations.31 All subjects were ventilated with an ICU ventilator having inspiratory and expiratory lines. The HH was placed in the inspiratory line, as recommended by the manufacturer, and the HME was placed at the Y-piece. Each subject sat in a chair or in bed at an angle exceeding 30°, and the size of the interface was selected to fit the subject. Standard oronasal masks with different shapes and sizes were used to ensure a proper fit for each subject and to maximize comfort. No flex-tube was placed between the Y-piece and the mask. Hydrocolloid dressings were used to protect the skin. The subject placed the mask on his or her face before the procedure began, when possible. A head strap was used to hold the mask in place. Strap tension was minimized. The first breaths were made with no expiratory pressure, and an inspiratory pressure not exceeding 8 cm H2O. Inspiratory and expiratory pressures were increased in increments not exceeding 2 cm H2O. The expiratory pressure was gradually increased to 3 cm H2O in COPD subjects, and to a maximum of 10 cm H2O in hypoxemic subjects. The inspiratory pressure was increased to obtain an expired tidal volume between 7 and 9 mL/kg, or 6 and 8 mL/kg in COPD subjects. Low doses of sedative were given infrequently to agitated subjects. The physician and nurses explained the different periods and setting modifications to reassure the subjects.
An HME (Hygrobac, DAR, Mirandola, Italy) and an HH (MR850, Fisher & Paykel Healthcare, Auckland, New Zealand) with heated circuits were compared with a crossover design. HME dead space was 95 mL,32 while HME resistance, measured in a previous paper, were equivalent to HH inspiratory circuit resistances.29
We a priori separated 3 groups of subjects:
Subjects with hypercapnia and respiratory acidosis (usually corresponding to the initiation of NIV treatment)
Subjects with hypercapnia and without respiratory acidosis (usually corresponding to the stabilization of NIV treatment)
Hypoxemic non-hypercapnic subjects
Hypercapnia was defined as a PaCO2 exceeding 42 mm Hg. Acidosis was defined as a pH < 7.38. Hypoxemia was defined as a SpO2 < 90% when breathing room air. Subjects were ventilated for 30 min with an HH device and for 30 min with an HME device. The sequence of the humidification device was randomized. At the end of each period (during the 5 last minutes), the ventilatory parameters were recorded from the ventilator (respiratory rate and minute ventilation), and arterial blood gases were measured. The ventilatory settings were selected by the attending physician, and no changes occurred during the whole study time for these settings.
Arterial blood gas measurements were also available for 19 subjects in the respiratory acidosis group at baseline, immediately before the initiation of NIV.
Statistical Analysis
The primary outcome was the impact of humidification device on physiological parameters (arterial blood gases and breathing pattern). Descriptive statistics, including means, standard deviations, medians, and interquartile ranges, were used to summarize the data. Categorical variables were compared using the Mann-Whitney 2-sample rank sum test. Continuous variables were compared using the Spearman rank correlation. Continuous variables were not dichotomized, except PEEP level. We tested the carry-over effect to determine the impact of the sequence order (first NIV period with HH or with HME) and the impact of the period (first vs second NIV period). We analyzed the association between the ΔPaCO2 between the 2 humidification systems and PaCO2 under the HME with univariate analysis. We then used multiple linear regression to identify variables that made an important contribution to the variability of ΔPaCO2, to adjust for possible confounding variables. Despite being significant in the univariate analysis, the type of respiratory failure was not entered in the multiple regression model, due to its close relationship with the variable PaCO2 under HME. The model was checked for normality, linearity, homoscedasticity, and multicollinearity. Statistical analysis was performed using statistics software (Stata 8.2, StataCorp, College Station, Texas). A P value < .05 was considered significant.
Results
Eighty-one subjects were included in our study. The indications for NIV were acute hypoxemic respiratory distress (from unilateral pneumonia or ARDS) in 26 subjects, exacerbation of COPD in 28, post-extubation respiratory distress in 7, cardiopulmonary edema in 12, and other indications in 8. The sex ratio (M/F) was 54/27, the mean age was 63 ± 14 years, and the mean Simplified Acute Physiology Score II score was 41 ± 28. Ventilatory settings were as follows: the pressure support level was 14 ± 3 cm H2O, PEEP was set at 5 ± 2 cm H2O, and FIO2 was 0.51 ± 0.23.
Table 1 and Figure 1 present the impact of the humidification devices on arterial blood gases and respiratory parameters for the whole population. The results for the different populations (hypercapnia with or without acidosis and hypoxemia) are presented in Table 2.
Influence of the HME and HH Devices on Arterial Blood Gases and Respiratory Parameters of All Patients

Comparison of the PaCO2 at the end of each study period: heat and moisture exchanger (HME) versus heated humidifier (HH) in the entire study population. PaCO2 was significantly higher with the HME than with the HH (51 ± 17 mm Hg vs 47 ± 13 mm Hg, P < .001).
Influence of Humidification Device on Arterial Blood Gases and Ventilator Parameters in Patients With Hypercapnia and Acidosis (Early NIV), Hypercapnia (End of NIV), and in Patients With Hypoxemia
In all groups, the HME led to small but significant increase in PaCO2, despite significantly higher minute ventilation (see Table 2). These effects were more pronounced in hypercapnic subjects (see Table 3 and Fig. 2). Baseline arterial blood gases prior to NIV were available for 19 subjects with respiratory acidosis. CO2 removal improved over baseline only with the HH device, and not with the HME. Figure 3 shows the evolution of PaCO2 according to the device used in these subjects.
Factors Influencing the ΔPaCO2*

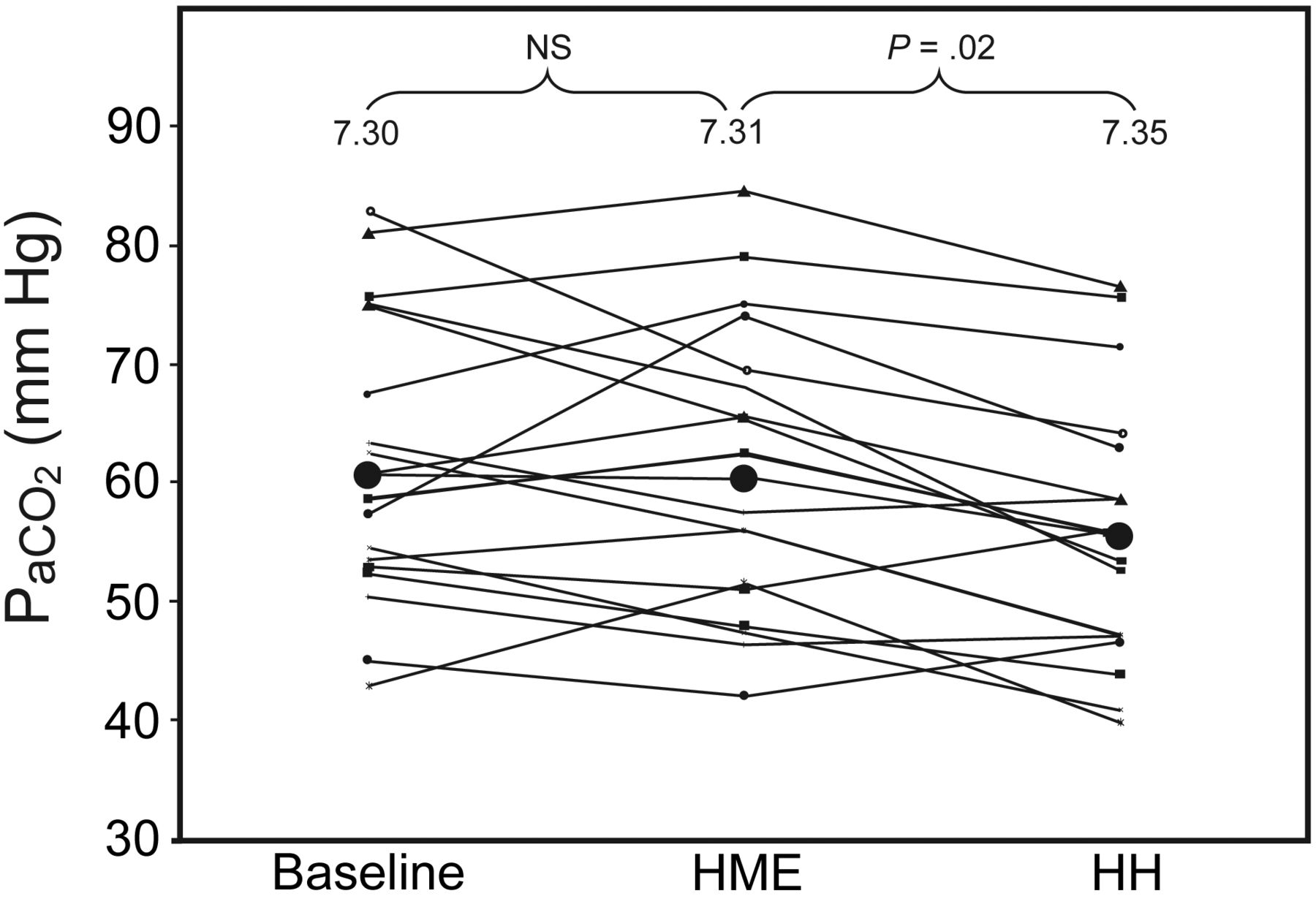
Comparison of the PaCO2 at the end of each study period: heat and moisture exchanger (HME) versus heated humidifier (HH) in hypercapnic subjects. PaCO2 was significantly higher with the HME than with the HH (62 ± 17 mm Hg vs 57 ± 14 mm Hg, P < .001).

Influence of the heat and moisture exchanger (HME) and heated humidifier (HH) devices on the pH correction in hypercapnic subjects with acidosis (n = 19); comparison with baseline values before NIV initiation.
The evaluation of a carry-over effect demonstrated that there is a period effect (first vs second), as expected due to the impact of NIV (P = .010), but no sequence effect (P = .70), indicating that beginning with HH or HME did not have any effect on the results for PaCO2 variations.
In univariate analysis, the most influential factors on the difference in PaCO2 between the 2 humidification systems (PaCO2 with HME – PaCO2 with HH) were the presence of hypercapnic respiratory failure, the level of initial PaCO2, and the expired tidal volume (see Table 3). Multiple regression analysis showed that PaCO2 level under HME was the best significant predictor of ΔPaCO2 after adjustment for PEEP level, expired tidal volume, and pH (Table 4).
Multiple Linear Regression Model for ΔPaCO2
Discussion
The present study assessed the effect of the main humidification devices on breathing pattern and arterial blood gases in a large number of consecutive subjects with various indications for NIV. The HME had a negative impact on CO2 elimination, compared to the HH (see Table 1). CO2 removal was reduced in all subject groups (see Tables 2 and 3), despite increased minute ventilation triggered by the added dead space of the HME. The effects were more pronounced in subjects with hypercapnic respiratory failure, high PaCO2, low tidal volume, and low PEEP (see Table 3).
Few data are available on humidification during NIV, and very few studies in the literature can be compared to the present study. Our group previously conducted a physiologic study comparing HH and HME devices during NIV in hypercapnic subjects.29 It showed that there is a significant increase in work of breathing, combined with an increase in minute ventilation, with the HME. However, a number of limitations due to experimental conditions made it impossible to evaluate the effect of the humidification devices on arterial blood gases in the previous study. First, the added dead space due to the pneumotachograph (almost 30 mL) may have reduced the difference in the volume of dead space of the devices studied. Second, the transdiaphragmatic pressure measurements using a double balloon eso-gastric catheter required patient cooperation. Because of this, patients with high PaCO2 and encephalopathy were excluded from the previous study. Patients were included after a mean ICU stay of 48 hours, and by then most of them had almost recovered from acidosis.29
In the present study the experimental conditions were similar to real-life clinical conditions, with no interventions except for changing the humidification device after 30 min. This large subject population made it possible to detect the deleterious effect of dead space on minute ventilation and breathing pattern in different categories of subjects (see Table 2).
In the group of subjects on NIV for decompensation of chronic respiratory failure (respiratory acidosis), there was a marked difference in median minute ventilation between the HH and HME devices (11.4 L/min vs 13.8 L/min, P < .001), respiratory rate, and PaCO2. The deleterious effect of dead space in this category of subject was present in the group of subjects with acidosis, corresponding to the initiation of NIV, as well as in the group without acidosis, corresponding to the end of NIV. Jaber et al28 reported the same HME dead-space effect in less severe hypercapnic patients. In their study, most of the patients had no acidosis and hypercapnia was moderate (PaCO2 46.0 ± 10.2 mm Hg at baseline).28
More striking was the finding that using the HME device for 30 min with NIV impeded pH correction in the group of subjects with respiratory acidosis, compared to baseline values (before NIV), while pH levels significantly increased with the HH device. Interestingly, many studies have reported that a decrease in CO2 during NIV is a strong predictor of success.8–12 The effect of HME in subjects treated for hypoxemic respiratory failure was less pronounced. These results are in agreement with those of Jaber et al.28
Our results were also in agreement with studies on intubated patients.25,33–36 With intubated patients on assisted ventilation, HMEs reduce CO2 elimination and increase minute ventilation and work of breathing, compared to HHs. This requires an increase in pressure support from 5 to 8 cm H2O, to compensate for the dead space of the HME.25,34,35 However, increasing pressure support during NIV is not always feasible because it can increase leaks and patient/ventilator asynchrony.37 In the current study the mean pressure support level was already 14 ± 3 cm H2O.
In a recently published study, Boyer et al compared HMEs with small dead space with HH during NIV and did not find differences in CO2 elimination.27 The absence of impact of dead space in this study may be explained by several factors. First, the difference of dead space between HME and HH was small (90 mL vs 33 mL when flex-tube was used and 38 mL vs 0 mL when no flex-tube was used). Also, the pressures used during NIV were very high (around 20 cm H2O of total inspiratory pressure or higher in patients with acute hypoxemic respiratory failure). These high pressures translated to high tidal volumes (around 750 mL in patients with exacerbation of COPD), which may be difficult to obtain in the real-life setting. Even if there is incontrovertible evidence that dead space impact exists during invasive and noninvasive mechanical ventilation,23–25,29,33–36,38–42 it is important to keep in mind that this effect is usually related to the amount of additional dead space.40 This impact may have little clinical importance, however, in specific conditions when small dead space HMEs are used.27
The effects observed in the present study were related to the dead space and not to the resistance of the humidification devices. Indeed, the inspiratory and expiratory resistance of the HME and HH devices were similar (2.5 vs 3 cm H2O/L/s), as previously reported.29 We used the same devices without flex tubes, as in our previous study.29 The physiologic dead space is usually around 150 mL,43 while the interface dead space is approximately 70 mL.44 The instrumental dead space of the HME device used in the present study was 95 mL. Instrumental dead space during NIV should be reduced as much as possible, since the aim of NIV is to reduce the work of breathing and to decrease PaCO2.45
In a previous study29 the HME device reduced the work of breathing but had no effect on minute ventilation when a PEEP of 5 cm H2O was applied. Interestingly, in the present study, mean PEEP was 5 ± 2 cm H2O (settings were performed by the attending physician). The negative impact of HME dead space on short-term physiologic parameters such as minute ventilation and arterial blood gases was present within these real-life settings.
The main limitation of the present study was that no conclusions could be reached regarding the impact of the HH and HME devices on the outcome and efficacy of NIV. However, in patients with marked hypercapnic encephalopathy and clinical signs of increased work of breathing, the dead space should be taken into account and the present results are relevant. An NIV session with a maximal reduction of the dead space should be attempted before proceeding to intubation, although this should not unduly prolong NIV and delay intubation if required. The other limitation of the present study was the absence of a period with no humidification. While this is possible with dedicated NIV turbine-based ventilators, it is not acceptable when using ICU ventilators because of the risk of increased bronchial hyperreacticity with dry gases and dryness of secretions.18–20 Another limitation of this study is the short time of the study periods (30 min each), which may have influenced the results.
Conclusions
In conclusion, the present study revealed that the dead space of the HME device had a short-term negative impact on CO2 elimination and minute ventilation in subjects treated with NIV delivered using an ICU ventilator. This impact was more pronounced in the hypercapnic population.
Footnotes
- Correspondence: François Lellouche MD PhD, Unité de Soins Intensifs de Chirurgie Cardiaque, Groupe de Recherche en Santé Respiratoire, Centre de Recherche de l'Institut Universitaire de Cardiologie et de Pneumologie de Québec, 2725 Chemin Sainte-Foy, Ville de Québec, Québec Canada G1V 4G5. E-mail: francois.lellouche{at}criucpq.ulaval.ca.
Dr Lellouche presented a version of this paper at the International Conference of the American Thoracic Society, held May 17–22, 2002, in Atlanta, Georgia.
The humidifiers for this study were supplied free of charge by Fisher & Paykel, which was not involved in the design or conduct of the study, collection, management, analysis, or interpretation of the data; or preparation, review, or approval of the manuscript.
Dr Brochard has disclosed relationships with Hudson and Fisher & Paykel.
- Copyright © 2012 by Daedalus Enterprises Inc.









{kind=link}
{kind=link}
{kind=link}