

Abstract
BACKGROUND: The application of CPAP has been used to minimize postoperative pulmonary complications after lung resection surgery. The aim of this study was to quantify both the CPAP effects upon lung function and functional capacity in early postoperative lung resection, as well as to evaluate if CPAP prolongs air leak through the chest drain.
METHODS: Thirty patients in the postoperative period of lung resection were allocated into 2 groups: an experimental group, consisting of 15 patients who underwent a 10 cm H2O CPAP, and a 15 patient control group, who performed breathing exercises. Arterial blood gas analysis, peak expiratory flow (PEF), respiratory muscle strength, spirometry, and 6-min walk test (6MWT) were assessed in the preoperative period, and repeated postoperatively on the first and on the seventh day (6MWT was repeated only on the seventh day).
RESULTS: Significant increases in PEF, muscle strength, and FEV1 between the first and seventh postoperative day were observed, both in the experimental and in the control group, whereas FVC and PaO2 increased significantly between the first and seventh postoperative day only in the experimental group. The average loss in 6-min walk distance (6MWD) from preoperative to postoperative day 7 in the experimental group was significantly lower than in control group. When comparing the 2 groups, only 6MWD was statistically different (P < .001). There was no air leakage increase through the drain with the early use of CPAP.
CONCLUSION: When compared to breathing exercises, CPAP increases the 6MWD in postoperative lung resection patients, without prolonging air leak through the chest drain.
- continuous positive airway pressure
- positive-pressure respiration
- respiratory function tests
- respiratory mechanics
- thoracic surgery
- walking
Introduction
Although operative mortality following thoracic surgery decreased over the last 20 years, postoperative pulmonary complications continue to occur with incidence rates as high as 49%.1 Because of this high incidence of postoperative pulmonary complications in thoracic surgery, substantial efforts have been aimed at predicting the most likely patients to develop such complications, and identifying techniques that could be used to prevent them.1,2 Despite greater awareness of physical therapy benefits used precociously after various types of surgical procedures, few studies have been performed regarding this practice.3–7 Noninvasive CPAP has been proposed to improve the recovery of functional residual capacity and to prevent postoperative pulmonary complications by means of increasing transpulmonary pressure in postoperative patients.8 This technique showed no hemodynamic adverse effects in patients following thoracotomy,7 and was associated with early and safe tracheal extubation after lung transplantation.5 Recent literature encourages the use of immediate postoperative CPAP to prevent postoperative pulmonary complications.8
Physiological and therapeutic effects of CPAP comprise improvement in arterial oxygenation, shift of the pressure-volume curve of the lung to the right, work of breathing reduction, and atelectasis reopening.9,10 Common side effects of CPAP include mask discomfort, skin abrasions, and irritation from device noise, among others.4,5
Clinical exercise testing is being largely used in clinical practice for 2 main reasons: its impact in the clinical decision-making process, and a growing awareness that resting cardiopulmonary measurements do not provide a reliable estimate of functional capacity.11 Several modalities of clinical exercise testing are used in clinical practice: some provide basic information, have low technical requirements, and are simple to deal with. The 6-min walk test (6MWT) is the most popular clinical exercise test, which has been used for postoperative evaluation of lung surgery.1,11 Therefore, a study to describe the effects of the early use of CPAP upon pulmonary function and 6MWT in postoperative lung surgery patients would add relevant clinical information. Although there are well known therapeutic effects of CPAP, its application in thoracic postoperative patients is likely to worsen air leakage through the chest tube. Thus, the aim of this study was to quantify CPAP effects upon both pulmonary function and functional capacity in postoperative lung resection, and to evaluate if CPAP prolongs air leak through the chest drain.
QUICK LOOK
Current knowledge
The use of CPAP following thoracic surgery reduces postoperative pulmonary complications.
What this paper contributes to our knowledge
Postoperative CPAP following lung surgery is associated with an increase in the 6-min walk test distance without increasing the risk of air leak.
Methods
The study was performed at the laboratory of respiratory physiology, State University of Rio de Janeiro, Rio de Janeiro, Brazil.
Patients
From March 2008 to November 2009 we enrolled 38 patients who underwent lung resection in the division of thoracic surgery of the State University of Rio de Janeiro, Rio de Janeiro, Brazil. We included patients aged 18–80 years in the postoperative period of elective lung resection (segmentectomy, lobectomy, or pneumonectomy) through posterolateral thoracotomy. The exclusion criteria comprised complications in the immediate postoperative period (need for mechanical ventilation after surgery, pneumonia, or hemodynamic instability), severe pain despite having received full analgesia in the postoperative period, and intolerance for CPAP application (less than 30 min).
According to the World Medical Association Declaration of Helsinki, the protocol was approved by the research and ethics committee of the University of the State of Rio de Janeiro, and written informed consent was obtained from all participants.
Procedures and Measurements
All surgeries were performed through posterolateral thoracotomy. Postoperative pain was controlled by epidural analgesia with morphine in the first 24–48 hours. After this period, tramadol and dipyrone were used.
The arterial blood sample to perform gas analysis was taken with the patient at bed rest, breathing room air for 5 min. The device used to analyze the sample was the Omni C System (Roche Diagnostics, São Paulo, Brazil).
Peak expiratory flow (PEF) was recorded through a peak flow meter (Assess, Health-Scan Products, Cedar Grove, New Jersey), while maximal inspiratory pressure and maximal expiratory pressure were measured by a manometer (Instrumentation Industries, Bethel Park, Pennsylvania).
Spirometry was performed according to the American Thoracic Society standards,12 using the Collins Plus pulmonary function testing system (Warren E Collins, Braintree, Massachusetts). Results were expressed in absolute values.
The 6MWT followed the American Thoracic Society guidelines.13 Tests were repeated twice, and the highest value was recorded. The subjects rested for one hour between tests. Vital signs monitoring was performed before and after the test. A digital oximeter (Onyx 9500, Nonin Medical, Plymouth, Minnesota) was used to measure heart rate and SpO2.
CPAP was applied to the patient in the sitting position via a face mask connected to an external CPAP valve (Acriflux, Criticalmed, Rio de Janeiro, Brazil), maintaining a 10 cm H2O PEEP.5,9,14 The system was kept pressurized by a high inspiratory flow of compressed air sent to the mask through a silicone tube, and the spring loaded valve, located at the outlet of the expiratory mask. This valve was set to maintain the desired pressure, according to the real-time pressure monitoring, using an analog manometer (Instrumentation Industries, Bethel Park, Pennsylvania). Oxygen supplementation was provided using an additional port when necessary. Two daily sessions of 30 min were performed (morning and afternoon). During each session the vital signs were monitored every 15 min, using a multiparameter monitor (ActiveX, Ecafix, São Paulo, Brazil), and control chest x-rays were taken every 24 hours in the first 7 postoperative days.
Study Protocol
The study protocol consisted initially in the preoperative evaluation (PRE) through arterial blood gas analysis, PEF, respiratory muscle strength, spirometry, and 6MWT.
In the immediate postoperative period, the 30 evaluated patients were allocated sequentially one by one into 2 groups: 15 in the experimental group, and 15 in the control group. Allocation was performed so that, sequentially, one patient was in the control group and the following was in the experimental group. The study was intentionally blinded from group allocation for physicians who administered the outcome measures of lung function and 6-min walk distance (6MWD). These physicians had access neither to the patient records nor to the places where the patients received CPAP or breathing exercises application. In both groups the patients performed the procedures twice a day, initiating on the first postoperative day. In the breathing exercises, the patients leaned forward in bed and performed 10 ventilatory cycles, with a 15–30 second interval between the cycles, or according to tolerance. The breathing exercises protocol was carried out as previously described by Pryor and Webber.15 Protocol was applied in both experimental and control groups for 7 days.
All post-surgery measurements were taken at 2 time points: on the first postoperative day (PO-1), before the CPAP or the breathing exercises, and on the seventh postoperative day (PO-7), except the 6MWT, which was repeated only on PO-7. On PO-1, all measurements were taken before CPAP or breathing exercises; while on PO-7, all of the measurements were taken after the protocol application.
In this study, prolonged air leak was defined as a persistent air leak through the chest drain for 5 days or more.16 If no air leak was detected, the chest tubes were removed when the drainage was less than 200 mL/24 h.
Data Analysis
SAS version 6.11 for Windows (SAS Institute, Cary, North Carolina) was used to analyze the data. To check the homogeneity of the sample, the Bartlett test was used. To compare continuous variables between groups, either the Student t test or Mann-Whitney test was used. Changes over the 3 periods (PRE, PO-1, and PO-7) within each group were examined by analysis of variance (ANOVA) with repeated measures, followed by post-test of Bonferroni. The difference in evolution over time between the 2 groups was examined by ANOVA with repeated measures on one factor (group).
The 6MWD variation between PRE and PO-7 was evaluated by the Wilcoxon signed-rank test, while the relative variation for the 6MWD between the 2 groups was performed by the Mann-Whitney test. The statistical significance level was set at P < .05.
Results
Eight of the 38 recruited patients were excluded from the study: 5 for requiring mechanical ventilation; 3 for pneumonia. All patients tolerated CPAP application well. Thus, the final sample consisted of 30 patients. The mean ages in the control and experimental group were 56.8 ± 10.2 years and 55.1 ± 12.3 years, respectively. The numbers of men in the control and experimental groups were 10 (66.7%) and 11 (73.3%), respectively. In the experimental group, the indications for the pneumonectomies were as follows: 12 pulmonary neoplasia, 2 tuberculosis residual lesions, and 1 mycetoma. In the control group, the indications for the pneumonectomies were: 11 pulmonary neoplasia, 2 mycetoma, 1 bronchiectasis, and 1 pulmonary sequestration.
The surgeries performed in the experimental group were: 4 segmentectomies, 7 lobectomies, 2 bilobectomies, and 2 pneumonectomies. The surgeries performed in the control group were: 2 segmentectomies, 9 lobectomies, 1 bilobectomy, and 3 pneumonectomies. Postoperatively, at no time during the observation was there any hemodynamic change or substantial pain that would prevent the continuation of the treatment in either group. On the seventh postoperative day, no prolonged air leak through the drain was noticed with CPAP or breathing exercises. In the 30 patients, the chest x-rays performed daily showed no pneumonia, atelectasis, or pneumothorax.
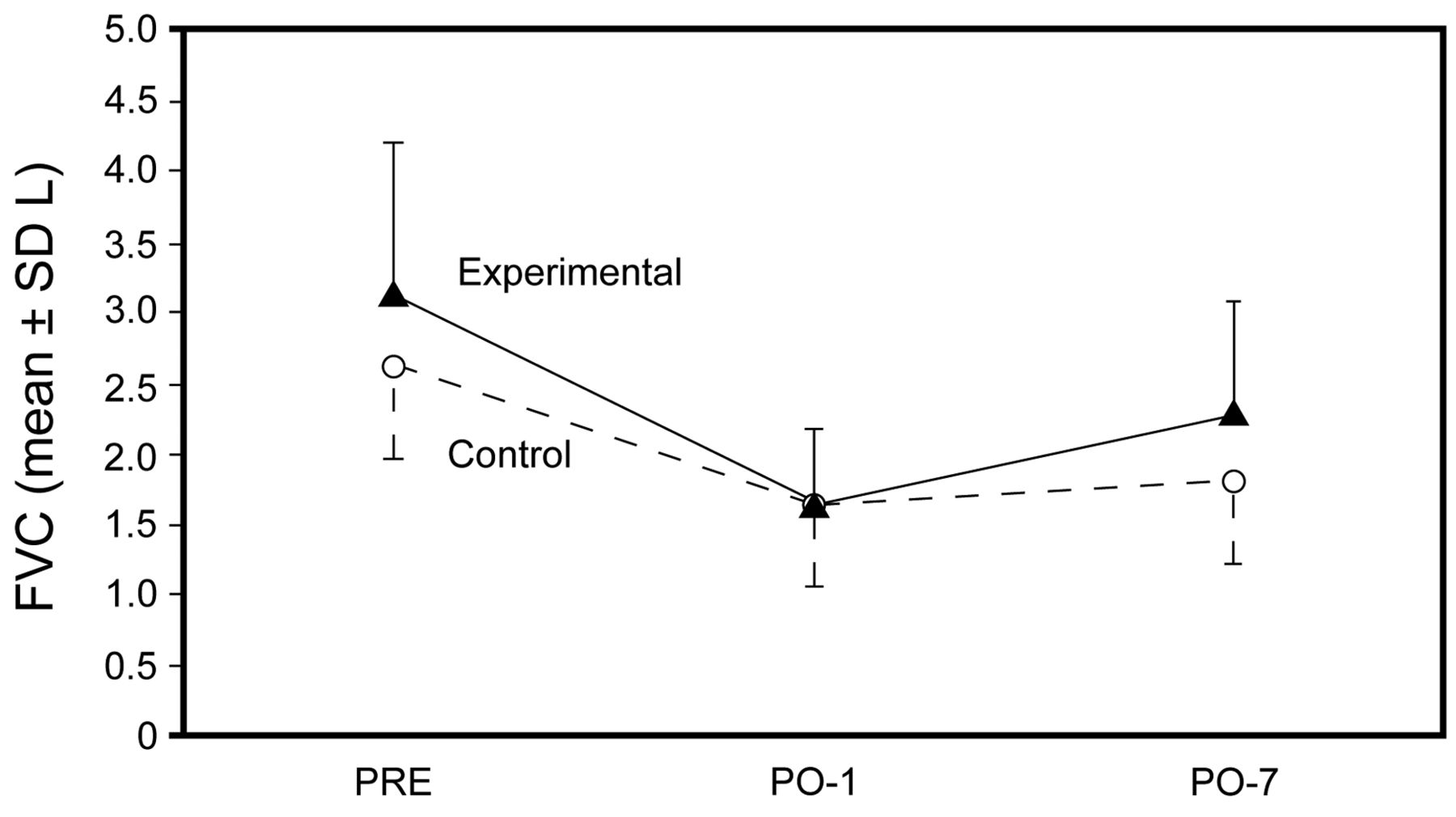
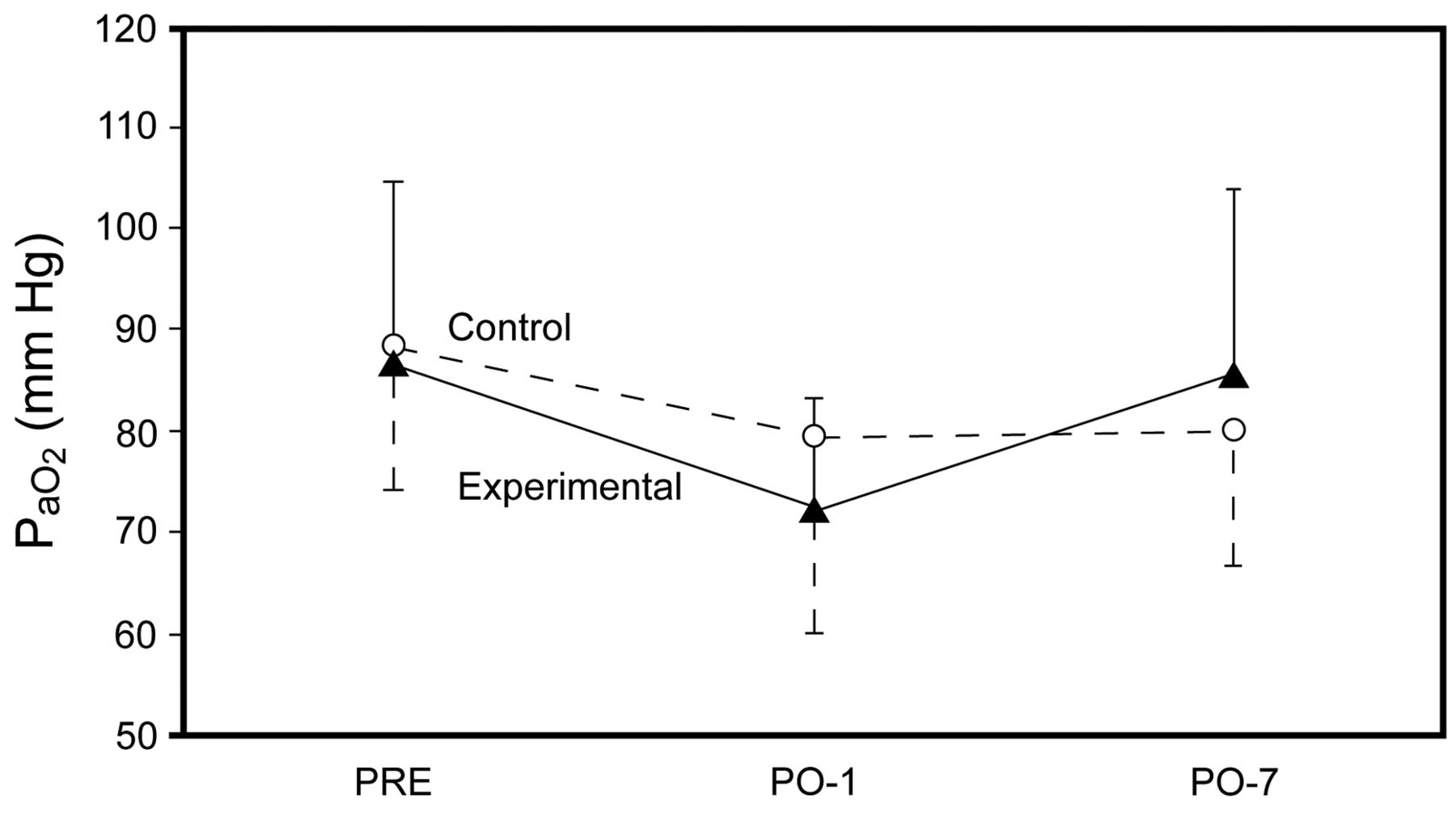
Table 1 shows the patients' respiratory function and 6MWT data for control and experimental groups, obtained preoperatively, on the first postoperative day and the seventh day after surgery, and the comparison between the 2 groups. No statistical differences in respiratory function and 6MWT data were noted between control and experimental groups in the preoperative evaluation (P > .05). The forced vital capacity (FVC) and PaO2 increased significantly between PO-1 and PO-7 only in the experimental group (Fig. 1 and 2).
Respiratory Function and 6-Minute-Walk Test Data for Control and Experimental Groups, Obtained Preoperatively, on the First Postoperative Day and the Seventh Day After Surgery, and the Comparison Between the 2 Groups
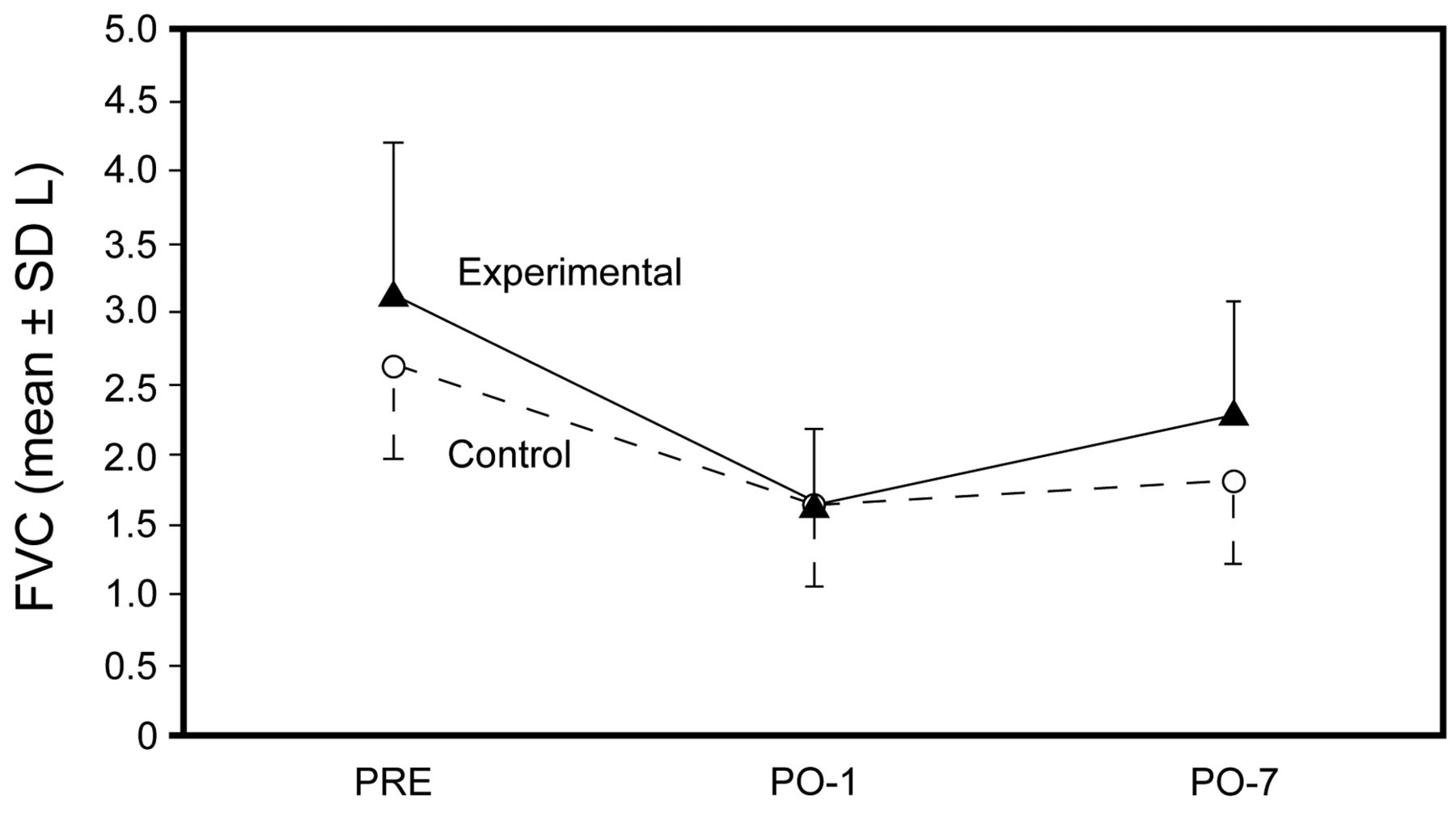
Changes in forced vital capacity (FVC) for control and experimental groups, obtained preoperatively (PRE), on the first postoperative day (PO-1), and the seventh day after surgery (PO-7).

Changes in PaO2 for control and experimental groups, obtained preoperatively (PRE), on the first postoperative day (PO-1), and the seventh day after surgery (PO-7).
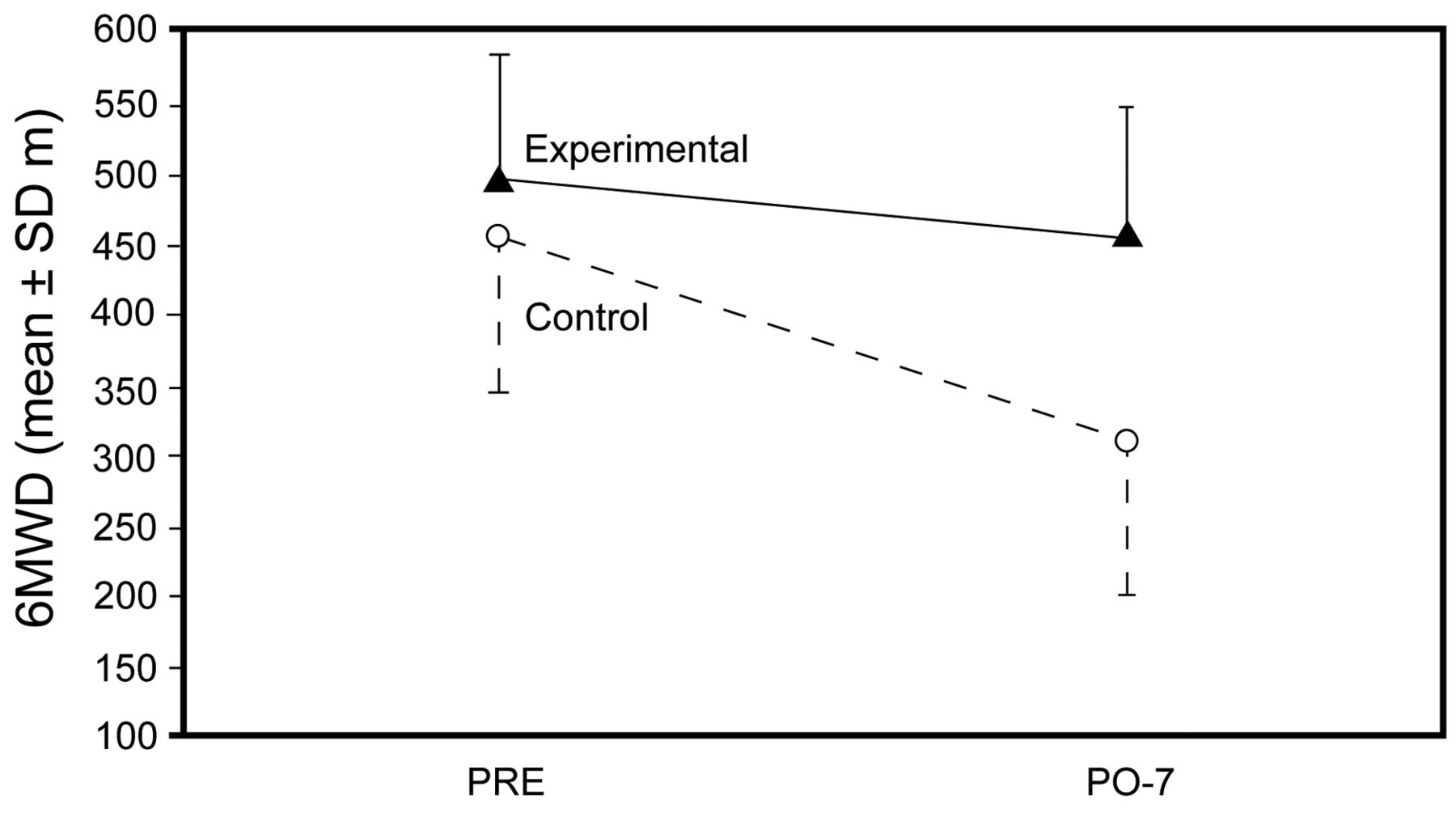
Comparison between the 2 groups revealed a significant difference only in the 6MWD (P < .001), where the average decrease between PRE and PO-7 in the experimental group (497.6 ± 90.7 m, 95% CI 451.7–543.5 m to 456.9 ± 93.5 m, 95% CI 409.6–504.3 m) was lower than in the control group (457.8 ± 111.1 m, 95% CI 401.6–514.1 m to 310.6 ± 107.1 m, 95% CI 256.4–364.8 m) (see Table 1 and Fig. 3). Statistical significance was found between control and intervention groups at PO-7 (P < .002), but no significant differences were obtained at PRE (P > .31). The 95% CI for the difference between control and intervention group at PO-7 was 74.5–218.3 m.

Changes in 6-min walk distance (6MWD) for control and experimental groups, obtained preoperatively (PRE) and the seventh day after surgery (PO-7).
Discussion
The main findings of the present investigation were that, when started early, CPAP improves the 6MWD performance on the seventh day after lung resection surgery, and that CPAP does not cause prolonged air leak through the chest drain. To our knowledge, no other investigation has evidenced CPAP's early effect on 6MWT in patients submitted to lung resection.
CPAP application has the potential to enhance the benefits of pulmonary rehabilitation.17–19 Despite some clinical benefits, the underlying mechanisms induced by CPAP are not fully understood. The reduction of the load against which the respiratory muscle pump must work seems to restore the central chemosensitivity and the central drive to breathe.20 Additionally, CPAP can reduce the inspiratory swings in esophageal and transdiaphragmatic pressure, as well as the paradoxical motion and expiratory recruitment of the abdominal muscles.21 This is accounted for by a reduction in auto-PEEP and in the elastic work performed.
The efficiency of the cardiopulmonary system may be different during increased metabolic demand than at rest. In contrast to other exercise tests, the 6MWT evaluates functional capacity at sub-maximal levels, and is therefore considered the test that best represents the ability of patients to perform activities of daily living. It has proved to be reliable, inexpensive, safe, and easy to apply.22 The 6MWT has also been used to measure outcomes before and after therapeutic interventions.23 The distance covered in the 6MWT predicts morbidity and mortality from cardiopulmonary diseases.24–26
In our research, the results found in 6MWT are highly important. The 6MWT is used in order to evaluate the response of an individual to exercise, providing a global analysis of the respiratory, cardiac, and metabolic systems.21 Since 6MWD is one of the survival and life quality parameters for patients in the postoperative period,27 the quick recovery of the values of this test in our study shows the importance of early CPAP application in patients who underwent pulmonary resection.
Prolonged air leak is the most feared complication when positive pressure is used. It is reported to cause increased stay and higher hospital costs.16 In our study, the early application of CPAP was safe, and there was no report of prolonged air leak. This fact may reduce the concern of health professionals in recommending the early application of CPAP in the lung resection postoperative period.
Perrin et al28 suggest that noninvasive ventilation with pressure support is more effective than the application of CPAP, as the outcomes obtained by CPAP deteriorate soon after the withdrawal of the interface application. In our study, such deterioration was not observed, and the application of CPAP caused effects similar to those achieved by these authors. It is noteworthy that patients were followed up only in the first 7 postoperative days. Therefore, it was not possible to evaluate the effect of CPAP on hospital stay.
In our study, the mean reduction in FVC was 0.83 L in the control group and 0.85 L in the experimental group at the end of the seventh postoperative day, when compared with preoperative values. Much of this reduction has been previously attributed to the pain and thoracic wall restriction after thoracotomy, rather than to the direct effect of lung parenchyma loss.29 However, we observed that only in the experimental group was there a significant gain in FVC between PO-1 and PO-7 (P < .001). A possible explanation for this FVC increase after noninvasive CPAP is the efficacy of this treatment to increase lung expansion.30
The noninvasive application of CPAP therapy has been described as an effective method for improving postoperative pulmonary dysfunction and pulmonary oxygen transfer.7 In fact, in patients who received CPAP, we found a significant increase in the PaO2 on the seventh postoperative day, when compared with that seen during the first postoperative day. This result was also observed by Perrin et al,28 who used noninvasive ventilation, with pressure support in the first 72 postoperative hours through a microprocessor device for the treatment of patients submitted to lobectomy or pneumonectomy. Severe atelectasis reduces functional residual capacity and may cause hypoxemia. Therefore, arterial oxygenation improvement may be explained by the recruitment of areas of alveolar collapse in the lungs with the application of CPAP.9 Interestingly, in our study, no arterial oxygenation improvement was observed in patients who received breathing exercises.
Caution should be exercised in attempting to generalize the findings of the present study, since the study protocol presents certain limitations in its design. As this was a sequential allocation rather than a randomized study, investigators had prior knowledge of the allocation group. However, allocation was not broken, and the physician who carried out the patient allocation did not know the type of surgical procedure that was subsequently performed. Moreover, demographic, respiratory function, and functional capacity data for experimental and control groups showed no significant differences. Since it was not possible to randomize the order of the evaluation, it is likely that the effect of learning the 6MWT helped to change the performance on the seventh postoperative day. However, we believe that in our study the fact that the patients were familiarized with the 6MWT in the preoperative period minimized this possible influence. It is worth emphasizing that there are some differences, albeit not statistically significant, between some baseline physiology parameters (eg, PEF lower in the control group than in the experimental group) that potentially could explain some of the differences noted in the 6MWD.
Conclusions
In conclusion, in the present study, both therapies were proven to be beneficial; however, CPAP therapy was more efficient than breathing exercises, especially with regard to 6MWD. Moreover, there was no case of prolonged air leak through the chest drain, corroborating the efficacy and safety of CPAP.
Footnotes
- Correspondence: Agnaldo J Lopes MD PhD, Laboratory of Respiratory Physiology, State University of Rio de Janeiro, Rua Araguaia 1266 Bloco 1/405, Freguesia, Jacarepaguá, Rio de Janeiro, Brazil 22745–271. E-mail: phel.lop{at}uol.com.br.
This research was partly supported by the Rio de Janeiro State Research Supporting Foundation.
The authors have disclosed no conflicts of interest.
See the Related Editorial on Page 474
- Copyright © 2012 by Daedalus Enterprises Inc.









{kind=link}
{kind=link}
{kind=link}