

Abstract
BACKGROUND: Respiratory therapist (RT) is a nascent career in China, so little information is available about intensive care unit (ICU) respiratory care resources and practices, requirements for RTs, and barriers to recruit RTs.
METHODS: Using survey methodology, we designed and mailed a questionnaire to ICU supervisors and staffs at all 106 ICUs within 46 tertiary and university-affiliated hospitals in Beijing.
RESULTS: We obtained responses from 72 of 106 ICUs. There were 644 ICU beds, 18 RTs, 464 physicians, and 1,362 nurses in these 72 ICUs. The ratios of invasive and noninvasive ventilators to beds were 0.7/1 and 0.31/1. Nineteen ICUs were not equipped with noninvasive ventilators; 18 had started using noninvasive ventilation only within the last 5 years; 9 had only nasal cannulas for conventional oxygen therapy. Of 194 responders, 57.8% implemented spontaneous breathing trial before extubation; 23.7% never monitored airway temperature while using heated humidifier; 56.7% changed circuits once a week; and 20.6% every 1–3 days. The survey indicated that 91.2% had heard of the profession of RT before, mostly by attending academic conferences; 86.1% believed respiratory care should be provided by RTs. Due to the paucity of trained RTs, only 9.7% (7/72) ICUs had actually recruited RTs. The specific tasks supposed to be assigned to RTs were mechanical ventilation, chest physiotherapy, and airway care.
CONCLUSIONS: ICU respiratory care equipment and the knowledge to use them are insufficient. Important differences exist in respiratory care practice, which is mostly provided by nurses and physicians. RTs have been gradually recognized and accepted by ICU staff, while professional training and education are needed.
Introduction
With the continuing development of critical care medicine in China, increasing demand has been placed on respiratory therapists (RTs). The intensive care unit (ICU) is a complex environment in which multidisciplinary expertise has been shown to enhance clinical outcomes. It is widely recognized throughout the United States that RTs contribute importantly to ICU outcomes.1–3 Services provided by RTs can decrease ventilator days, utilization of ICU resources,2–9 medical care, and costs,5–7 as well as ICU and hospital stay.8,9 Also, for non-ICU surgery patients, total hospital costs are decreased by RT-evaluate-and-treat protocols.10
However, there were no trained RTs in mainland China until 2004, when the first group of trained RTs graduated from West China Medical Center of Sichuan University, the only medical university providing respiratory care education in China.11 To date, there have been fewer than 100 graduates. Due to a lack of professional RTs in the majority of ICUs, respiratory care services have been primarily provided by nurses and doctors, as shown in our previous questionnaire survey, in which 491 ICU staff from 320 ICUs participated.12
To know more details about current ICU respiratory care resources and practices, requirements for RTs, and the barriers to recruit RTs, we performed a survey in the ICUs of tertiary or university-affiliated hospitals in Beijing, where ICUs were first instituted in China,11 and acquired information about current practice and requirement.
QUICK LOOK
Current knowledge
Respiratory care practices in China are predominantly performed by physicians and nurses. Healthcare systems within China are rapidly developing and changing to meet demands.
What this paper contributes to our knowledge
The role of the respiratory therapist is being defined and expanded, with greater acceptance of respiratory therapists as a distinct profession. Mechanical ventilation, airway clearance, and airway care are the most common procedures assigned to respiratory therapists.
Methods
Survey Design
The study was approved by the institutional review board of Beijing Chaoyang Hospital. To develop the survey instrument, we relied on the background information obtained from an extensive literature review, our prior survey,12 and informal interviews with experts in the respiratory care and ICU fields. A survey methodology was employed, including item generation and reduction, pretesting, clinical sensibility, and test-retest reliability, to develop a questionnaire. The 106 ICU supervisors (directors/associate directors/nursing heads) of all 46 acute care tertiary or teaching hospitals in Beijing were identified through Internet information or through hospital telephone directories. Three questionnaires and a personalized cover letter were sent via surface mail to each ICU supervisor, who was asked to fill out one questionnaire and distribute the other 2 to his or her staff. Reminders were issued via telephone and e-mail to non-responders. The survey took place between October 2006 and January 2007.
Survey Items
The self-administered, anonymous, descriptive survey inquired about 57 items, in 7 specific areas: demographic characteristics (respondent's job titles, hospital's level of care, and ICU size [eg, beds, doctors, nurses]); ICU respiratory care equipment (ventilators, oxygen therapy and aerosol therapy devices); noninvasive ventilation (NIV) information, including usage, type of NIV ventilator, and initial mask for NIV; respiratory care providers; actual practice of daily clinical work (spontaneous breathing trial [SBT], airway care, and ventilator management); ICU staff's recognition of the RT; and the requirements for the RT profession. The ICU supervisors were questioned regarding their satisfaction with the quality of respiratory care practice, including 12 different common scenarios in Chinese ICUs: ventilator settings, monitoring, weaning, extubation, ventilator check, circuits changing, suctioning, humidification, aerosol therapy, chest physiotherapy, oxygen therapy, and transportation of mechanically ventilated patients, by using a 1–10 point scale (in which 1 was “very dissatisfied” and 10 was “very satisfied”). A rating score higher than 6 was considered to be “satisfied.”
Statistical Analysis
Population-weighted descriptive statistics were calculated (means, standard deviations, tabulations, and proportions) for all questions on the survey. Multivariate statistical analyses were used to explore relationships between questions, and to compare responses to key questions among the principal subgroups of respondents (based on position and setting). Differences were considered significant if P < .05. Data analysis was established by Epidata software (http://www.epidata.dk/index.htm) and analyzed by SPSS software (SPSS 15.0 for Windows, SPSS, Chicago, Illinois).
Results
We sent 288 questionnaires to all the ICUs in the 14 tertiary and 32 teaching hospitals in Beijing, and received 194 (response rate 67.4%, 194/288) effective questionnaires (defined as answers to questions ≥ 90%). We excluded 12 questionnaires in which more than 10% of the questions had not been answered. The 194 responders included 134 physicians and 60 nurses from 72 ICUs from 13 tertiary hospitals and 31 teaching hospitals (response rate 67.9%, 72/106). Seventy-two ICU supervisors participated, including 65 (90.3%) ICU directors/associate directors and 7 (9.7%) nurse managers. Not all questions were completely answered by all responders, so the number of replies varied by question.
ICU Manpower and Respiratory Care Equipment
The survey provided information about the ICU, including the number of beds, doctors, nurses, and ventilators. The physician/bed and nurse/bed ratios were similar among all of the ICUs (Table 1). Only 18 RTs worked at 7 ICUs in 6 hospitals, and the RT/bed ratio was 1:35.8. The ratio of invasive ventilators to beds was higher in the surgical ICUs and respiratory ICUs than in the other ICUs (0.85 vs 0.70, P < .01), while the ratio of noninvasive ventilators to beds was higher in the respiratory ICU than the other ICUs (0.80 vs 0.31, P < .01), in which 19 ICUs were not equipped with noninvasive ventilators. In the remaining 53 ICUs, 4 ICUs' ratio of noninvasive ventilators to beds was less than 0.1, and 22 ICUs' ratio was 0.1–0.3. The survey found that 42.9% started using NIV less than 5 years ago, 35.7% used critical care ventilators for NIV, and 84.6% reported that they initially used face masks. Moreover, nasal cannulas were the only type of conventional oxygen therapy devices in 13.6% (9/66) of the ICUs, while 56.1% (37/66) had an additional item (either a simple or Venturi or reservoir mask) (Table 2).
ICU Manpower and Ventilators
Kinds and Types of Oxygen Therapy Devices
Physicians and nurses shared the work of respiratory care in most of ICUs. As shown in Figure 1, physicians carried the responsibility of managing ventilators, such as setting modes and adjusting parameters (94.4%), weaning (91.7%), and extubation (91.7%). Nurses typically took charge of airway care, including suctioning (95.8%), humidification (94.4%), aerosol therapy (93.1%), chest physiotherapy (90.3%), and circuit changing (87.5%). In the 7 ICUs with RTs, RTs took different responsibilities for their daily work in different ICUs, but they were all independently in charge of ventilator management, including ventilator checks and circuit changing.
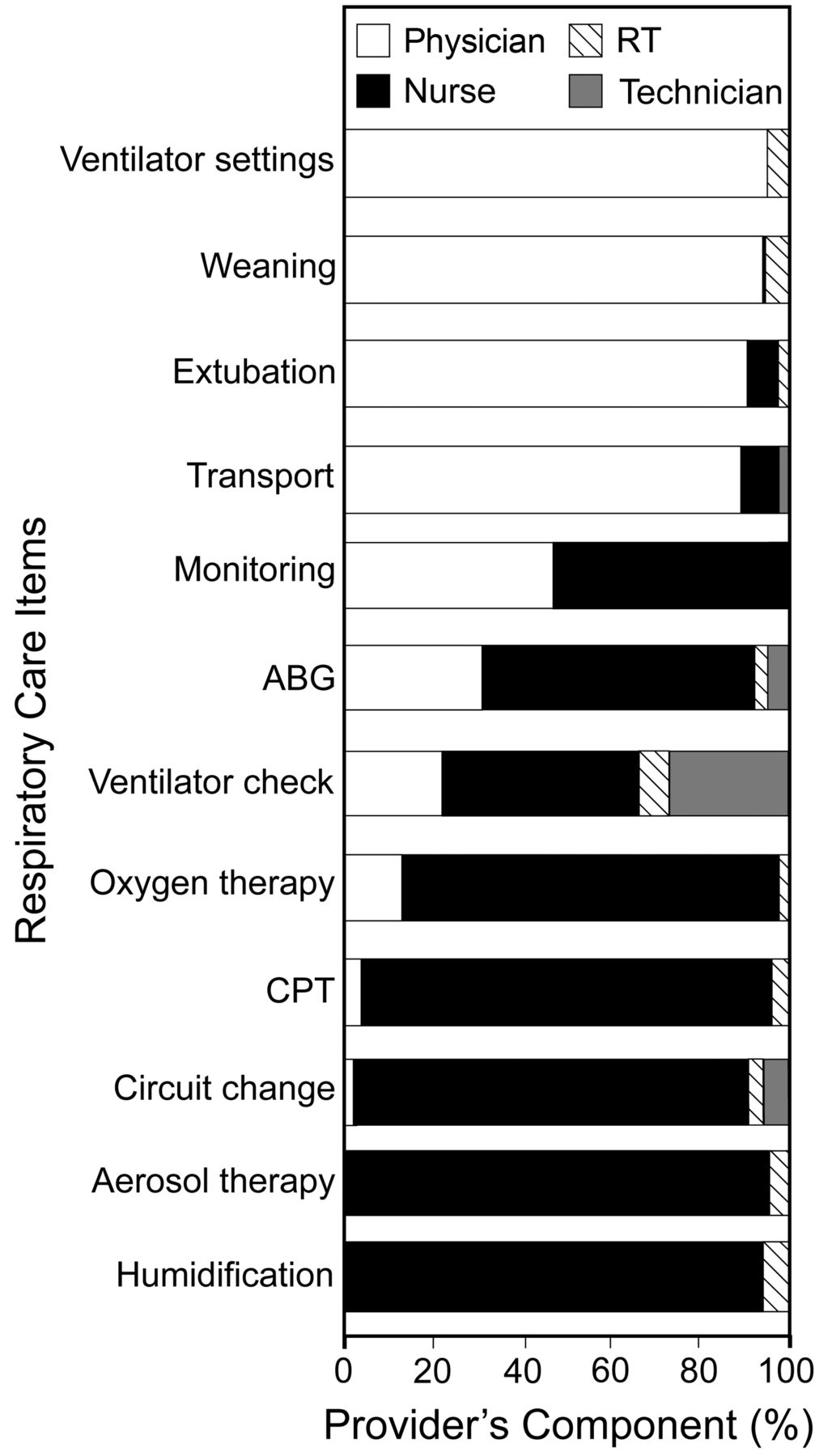
Respiratory care providers. RT = respiratory therapist. ABG = arterial blood gas analysis. CPT = chest physical therapy.
Daily Clinical Practices of Respiratory Care
Of 194 responders, 57.8% implemented SBTs before extubation, while 10.3% were unaware of SBT; 23.7% never monitored airway temperature during invasive mechanical ventilation with heated humidifiers; 26.8% provided humidification by instilling or pumping saline continuously for those patients who were weaned from ventilators but not extubated; and 63.9% checked ventilators before use. Ventilator circuits were changed once a week (56.7%), every 1–3 days (20.6%), and every 3–5 days (10.8%) (Table 3).
Clinical Daily Respiratory Care Practices
ICU Supervisors' Satisfaction With Respiratory Care
The top 3 items with which supervisors reported being satisfied were ventilator settings (79% supervisors reported satisfaction), extubation (76%), and weaning (74%), while chest physiotherapy and ventilator checks gained the minimum satisfaction: only 52% and 58% of supervisors reported satisfaction. In the 7 ICUs with RTs, supervisors were all satisfied with ventilator checks and circuit changing.
Recognition of and Requirements for Respiratory Therapists
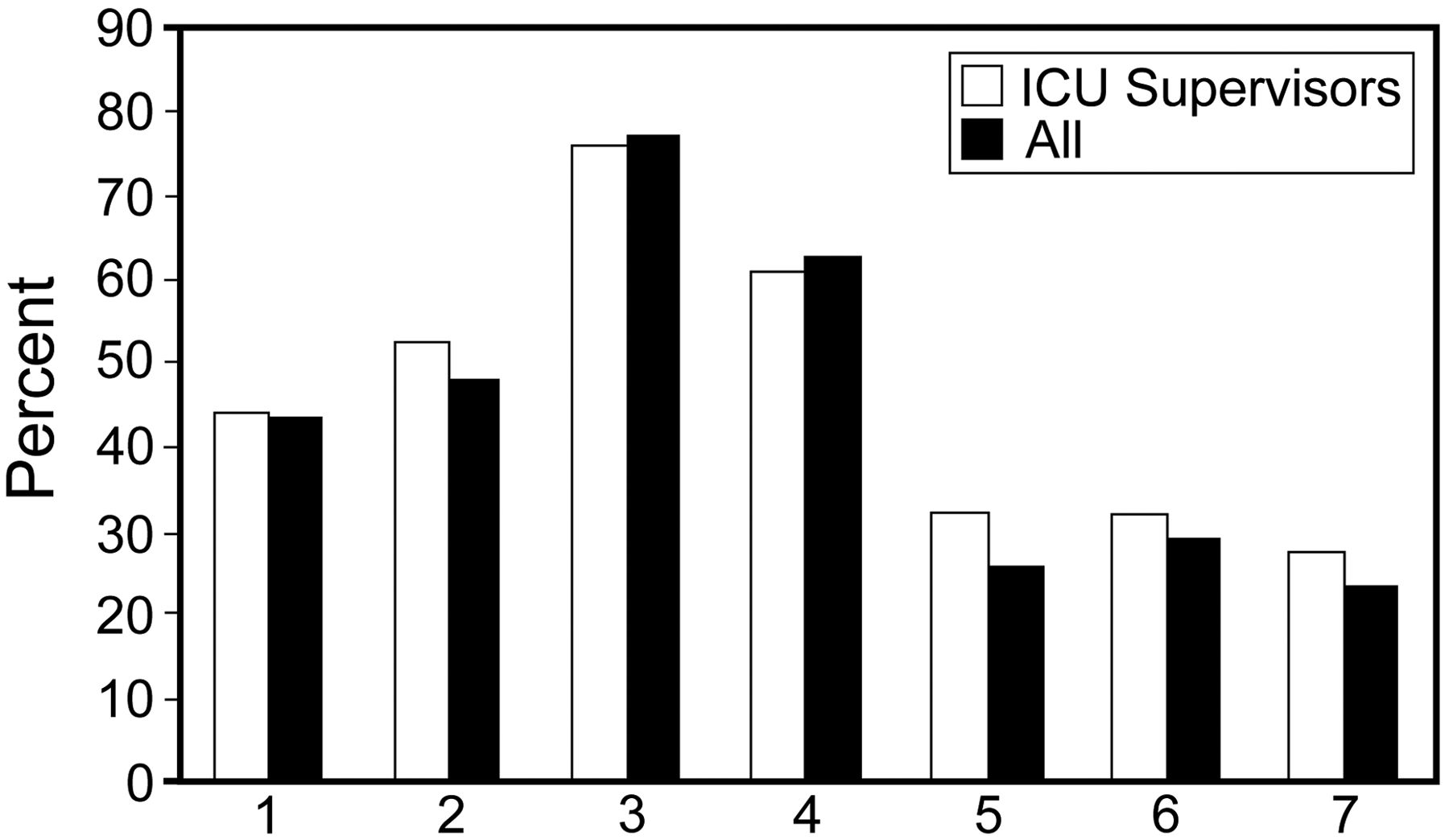
Of 194 responders, 177 (91.2%) had heard of RTs before, primarily while attending conferences for the first time (34%), and 167 (86.1%) believed that respiratory care services should be provided by professional RTs. Sixty-six of the ICU supervisors agreed with this statement and 7 of them had already recruited RTs. The main barrier to recruiting RTs was the paucity of professional RTs with formal training. Other barriers are illustrated in Figure 2.

Barriers to recruiting respiratory therapists (RTs) for those intensive care units (ICUs) who need RTs. 1. Didn't know respiratory care well, hard to arrange their work. 2. Difficulty in coordinating with current ICU staffs. 3. Lack professional RTs who had gained systematic training. 4. Lack job titles. 5. The quantity of patients was not enough. 6. RTs could not produce economic benefit directly. 7. Influenced other staffs' income.
To further assess the specific tasks needing an RT, we included a series of questions to elicit more detailed responses. In terms of performing specific tasks, based on the population-weighted responses, more than 70% of survey participants reported that RTs were cost-effective for providing higher skill services involving mechanical ventilation. Fewer survey participants reported that RTs were cost-effective for several simple operations such as oxygen therapy. However, for those who had worked with RTs before, all considered mechanical ventilation, airway care, and chest physiotherapy of the same importance (Table 4).
Percentage of Different Survey Participants Who Consider Respiratory Therapists Cost Effective for Specific Tasks
Discussion
Beijing ICUs are considered among the best in China, especially those ICUs in tertiary and teaching hospitals. We have gained remarkably good responses from nearly all of the 46 tertiary and teaching hospitals. Thus we consider that our findings are faithful indicators of ICU practices in Beijing, which is deemed to have more access to resources than most other areas of China. For example, ICU nurse-to-bed ratio in our survey (2.12, 1,362/644) is higher than the national average, which ranged from 1.37 to 2.02.11 However, it was still lower than the standard in most developed countries.13–15 There were only 18 RTs who took part in our survey; the ratio of RTs to ICU beds (1 to 35.8) was also much lower than that preferred in the United States.13
Compared with our previous questionnaire survey, in which 491 ICU staffs from 320 ICUs in 30 provinces participated, the ventilator-to-bed ratio in this survey was higher and the noninvasive-ventilator-to-bed ratio was double the ratio in the previous survey.12 However, nearly half of ICUs started using NIV less than 5 years ago, and there was not yet enough experience with NIV. Nineteen ICUs were still not equipped with any noninvasive ventilators. In contrast, only 1 in 71 hospitals was not equipped with NIV ventilators in the United States, according to a regional survey,16 and NIV was reported to be available at any time by nearly all respondents (97%) from half (63/128) of the United States Veterans Affairs ICUs.17 Oxygen therapy also proved to be an area where there was a lack of proper equipment. In 9 ICUs with only nasal cannulas for conventional oxygen therapy, it could be speculated that acute hypoxemic patients were usually intubated if hypoxemia could not be corrected by adjusting oxygen flow with nasal cannulas. Compared with nasal cannulas, high flow oxygen devices were found to decrease mortality and comorbidities in patients who experienced a severe acute ischemic stroke.18 High oxygen concentrations have also been shown to significantly reduce the risk of wound infection.19 In all, the lack of a spectrum of respiratory care equipment and adequate knowledge is a serious problem.
Our survey confirmed the conclusion from the previous survey: physicians and nurses share responsibility for respiratory care in ICUs.12 However, respiratory care practices varied. Take weaning as an example; in many guidelines, SBTs have been recommended as a routine tool for evaluating a patient's readiness for weaning,20,21 but it was not routine in nearly half of Beijing ICUs, and some staffs did not know what an SBT was or how to perform one. Airway temperature should be monitored when using heated humidifiers in order to avoid burning or delivering a gas that has not been properly warmed, but one fourth of responders reported that they never monitored it; using heated humidifiers without monitoring might be dangerous in those ICUs. For patients who were weaned from invasive ventilation but could not be extubated, continuously pumping or instilling saline directly into patient's airway was a popular practice. We could not find the same technique being used for humidification in any papers published in English. Similarly, we found that saline instillation was used before endotracheal suctioning when indicated.22 A recent study suggested that normal saline instillation prior to suctioning decreased the incidence of microbiologically proven ventilator-associated pneumonia in ventilated patients.23 However, on a review of the literature on instilling saline, the American Association for Respiratory Care formulated a guideline that the routine use of normal saline with suctioning might be more harmful than helpful.24 Moreover, it is well known that the instilled saline easily goes to the gravity dependent areas of the lung.25 Therefore, we think that pumping or instilling saline as a method for humidification during weaning procedures should be eliminated.
In the current cost-attentive healthcare climate, the effectiveness of different providers in delivering care is being examined closely. The cost-effectiveness of RTs still needs to be evaluated in many countries. In Australia and New Zealand, where there are no professional RTs, full time nurses have to take responsibility for mechanical ventilation in ICUs, resulting in additional training and more recruitment of nurses. It was reported that the nurse-to-bed ratio was 4.7:1 in Australia and 4.2:1 in New Zealand.14 In comparison, this ratio was lower in the United States,15 where RTs were in charge of respiratory care. Critical care medicine in China is still in an early phase of development. There is no formal accredited critical care training program. As a result, the majority of ICU staffs cannot get enough professional education and training.11 Without enough ICU staffs and professional training, it is hard to provide satisfactory respiratory care.
As reported in our survey, some respiratory care services were provided by physicians and nurses. Their supervisors were well aware of this situation and not satisfied with most of the current services. In contrast, in the 7 ICUs with RTs, the supervisors were all satisfied with ventilator management, which RTs independently took charge of. This means that the RT, as a new member of the Chinese ICU team, has been gradually recognized and accepted by ICU staffs.
Academic conferences are an effective way to exchange information. Most of the staffs were aware of the practice of respiratory care as a separate and distinct profession through academic lectures given by RTs from the United States, Taiwan, and other countries. However, lectures alone cannot provide adequate information about the work content and value of RTs. The staffs already working with RTs understand that RTs provide more encompassing services than just mechanical ventilation. They are hence more willingly to make efforts to recruit RTs and to take full advantage of these professionals.
Professional staffs and training are needed, but there are still no RTs in the majority of Chinese ICUs. Only one Chinese medical university provides bachelor degree education. We suggest that associate degree and on-the-job education of high quality are desirable for expanding the availability of RTs, whose professional value and benefit still need to be proved in more areas. Moreover, the relationship between physicians, nurses, and RTs needs to be considered. These considerations will determine the success of RTs in Chinese medicine. As more RTs begin to work in different hospitals, further studies are needed regarding their work content, employment, professional certifications, and evaluation by their colleagues.
One limitation of our study is that we could not survey all of the ICUs in the tertiary or teaching hospitals. The 72 ICU participants might be aware of RTs or be interested in the profession, so their demands on RTs might be higher than those ICUs that did not respond. For the sensitive question of why there is no RT in a facility, we designed 7 choices and space to add comments. Responders tended to opt out for the multi-choice questions, but the space for comments was occasionally filled. Possibly those choices had properly described their reasons, or their situation was too complicated to be described.
We are aware that this survey was completed 5 years ago. Since then critical care medicine in mainland China has developed, and ICU staffs have gained more professional training. It is likely that the current situation has been improved. Therefore, future studies are warranted to unfold these changes.
Conclusions
The number of ventilators has increased, but other types of respiratory care equipment and the knowledge of how to use it are still deficient. That has led to variable clinical practices in ICU respiratory care, which have been provided mostly by nurses and physicians. This lack has been perceived by ICU staffs, who expressed the need for professional respiratory care training and staffs. RTs have been gradually recognized and accepted as new members in the Chinese ICU team, and more studies are needed to confirm their cost-effectiveness.
Footnotes
- Correspondence: Chen Wang MD, Department of Respiratory Medicine, Capital Medical University, Beijing Key Laboratory of Respiratory and Pulmonary Circulation Disorders, Beijing Institute of Respiratory Medicine; Beijing Hospital, Ministry of Health, PR China, 1 Da Hua Road, Dong Dan, Beijing, 100730, PR China. E-mail: cyhrt{at}sina.cn.
The authors have disclosed no conflicts of interest.
See the Related Editorial on Page 476
- Copyright © 2012 by Daedalus Enterprises Inc.









{kind=link}
{kind=link}