

Abstract
BACKGROUND: The measurement of maximal respiratory pressure (MRP) is a procedure widely used in clinical practice to evaluate respiratory muscle strength through the maximal inspiratory pressure (PImax) and maximal expiratory pressure (PEmax). Its clinical applications include diagnostic procedures and evaluating responses to interventions. However, there is great variability in the equipment and measurement procedures. Understanding the impacts of the characteristics of different interfaces can augment the repeatability of this method and help to establish widely applicable predictive equations. The aim of this study was to evaluate the influence of 4 different interfaces on a subject's capacity to generate MRP and the impact of these interfaces on the repeatability of these measurements.
METHODS: Fifty healthy subjects (mean ± SD age 26.36 ± 4.89 y) with normal spirometry were evaluated. MRP was measured by a digital manometer connected to 4 interfaces using different combinations of mouthpieces and tubes. The following variables were analyzed: maximum mean pressure, peak pressure, plateau pressure, and plateau variation. Analysis of variance for repeated measures or a Friedman test was used to compare the 4 interfaces, with P < .008 after Bonferroni adjustment considered significant.
RESULTS: There was no significant difference between the 4 interfaces with respect to maximum mean pressure, peak pressure, plateau pressure, or plateau variation for PImax (P ≥ .49) or PEmax (P ≥ .11), nor did the number of tests performed to fulfill the criteria of repeatability for PImax (P = .69) or PEmax (P = .47) differ among the 4 interfaces.
CONCLUSIONS: PImax and PEmax values seem not to be influenced by the different interfaces studied, suggesting that patient comfort and availability of interfaces can be considered.
Introduction
Measuring maximal respiratory pressure (MRP) is a method of investigating the strength of respiratory muscles, involving specifically the measurement of both maximal inspiratory pressure (PImax) and maximal expiratory pressure (PEmax). PImax and PEmax are simple, static, volitional, and effort-dependent tests defined as the respiratory pressure an individual is able to generate from the mouth. The pressure measured during these tests reflects the synergistic action of inspiratory or expiratory muscles.1–3
The applicability of MRP tests in the clinical practice of physical therapists and physicians is wide, involving several diagnostic procedures and assessing responses to interventions.4–10 PImax is more sensitive to certain clinical disorders, such as situations of muscle weakness,1 whereas PEmax reflects an important parameter of the ability to cough and expectorate, which are very important for patients with neuromuscular diseases.11 These tests were also widely used in research protocols.4,7,9
Currently there is great variability in the equipment and procedures used to measure MRP. One possible source of observed differences may be this lack of standardization.1–3,12–17 These variations involve the mouthpiece, the tube used to connect the mouthpiece to the manometer, the air leak orifice, the lung volume at which the maneuver is performed, the posture of the individual during the test, the use of a nose clip, the definition of maximum pressure, the duration of the test, the resting time between tests, and the type of manometer (analog or digital).12,15,17–19
Recently, in a review of studies assessing MRP in adults, Evans and Whitelaw17 noted factors that can influence the measurements, including the interface. However, there is still no formal recommendation regarding the different factors that can influence MRP tests. Consensus exists only on the presence of the air leak orifice (which is 1–2 mm in diameter1,20) and the maximum of 5 efforts to achieve repeatability in each PImax and PEmax test.2,3 Of these 5 efforts, at least 3 should be acceptable and, among these, at least 2 should be reproducible.3
Taking into account the relative lack of standardization of equipment and procedures for measuring MRP, many researchers have recommended that they be standardized.1–3,15–17 Understanding the influence of different interfaces on the repeatability of the MRP measures can help practitioners and researchers to select the more adequate interface to be used when measuring respiratory muscle strength.
In this context, the main objective of this study was to evaluate the influence of 4 different interfaces that vary with respect to their mouthpieces and tubes on a subject's capacity to generate PImax and PEmax. Secondarily, the impact of these interfaces on the acceptability and repeatability of the measurements was evaluated.
QUICK LOOK
Current knowledge
The measurement of maximal respiratory pressure is a procedure widely used in clinical practice to evaluate respiratory muscle strength. However, there is great variability in the equipment and measurement procedures.
What this paper contributes to our knowledge
With use of a digital manometer, changing the interface had little effect on the accuracy or reproducibility of the measurement. The best interface for monitoring maximal respiratory pressure may be the interface that provides the greatest patient comfort and acceptance.
Methods
This study was performed at the Laboratory of Assessment and Research in Cardiorespiratory Performance, Physiotherapy Department, Universidade Federal de Minas Gerais, Belo Horizonte, Minas Gerais, Brazil.
Sample
A convenience sample was recruited from the institution's community. The sample size calculation was based on a pilot study with the first 10 subjects who reached the criteria for acceptability and repeatability for MRP tests.3 The maximum mean pressure variable was considered for both PImax and PEmax. For a significance level of .05 (α = .05) and a statistical power of 0.80 (β = 0.20), a sample size of 45 subjects was indicated.21 Taking into account subject drop-out, a total of 50 subjects were included.
The inclusion criteria were: age between 20 and 50 years22; body mass index (BMI)23 between 18.5 and 29.9 kg/m2; no history of or current smoking; no occupational exposure to a risk environment2,24; no evident chest deformities3; no reported neuromuscular, respiratory or heart disease16; no fever in the last 3 weeks prior to the test; no cold or influenza in the week before the test16; no use of drugs such as oral corticoids, central nervous system depressants, barbiturates, or muscle-relaxing drugs16; and spirometric parameters within the normal range.24
The exclusion criteria were: inability to understand or perform the procedures of the research protocol; blood pressure at rest ≥ 180/110 mm Hg; SpO2 < 90%; heart rate > 85% of maximum predicted.25
The study was approved by the ethics committee of the institution (ETIC 556/08), and all subjects gave written informed consent.
Measurement Instruments
A digital manometer, in which PImax and PEmax are measured by pressure transducers,26 was used to measure the MRP with 4 different interfaces. This device was developed in a partnership between the Center for Studies and Research in Biomedical Engineering and the Laboratory of Assessment and Research in Cardiorespiratory Performance, Universidade Federal de Minas Gerais. The interfaces were selected based on guidelines1,3 and a small survey of Brazilian physiotherapists conducted prior to the study.27 The selected interfaces were composed of a tube and a mouthpiece of varying dimensions and materials. Interface A was composed of a corrugated plastic tube 30 × 2 cm and a smooth plastic mouthpiece (Hudson RCI, Temecula, California). Interface B was composed of the same tube but with a flanged silicone mouthpiece (ST3, NS Medical Devices, São Paulo, Brazil). Interface C was composed of a transparent silicone tube 50 × 0.5 cm and a smooth plastic mouthpiece (Globalmed, Porto Alegre, Brazil). Interface D had the same tube, but with a flanged silicone mouthpiece. All mouthpieces included an air leak orifice of 1.8 mm.3,20 Disposable biological filters were used (Vida Tecnologia Biomédica, São Paulo, SP, Brazil). Figure 1 shows in detail the 4 interfaces used in the study. All parts that composed the interfaces are commercially available, and because the flanged mouthpiece could not be directly connected to the tube, a 2 × 5 cm acrylic tube, usually used in noninvasive ventilation circuits, was necessary.

The 4 interfaces assessed in this study. A: Interface with a 30 × 2 cm corrugated plastic tube and a smooth plastic mouthpiece. B: Interface with a 30 × 2 cm corrugated plastic tube and a flanged silicone mouthpiece. C: Interface with a 50 × 0.5 cm transparent silicone tube and a smooth plastic mouthpiece. D: Interface with a 50 × 0.5 cm transparent silicone tube and flanged silicone mouthpiece.
Analyzed Variables
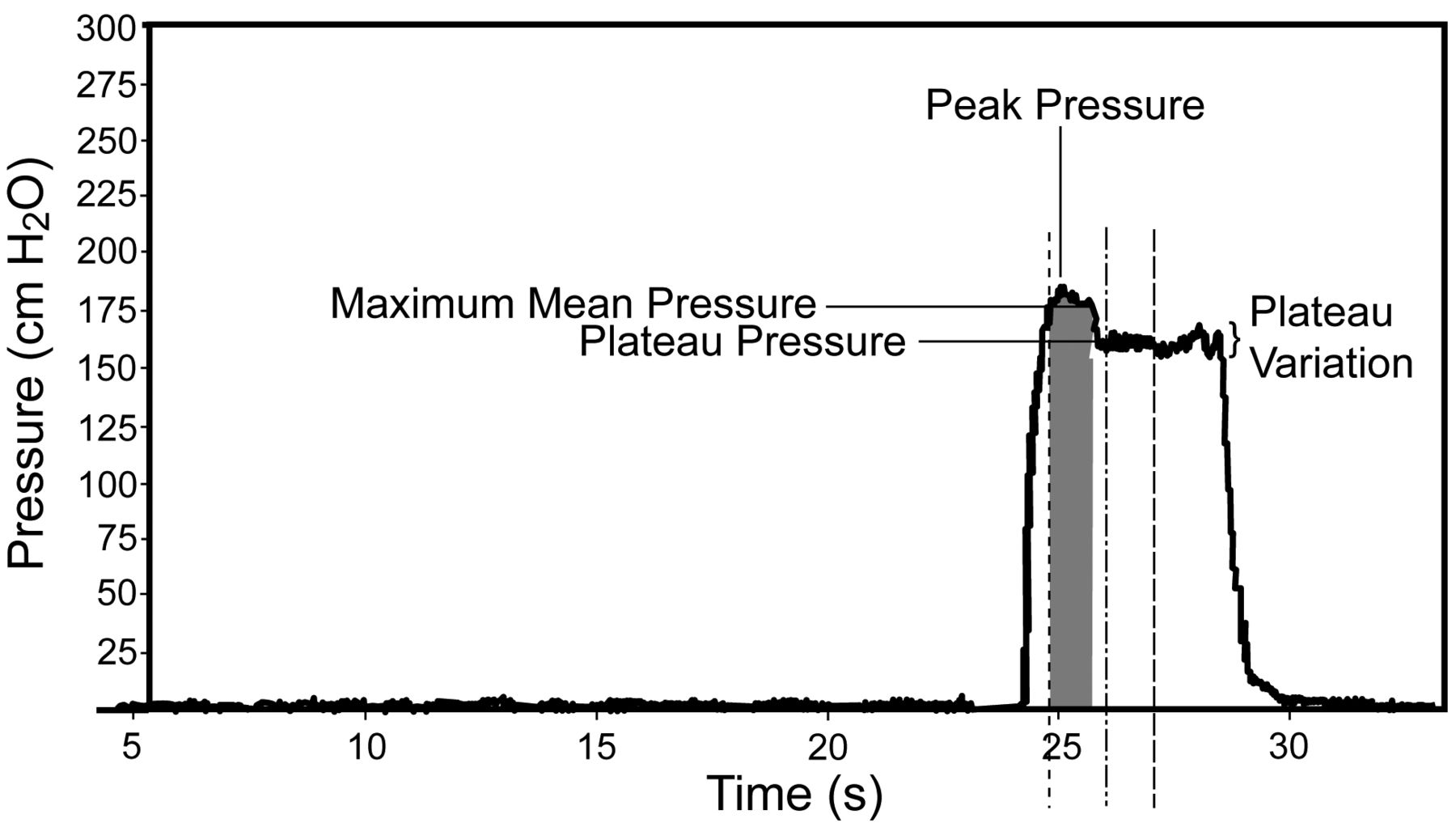
The following variables were analyzed through the graphic interface of the Manovac 3.0 software of the digital manometer: maximum mean pressure, which is calculated first by finding the peak pressure value and subsequently the pressure is calculated around this point and encompasses the highest values included in a one-second period28; peak pressure, which is the highest pressure value obtained during the test28; plateau pressure, which refers to a period of one second19 after the peak pressure in which maximum pressure is maintained with less variability26; and plateau variation, which indicates the variation of the plateau pressure, for which the maximum acceptable rate was 5%. Figure 2 shows a screen display obtained during a test, and the 4 variables analyzed in the study are indicated, as well as the onset and end of plateau pressure variable and the onset of maximum mean pressure variable.

Example of a maximal expiratory pressure screen display using the Manovac 3.0 graphic interface, with variables identified. The maximum mean pressure, peak pressure, plateau pressure, and plateau variation values obtained during each maneuver are displayed separately. The dotted line indicates the maximum mean pressure onset. The dotted-and-dashed line indicates the plateau pressure onset. The dashed line indicates the plateau pressure end.
Procedures
Measurements were taken by the same investigator on 2 separate days. On the first day the subjects underwent an interview about their health and physical activity history, and they filled out the Human Activity Profile questionnaire.29,30 Subsequently, body mass and height, blood pressure, respiratory rate, heart rate and SpO2 were measured. A pulmonary function test was performed in accordance with the Brazilian Thoracic Association guideline,24 using a spirometer (Vitalograph 2120, Vitalograph, Ennis, Ireland) calibrated prior to the test. Subjects with normal spirometry attended the second day of data collection. Subjects were instructed in advance not to perform strenuous physical activity for 12 hours prior to their MRP test performed on the second day.31
On the second day, an electronic randomization of the tests (PImax or PEmax) and of the sequence of interfaces (A, B, C, and D) was performed. The subjects' vital signs (blood pressure, respiratory rate, heart rate, and SpO2) were recorded, they were instructed about the test, and an inducement screen regarding the intensity of effort in the manometer was employed. Following the measurement using the first randomly selected interface and the first maximal pressure, there was a 5-minute rest interval. After that, vital signs (blood pressure, respiratory rate, heart rate, and SpO2) were measured. If the vital signs had not returned to baseline parameters, another 5-minute period was given to the subject.
During all the MRP tests the subjects remained seated, received a standardized specific verbal command, and breathed through the mouthpiece and the tube before performing maximal effort.3 There was an interval of one minute between each test.3,16,32–34 For all tests a nose clip2,16 was worn and subjects were instructed to put the mouthpiece between their teeth and hold it firmly with their lips to prevent air leakage.28
In the PImax tests the subjects were instructed to perform 3 respiratory cycles and then to expire to residual volume, indicating that moment by elevating their right hand. Simultaneously the examiner closed the occlusion orifice, and at this point the subject generated a maximum inspiratory effort and was encouraged to maintain it for 3 seconds.28 In the PEmax tests, the subjects were instructed to perform 3 respiratory cycles and then to inspire to total lung capacity, indicating that moment by elevating their right hand. Simultaneously, the examiner closed the occlusion orifice. At that point the subject generated a maximal expiratory effort and was encouraged to maintain it for 3 seconds.28 During this test the investigator gently held the subject's cheeks to prevent air from accumulating in the lateral region of the mouth cavity.16
The pressure measurement was considered successful when the subject performed at least 3 acceptable tests (ie, no air leakage between the lips or nose clip, and lasting at least one second), and among these, 2 repeatable tests (ie, maximum mean pressure variation less than or equal to 10% and selection of the highest value observed as long as this value was not the last one obtained).2,3,16 The pressure measurement was not considered acceptable in cases where the criteria for acceptability and repeatability were not achieved in a maximum of 8 tests.24,35
The digital manometer was calibrated monthly36 using a digital calibrator (PC507, Hotek Technologies, Tacoma, Washington) (accuracy of 0.025% of full scale) and a duplex pneumatic pump (8111–300, Presys, São Paulo, Brazil) as established by Ferreira et al.26 The expanded uncertainty (kappa = 2) of the manometer was 5 cm H2O.
Statistical Analysis
The data are presented as mean and standard deviation. Spirometric parameters and the variables age, BMI, and Human Activity Profile were used to characterize the sample. When analyzing the variables with respect to the MRP measurements, the data distribution was evaluated using the Shapiro-Wilk normality test. When the data were normally distributed, multi-comparisons were performed by analysis of variance for repeated measures, and the Friedman test was used when the data were not distributed normally. The level of significance was set at P < .008 after Bonferroni adjustment.37,38 The software SPSS 15.0 (SPSS, Chicago, Illinois) was used for the statistical analysis.
Results
Sixty subjects were initially selected, 8 of whom had abnormal pulmonary function tests and were not included in the study. Of the 52 subjects included in the study, 2 were excluded due to inability to perform the procedures, despite care taken with respect to previous instructions and motivation during tests. Thus, 50 subjects were studied (26 women and 24 men) and underwent MRP measurements. Interface A was randomly selected to be first for 9 subjects, B for 17, C for 13 and D for 11.
Table 1 shows the demographic, anthropometric, spirometric, and physical activity level data of the 50 evaluated subjects. Thirty-seven had a BMI within the normal range, 13 were overweight, and all individuals were classified as active.
Demographic, Anthropometric, and Spirometric Data Plus Level of Physical Activity for 50 Subjects
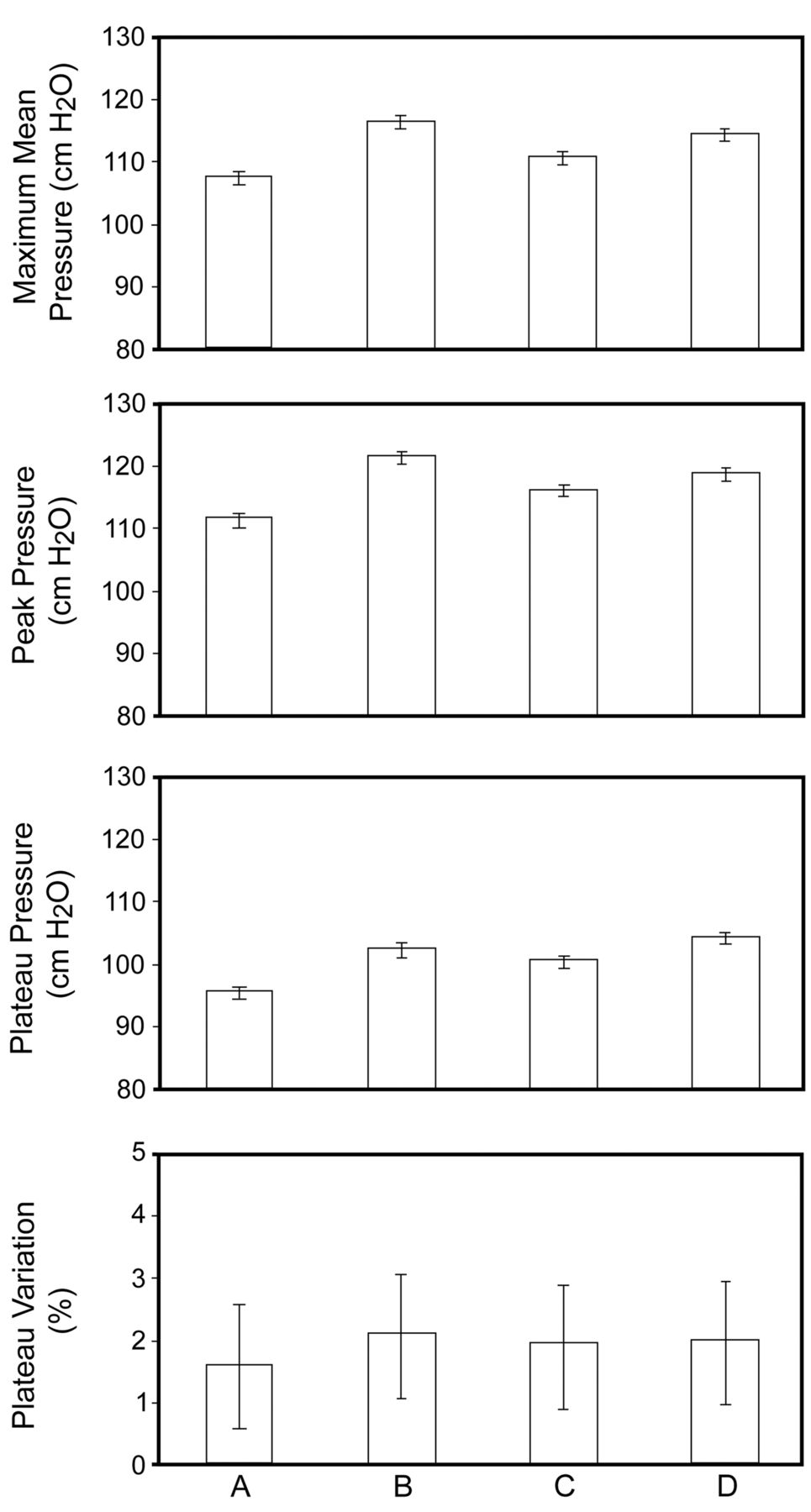
Figure 3 shows the maximum mean pressure, peak pressure, plateau pressure, and plateau variation values for PImax, and Figure 4 shows those for PEmax. When the 4 interfaces were compared, there was no significant difference in any of the variables analyzed for either PImax (P ≥ .49) or PEmax (P ≥ .11).

Comparison of the 4 different interfaces (A, B, C, and D) with respect to variables obtained during maximal inspiratory pressure maneuvers in 50 healthy subjects. Data are shown as mean and standard deviation. None of the differences are significant.
Comparison of the 4 different interfaces (A, B, C, and D) with respect to variables obtained during maximal expiratory pressure maneuvers in 50 healthy subjects. Data are shown as mean and standard deviation. None of the differences are significant.
Table 2 shows the confidence intervals for the primary variable outcome (maximum mean pressure) for both PImax and PEmax. For all interfaces, the actual repeatability between the 2 highest maximum mean pressure values was lower than 5% for PImax and 6% for PEmax.
Mean Difference and 95% Confidence Interval for Maximum Mean Pressure Obtained During PImax and PEmax Tests Using Interfaces A, B, C, and D
Concerning the number of tests required to achieve repeatability with the 4 interfaces, no significant difference was observed among them in the measurement of PImax (P = .69) or PEmax (P = .47). Regarding PImax, 49 of the 50 subjects met the criteria for repeatability with interfaces A, B, and D, and 45 met them with interface C. The number of tests was on average 3.80 ± 1.01 (A), 3.94 ± 1.34 (B), 4.24 ± 1.53 (C), and 3.96 ± 1.29 (D). Regarding PEmax, 48 of the 50 subjects met the criteria for repeatability with interface A, 47 met them with B and C, and 50 met them with D. The number of tests was 4.24 ± 1.30 (A), 4.47 ± 1.32 (B), 4.50 ± 1.44 (C), and 4.14 ± 1.21 (D).
Discussion
The main findings of this study were:
The values obtained for the MRP (PImax and PEmax) parameters of maximum mean pressure, peak pressure, plateau pressure, and plateau variation did not differ significantly between the 4 different interfaces.
There was no significant difference among the 4 interfaces studied in the number of tests needed to achieve the repeatability criteria in the measurement of MRP (PImax and PEmax).
To our knowledge, only 2 studies have compared the influence of different mouthpieces on the MRP measurement. Koulouris et al32 compared 2 types of mouthpieces (flanged-type and rubber tube) in 21 healthy subjects and 40 patients divided into 2 subgroups, according to normal values39 of PImax. In cases where the inspiratory muscle strength was considered to be normal, significantly higher values of both PImax and PEmax were observed with the tubular mouthpiece. These authors suggested that the shape, size, and way of using the mouthpiece are factors that can interfere in the measurement of MRP, because they require activation and coordination of different groups of muscles according to the characteristics of the mouthpiece. This idea is shared by other authors.1–3,12–17
Tully et al40 studied 50 male patients with spinal cord injuries and observed significantly lower PEmax values when measurements were made with the flanged mouthpiece, compared with the tube-style one. In the present study, which included only healthy subjects, no significant differences were observed among the interfaces evaluated. Patients with muscular injury or respiratory disease may show changes in respiratory mechanics, which could account for the findings of Tully et al.40
In our study it was not possible to include the tubular plastic, cardboard mouthpiece, or circular rubber used by Black and Hyatt,39 and this could be considered a limitation. In order to ensure the acceptability of the test, the recommendation for the use of the flanged mouthpiece published in 2002 by the American Thoracic Society and European Respiratory Society,1 and reinforced by Evans and Whitelaw,17 was adopted. Another aspect to be considered is that the results of the present study cannot be generalized to children, the elderly, or unhealthy people.
Regarding the number of tests needed to achieve the criteria of acceptability and repeatability, the results of this study support the recommendations of the American Thoracic Society and European Respiratory Society1 and the Brazilian Thoracic Association,3 which were recently reiterated in a review on the topic.17 The results of this study showed that the subjects reached these criteria with approximately 4 tests (3.80–4.50) for both PImax and PEmax, with no significant difference between the evaluated interfaces.
This was the first clinical study performed with this digital manometer, which allows connection with a large number of available tubes and mouthpieces. Moreover, the software Manovac 3.0 provides an easy to use graphic interface allowing the user to register the subject's data, select the type of MRP test, visualize a graphical display of the test in real time, and access and store information from multiple tests. The analysis of values from curves displayed in the manometer represents an improvement in the assessment of respiratory pressure and may positively impact treatment decisions. The manometer also provides other interesting variables besides peak pressure and maximal mean pressure, including the plateau pressure and plateau variation. This last variable can provide relevant information regarding one-second time periods with less variability in the MRP curves. To the best of our knowledge, these variables have not been described, and future studies are needed to determine their role in MRP tests.
Conclusions
In conclusion, when PImax and PEmax were measured with 4 different interfaces, no significant difference was found in the values obtained for maximum mean pressure, peak pressure, plateau pressure, or plateau variation, nor was there a difference in the number of tests performed to meet the repeatability criteria. Thus, it might be interesting to consider the comfort reported by subjects who undergo MRP measurements. The results of the present study can be used as a framework for future studies investigating the influence of mouthpieces on respiratory muscle pressure in different patient populations.
Footnotes
- Correspondence: Verônica Franco Parreira PhD, Laboratório de Avaliação e Pesquisa em Desempenho Cardiorrespiratório, Universidade Federal de Minas Gerais, Avenida Antônio Carlos, 6627, 31.270–901, Belo Horizonte, Minas Gerais, Brazil. E-mail: veronica.parreira{at}pq.cnpq.br.
Dr Parreira presented a version of this paper at the European Respiratory Society Annual Congress, held September 18–22, 2010, in Barcelona, Spain.
This research was supported by Pró-Reitoria de Pesquisa da Universidade Federal de Minas Gerais, Fundação de Amparo à Pesquisa do Estado de Minas Gerais, and Conselho Nacional de Desenvolvimento Científico e Tecnológico. Dayane Montemezzo was partly supported by a scholarship from Coordenação de Aperfeiçoamento de Pessoal de Nível Superior.
- Copyright © 2012 by Daedalus Enterprises Inc.









{kind=link}
{kind=link}
{kind=link}
{kind=link}