

Abstract
While group C beta hemolytic streptococcal infections are uncommon in humans, group C beta hemolytic streptococcal pneumonia is exceedingly rare. To the best of our knowledge, only 2 cases of necrotizing pneumonia caused by group C beta hemolytic streptococcus have been reported in the past. Thus, we are reporting a rare case of necrotizing group C beta hemolytic streptococcal pneumonia in a young healthy adult with no risk factors.
Introduction
Group C β-hemolytic streptococci (GCBHS) is an uncommon cause of infection in humans, and GCBHS pneumonia is exceedingly rare. To the best of our knowledge, only 2 cases of necrotizing pneumonia caused by GCBHS have been reported in the past.1,2 We herein report a rare case of necrotizing pneumonia caused by GCBHS in a young healthy adult with no risk factors.
Case Report
A 28-year-old, previously healthy, Hispanic male presented with a sore throat, intermittent nonproductive cough, pleuritic chest pain, and a 4-day history of fever. He denied dyspnea, contact with any illness, recent travel, exposure to animals, or use of any tobacco products. Physical examination revealed an acutely ill appearing individual, with a respiratory rate of 22 breaths/min, heart rate of 110 beats/min, blood pressure of 110/70 mm Hg, temperature of 38.3°C, and oxygen saturation of 96% in ambient air. Examination of the oral cavity was normal. Chest examination revealed crepitations in the right side posteriorly. Other systemic examinations were normal. A complete blood count revealed a substantial increase in the white-blood-cell count (16,000 cells/mL), with a left shift (92% neutrophils), toxic granulations, and Döhle bodies. Other laboratory findings, including basal metabolic panel, liver function tests, hemoglobin level, and coagulation tests, were all within normal limits, and his human immunodeficiency virus (HIV) test was negative.
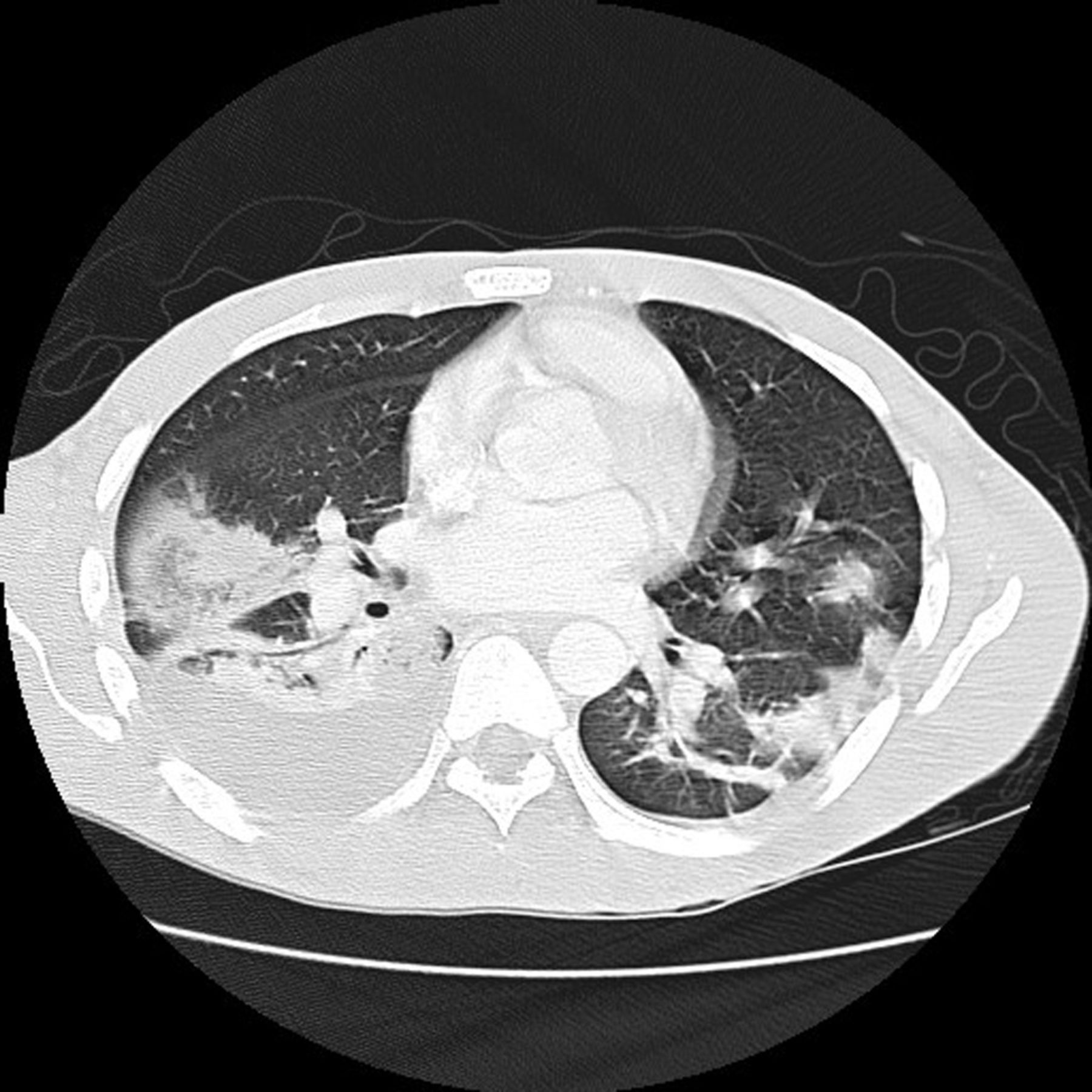
A chest radiograph showed a right lower lobe infiltrate, consistent with pneumonia. Since the patient was allergic to penicillin, intravenous levofloxacin was initiated for treatment of the pneumonia. Blood, urine, and sputum samples were collected for aerobic and anaerobic cultures. Due to continuing fever of up to 39.4°C, the chest radiograph was repeated 3 days later and showed increased predominant bilateral lower lobe pulmonary infiltrates. Computed tomography scan of the chest was done, which showed bilateral pleural effusions (Fig. 1) and patchy confluent areas of air space opacity in multiple lung fields bilaterally, with air bronchograms and several lung abscesses (Fig. 2). Necrotizing pneumonia was diagnosed, and the patient was started on broad-spectrum antibiotics (aztreonam and clindamycin) to cover all Gram-positive and Gram-negative organisms, pending the outcome of the sputum and blood cultures. A transesophageal echocardiogram was done, and it was normal.
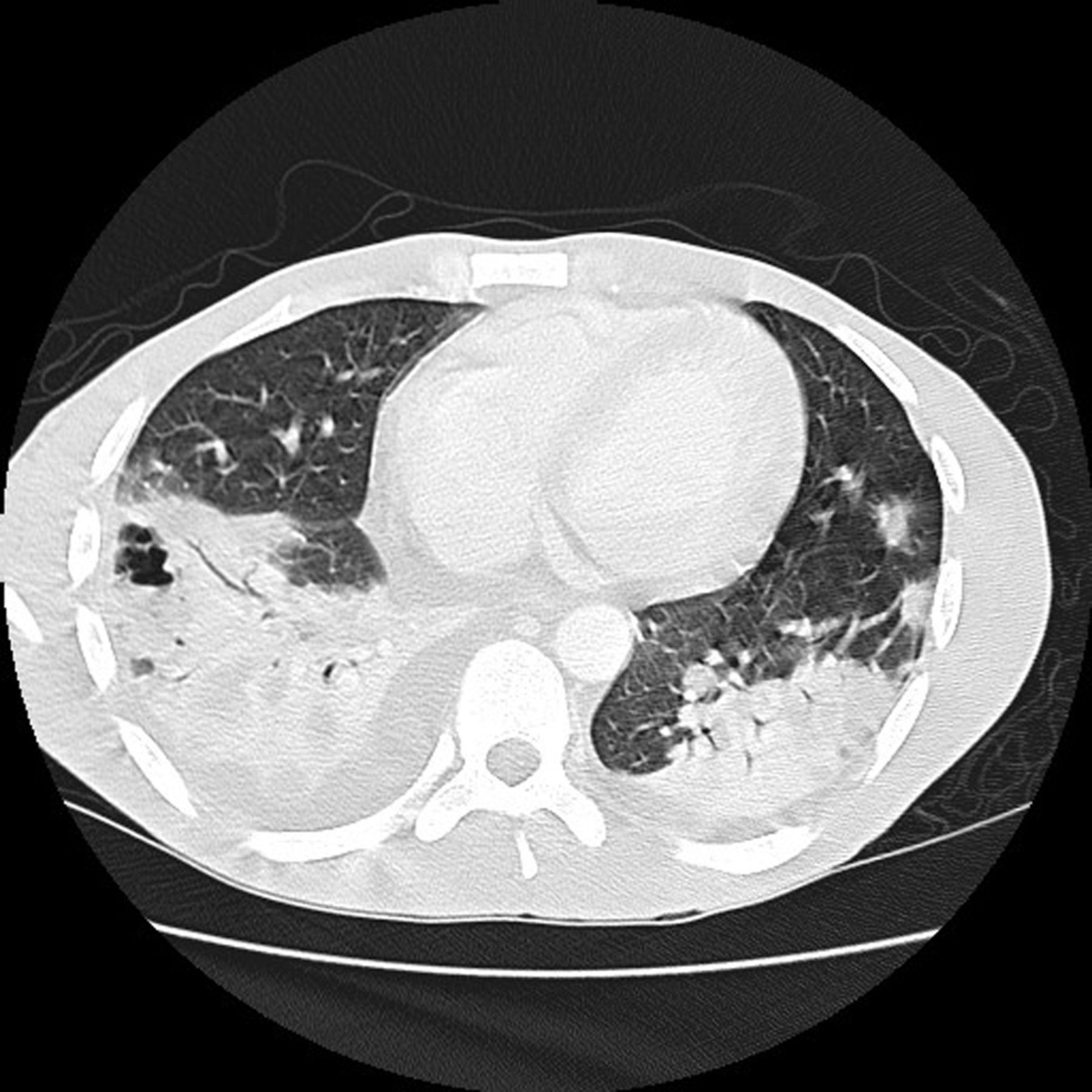
Computed tomogram shows multiple lung abscesses (180 × 180 mm, 72 × 72 dots per inch).

Computed tomogram shows bilateral pleural effusion (180 × 180 mm, 72 × 72 dots per inch).
Three anaerobic blood cultures all grew GCBHS. Susceptibility testing showed the organism to be sensitive to clindamycin, erythromycin, penicillin G, and vancomycin. Species identification was not carried out because it would have not changed the choice of antibiotics or the management of our patient in any way. The diagnosis was revised to necrotizing pneumonia due to GCBHS, and treatment with intravenous aztreonam and clindamycin were continued. Typical parapneumonic effusions, as in our case, resolve when the patient receives appropriate antibiotic therapy. Our patient did not have a loculated pleural effusion: it was more of a “lung abscess.” Therefore, thoracocentesis was avoided.
The patient's condition improved dramatically, and he was discharged home on 4 weeks of ciprofloxacin and clindamycin. A computed tomography chest scan repeated a few weeks later showed complete resolution of the above findings.
Discussion
Necrotizing pneumonia is a serious complication of pneumonia. Some authorities use the term “necrotizing pneumonia” or “lung gangrene” to distinguish pulmonary necrosis with multiple small abscesses (usually < 2 cm) from lung abscess (a larger cavitary lesion), but these actually represent a continuum of the same process. Necrotizing pneumonia involves necrosis and liquefaction of lung parenchyma. It has severe clinical manifestations and is confirmed by chest radiography. It requires a prolonged course of antibiotic therapy.
Anaerobes are the most common cause of pleuropulmonary infections, including necrotizing pneumonia.3 Peptostreptococcus species, Bacteroides species, Fusobacterium species, and microaerophilic streptococci are the most common pathogens.3 There are some aerobic bacteria that may infrequently cause lung abscess, including Staphylococcus aureus, Streptococcus pyogenes, Streptococcus pneumoniae (rarely), Klebsiella pneumoniae, Haemophilus influenzae, Actinomyces species, Nocardia species, and Gram-negative bacilli.4–8 To the best of our knowledge, lung abscess due to GCBHS is exceedingly rare and has been reported only twice in the past.1,2
GCBHS are Gram-positive facultative anaerobes that produce small (< 0.5 mm) or large (> 0.5 mm) colonies on sheep blood agar and occasionally cause human infections. Traditionally, group C streptococci (GCS) include Streptococcus dysgalactiae subspecies dysgalactiae and subspecies equisimilis, Streptococcus equi subspecies equi and subspecies zooepidemicus, Streptococcus anginosus, Streptococcus constellatus subspecies pharyngis, and Streptococcus phocae.9 The small colony isolates are currently designated as Streptococcus milleri or Streptococcus anginosus group. In animals they are thought to cause equine strangles, bovine mastitis, and porcine arthritis; however, GCBHS are rarely the cause of pneumonia in humans.10
GCBHS usually affect young, healthy, immunocompetent adults. In 9 well-described cases of GCHBS pneumonia in the literature, the patients were all under 40 years of age.1,10–17 Despite the frequent presence in animals, only occasional reports of GCS infections in humans include information about exposure to animals,18 as in our patient, who denied any animal exposure. Frequent underlying characteristics of patients with GCS infections are age > 65 years, male, underlying medical conditions including cardiovascular disease, diabetes mellitus, cirrhosis, chronic alcoholism, bone and joint disease, dermatologic processes, an immunocompromised state, and animal or animal product exposure.19,20 Interestingly, other than being male, our patient did not have any of the aforementioned risk factors.
Clinically, as in our case, patients present with high grade fever, chills, sore throat, and cough. These patients are often initially thought to have pharyngitis or bronchitis and are treated accordingly.10,12–14,17 Eventually as the disease progresses, they develop lobar pneumonia and pleural effusion.1,10–17 Most usually also develop bacteremia. Our patient presented in this described manner, and eventually developed necrotizing pneumonia and pleural effusion. The outcome for these patients depends on early diagnosis and treatment: of the 9 well described cases referred to previously, 3 died with cardiorespiratory arrest,12,13,15 and one had a fulminant course, developing pericarditis, mediastinitis, disseminated intravascular coagulopathy, and ARDS.1 These infections usually respond well to penicillin.
The majority of GCS strains demonstrate in vitro susceptibility to the penicillins, vancomycin, erythromycin, and the cephalosporins.21 Antimicrobial tolerance (defined as a minimum bactericidal concentration 32 or more times higher than the minimum inhibitory concentration [MIC]) among GCS and group G streptococci (GGS) has been reported for penicillin and other agents.22 Only a few clinical isolates have been reported to exhibit tolerance to vancomycin.22
Given that results were equivocal, Zaoutis et al23 further investigated these antibiotic susceptibility patterns among GCS and GGS isolated from patients with invasive infections (eg, bacteremia and meningitis). Their findings support the use of penicillin G as the antimicrobial agent of choice for GCS infections. All MICs were less than 0.03 μg/mL, and tolerance was not identified. All isolates in the study were susceptible to vancomycin (MICs ranging between 0.12 and 0.5 μg/mL). No GCS isolates exhibited tolerance. Since there are few reports in the literature of GCS isolates examined for vancomycin tolerance, the importance of this difference between GCS and GGS is unclear. These findings suggest that for patients with invasive GCS infections who cannot be treated with penicillin, tolerance to other antimicrobial agents, including vancomycin, should be closely monitored.
Our patient was treated with clindamycin and aztreonam, as he was allergic to penicillin. In cases of complicated pleural effusion or development of empyema, a chest tube is required, and thoracotomy is required if closed chest tube drainage fails.
GCBHS are an exceedingly rare cause of necrotizing pneumonia and should be considered in the differential diagnosis of causative organisms. It is particularly difficult to diagnose in patients with no comorbid illness and no history of animal exposure. It usually affects young males and has a fulminant course, with very high morbidity and mortality; therefore, early identification, close monitoring, and appropriate antibiotic therapy are key to survival.
Footnotes
- Correspondence: Vikas Pathak MD, Division of Pulmonary Diseases and Critical Care Medicine, Department of Medicine, University of North Carolina, 130 Mason Farm Road, CB# 7020, Chapel Hill NC 27599. E-mail: drvikaspathak{at}gmail.com.
The authors have disclosed no conflicts of interest.
- Copyright © 2012 by Daedalus Enterprises Inc.









{kind=link}
{kind=link}