

Abstract
Hypersensitivity pneumonitis is an immunologic reaction to an inhaled antigen, with a wide spectrum of clinical presentations. The most common manifestations are fever, cough, and dyspnea. We describe a case of hypersensitivity pneumonitis with marked alveolar lymphocytosis; the patient presented with respiratory failure and shock requiring mechanical ventilation and vasopressive agents. We hypothesized that immune mediators implicated in the pathogenesis of hypersensitivity pneumonitis were responsible for the transient shock observed in this patient.
Introduction
The clinical presentation of hypersensitivity pneumonitis varies from acute febrile reaction to a more insidious onset. A wide array of airborne antigens has been associated with the development of hypersensitivity pneumonitis, bacterial products and fowl proteins being the most common. The diagnosis of hypersensitivity pneumonitis is based upon a high index of suspicion, exposure history, high-resolution computed tomography, and marked lymphocytosis.1
Case Report
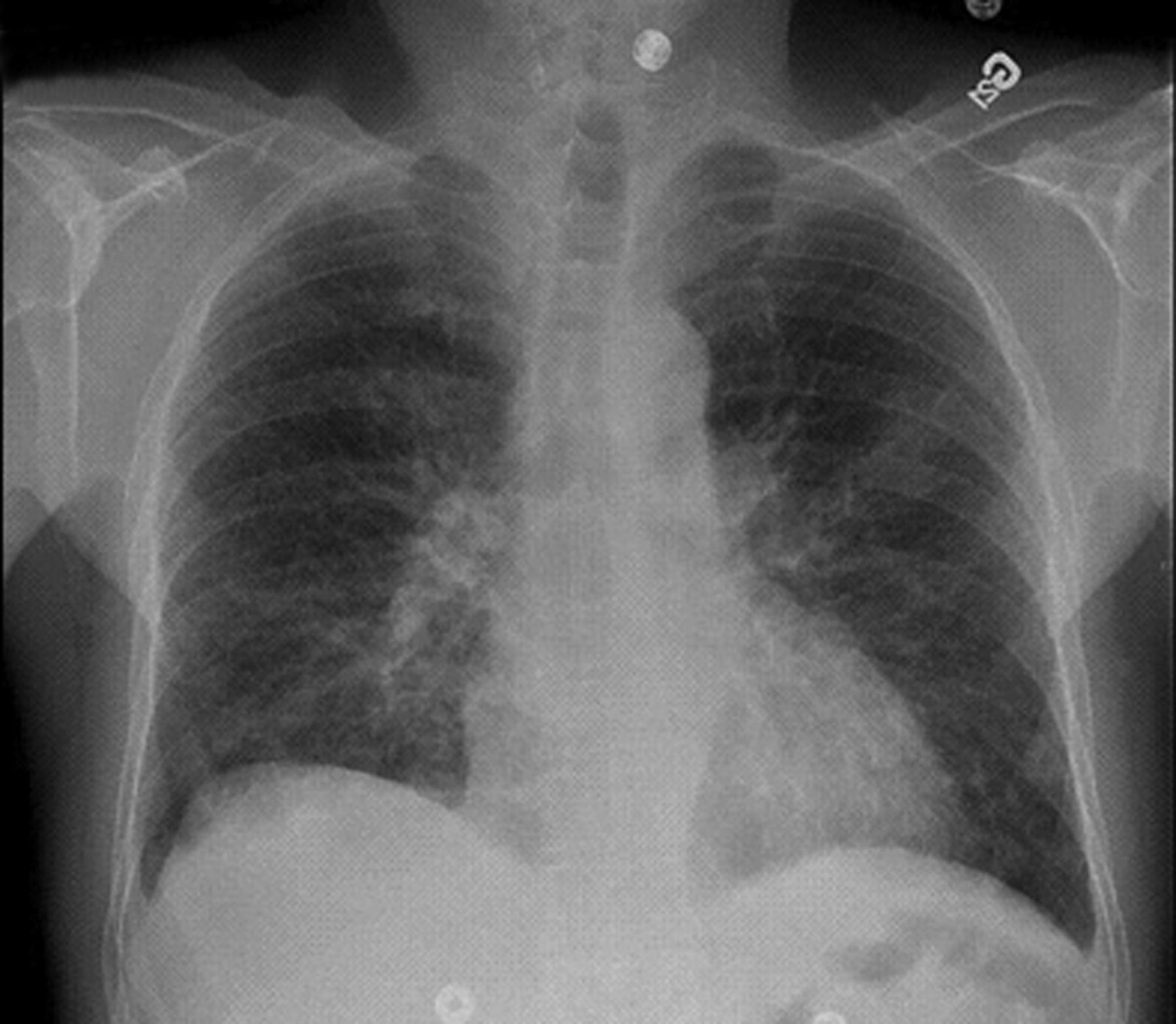
A 62-year-old, non-smoking farmer with no preexisting illness presented to the emergency room with progressive dyspnea and cough of 10 days duration. He also complained of fatigue, headache, and nausea. On arrival, he was febrile (39.7°C), and had mild hypotension (102/62 mm Hg) and tachycardia (128 beats/min). He was breathing at 40 breaths/min and his O2 saturation was 88% despite 100% O2 with rebreathing face-mask. Diffuse crackles were audible on chest auscultation. He was transferred to the intensive care unit and rapidly required endotracheal intubation. Vasopressor drugs (norepinephrine 0.8 mg/h) were introduced 2 hours after admission, because of refractory hypotension (88/48 mm Hg) despite volume repletion (4.5 L). In addition to maximal ventilatory support, inhaled nitric oxide was needed to maintain PaO2 > 60 mm Hg. Chest x-ray (CXR) showed bilateral interstitial infiltrates (Fig. 1) that progressed to bilateral alveolar infiltrates. Complete blood count showed marked leukocytosis (23.0 × 106/mL), with neutrophilia and lymphopenia.

Initial CXR shows reticular infiltrates of perihilar distribution, with ground-glass opacities.
The patient was empirically treated with ceftriaxone and levofloxacin after extensive samplings for cultures. He also received intravenous hydrocortisone and drotrecogin alpha for worsening of organ failures, including transient acute renal failure. The vasopressor drugs were progressively tapered, and the FIO2 was brought down progressively to 0.40 after 48 hours. The patient was weaned from ventilator support on day 4. Blood and urine culture were negative, and no urinary antigen was found for Haemophilus influenzae, Streptococcus pneumoniae, Neisseria meningitidis, Blastomyces species and Histoplasma species. Bronchial cultures taken during bronchoscopy showed no growth, and polymerase chain reaction technique was negative for hantavirus, influenza, and respiratory syncytial virus. Immunofluorescence technique was also negative for adenovirus, influenza, parainfluenza, and respiratory syncytial viruses. No bronchoalveolar lavage was performed. Nasal swab culture revealed the presence of 3 species of aspergillus (nidulans, glaucus, and terreus) and mucormycosis. The patient initially denied any exposure to moldy hay, birds, or unusual dust, but reported recurrent episodes of fever and dyspnea occurring at night over the last 2 months. Because the patient initially presented with ARDS and shock, which improved with initial antibiotics, the diagnosis was presumed to be bacterial pneumonia. The patient was discharged from the hospital on day 23, with minimal residual reticulation on the CXR (see Fig. 2).
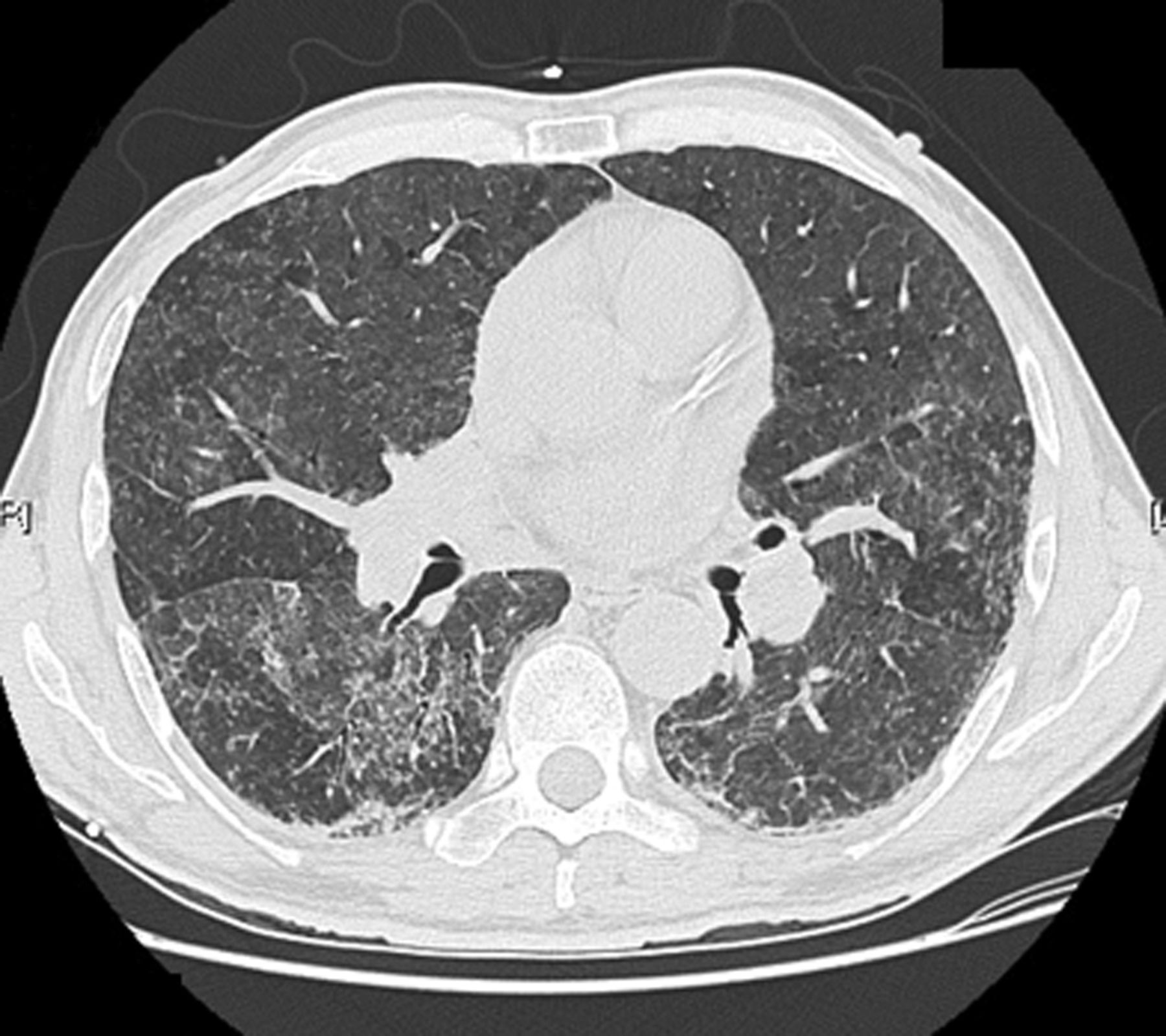
On hospital day 23 the infiltrates had regressed.
The patient returned to work in the following days. He consulted 17 days later with recurrence of dyspnea, weakness, fever (38.8°C), and chills. The patient then admitted recurrent exposure over the last 2 months and even chainsaw-cutting through moldy hay over the 2 weeks preceding the previous hospitalization. This created a thick cloud of dust before the hay was spread as bedding for his cows. On admission, CXR showed worsening of interstitial infiltrates (Fig. 3). A high-resolution computed tomography (Fig. 4) showed centrolobular ground glass opacities, with areas of hypoattenuation. A bronchoscopy with lavage was negative for bacteria, mycobacteria, and fungus, including Pneumocystis jiroveci, but yielded 220 × 106 white blood cells, 92% of which were lymphocytes. No biopsy was taken. Serum precipitins for farmer's lung antigens (Saccharopolyspora rectivirgula) were positive. A diagnosis of farmer's lung-induced hypersensitivity pneumonitis was made, and the patient was strongly advised to avoid any exposure to moldy hay.

Seventeen days after discharge the infiltrates had recurred and the patient was readmitted.
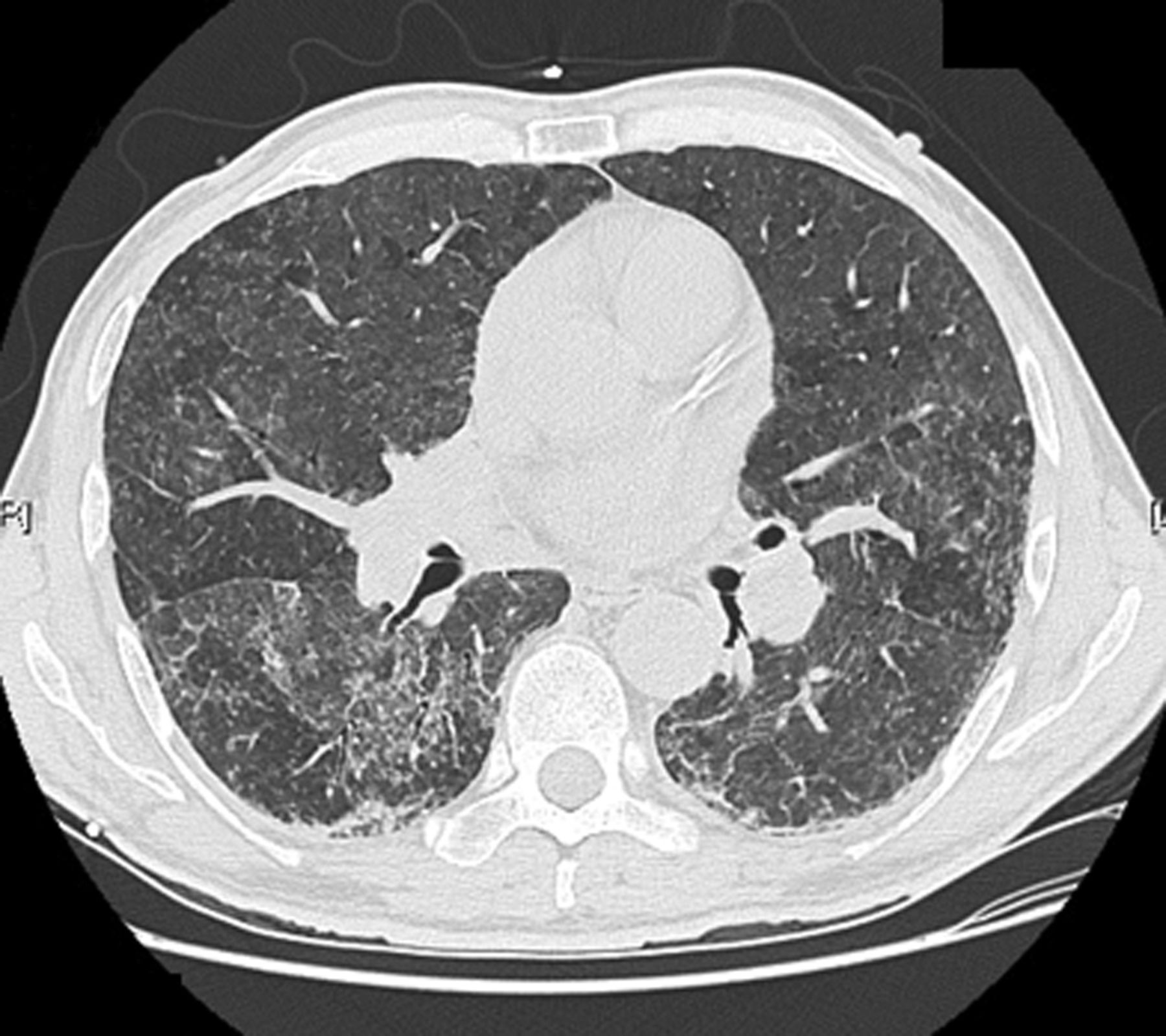
High-resolution computed tomography confirmed centrolobular ground-glass opacities, hypoattenuated areas, as well as coarse reticulations.
Discussion
Hypersensitivity pneumonitis is an immune reaction of complex origin, involving alveolar macrophages, immunoglobulin G, complement cascade, neutrophils, and T lymphocytes.2 It usually presents as a delayed dyspnea and cough after exposure to the causative antigen, and requires stringent documentation of medical history and collective input from pulmonologists, radiologists, and, occasionally, pathologists. To our knowledge, no reports have ever described a hypersensitivity pneumonitis reaction of this intensity accompanied by severe shock.
In the present case the clinical presentation with recurrent episodes of symptoms following exposure to a known offending antigen, the presence of diffuse crackles and positive serum precipitins for Saccharopolyspora rectivirgula were highly suggestive of farmer's lung-induced hypersensitivity pneumonitis.3 The marked alveolar lymphocytosis, as well as the centrolobular ground glass opacities and areas of hypoattenuation on high-resolution computed tomography, is also a characteristic finding of hypersensitivity pneumonitis.1 The reoccurrence of acute hypersensitivity pneumonitis and his subsequent re-hospitalization after only 17 days was likely to result from re-exposure. Importantly, the fact that the diagnosis of hypersensitivity pneumonitis was missed during the initial hospitalization emphasizes the challenges in diagnosing this multifactorial and multifaceted disease. The initial differential diagnosis included mycotoxicosis (also known as organic dust toxic syndrome) and severe sepsis. However, mycotoxicosis is characterized by symptoms of short duration (hours), normal CXR and absence of shock. Furthermore, mycotoxicosis is associated with alveolar neutrophilia on bronchoalveolar lavage, followed by mild lymphocytosis.4 Alveolar neutrophilia is also generally observed in infectious processes. This contrasts with the massive lymphocytosis observed in our patient. Finally, sepsis seemed less likely, considering that extensive cultures, viral search, and serology showed no evidence of a causative infectious organism.
Numerous pro-inflammatory cytokines have been implicated in the pathogenesis of hypersensitivity pneumonitis.4 Tumor necrosis factor alpha and interleukin-1 (IL-1) play a role in enhancement of inflammation. IL-8 and granulocyte macrophage colony stimulating factor are also increased and act as chemotactic factors for neutrophils and activators of alveolar macrophages, both of which subsequently produce oxidants, resulting in damages of the fine alveolar lining and capillary leak.5 Interestingly, IL-2 is also increased in bronchoalveolar lavage of patients with hypersensitivity pneumonitis.6 IL-2 is a 15 kilodalton glycoprotein produced by activated T lymphocytes, which has been used in several cancer clinical trials. Despite survival benefit, its use has been limited, due to its cardiovascular toxicity, mainly hypotension, requiring vasopressors in as many as 65% of patients.7 Although IL-2 was not measured in the patient's serum or bronchoalveolar lavage, IL-2 could have contributed, in addition to other pro-inflammatory cytokines involved in hypersensitivity pneumonitis pathogenesis, to the occurrence of shock in this patient with initially undiagnosed hypersensitivity pneumonitis. The farmer's indifference to occupational hazard may also be in part responsible for the emergence of untreated hypersensitivity pneumonitis and the subsequent ARDS-like reaction and shock.
We thus hypothesized that the immunologic pathways implicated in the pathogenesis of hypersensitivity pneumonitis were responsible for the severe hypotension and ARDS-like reaction observed in our patient. This case also illustrates the challenge in diagnosing hypersensitivity pneumonitis and the need to keep a high index of suspicion for this disease.
Footnotes
- Correspondence: Steeve Provencher MD MSc, Centre de Recherche, Institut Universitaire de Cardiologie et de Pneumologie de Québec, 2725 Chemin Ste-Foy, Québec, Canada G1V 4G5. E-mail: steve.provencher{at}criucpq.ulaval.ca.
The authors have disclosed no conflicts of interest.
- Copyright © 2012 by Daedalus Enterprises Inc.









{kind=link}
{kind=link}
{kind=link}
{kind=link}