

Abstract
BACKGROUND: Pulmonary function, in HIV infected patients, has been associated with reduction in pulmonary ventilation parameters.
METHODS: We conducted a prospective cross sectional study to evaluate the pulmonary function of AIDS patients cared for in the infectious diseases ambulatory care clinic. Maximal inspiratory (PImax) and expiratory (PEmax) pressures and spirometry were assessed. Clinical, demographic, and laboratory data were also evaluated.
RESULTS: PImax and PEmax were assessed in 73 and spirometry in 54 subjects. The mean time of HIV infection (in years) was similar for men (8.5 ± 5.1 y) and women (10.4 ± 4.2 y, P = .13), and the mean time of use of antiretroviral therapy was 8.5 ± 4.1 years for women and 7.7 ± 4.1 years for men (P = .46). PImax and PEmax values were normal in 35 (48%) and 48 (66%) subjects, respectively. The use of tenofovir and presence of cough, by the time the test was performed, were independently associated with PEmax below the predicted value. Elevated creatine kinase values were associated with prolonged antiretroviral usage (9.6 ± 4.1 y vs 7.4 ± 3.9 y, P = .05). FVC was reduced in 14 (26.4%) subjects and was independently associated with high and/or intermediate cardiovascular risk (P = .002), and those with reduced vesicular murmur in auscultation (P = .047). FEV1 was significantly lower in subjects with prolonged time of smoking (P = .02) and high and/or intermediate cardiovascular risk (P = .003). Reduced FEV1/FVC was associated with smoking (P = .041).
CONCLUSIONS: AIDS subjects, in our study, had reduced parameters of maximal respiratory pressures and spirometry. The frequent dysfunction of respiratory muscles might be due to the association of multiple factors and not a particular one; moreover, smoking was independently associated with abnormal airway function. Pulmonary function tests should be implemented as an essential part of the medical assistance to AIDS patients.
- acquired immune deficiency syndrome
- AIDS
- pulmonary function
- spirometry
- physiotherapy
- smoking
- antiretroviral therapy
Introduction
AIDS patients are subjected to several pulmonary dysfunctions associated with opportunistic infections such as Pneumocystis jiroveci, Cryptococcus species, mycobacterial disease, and viral infections. Pulmonary function has been studied in HIV infected patients with AIDS and non- AIDS, and has been associated with reduction in pulmonary ventilation parameters. The use of nucleoside reverse transcriptase inhibitors as a major therapy in these patients has been related to mitochondrial dysfunction and decrease in muscle strength. Tobacco use in HIV patients, though not associated with an increased risk to progression of HIV infection in men1 or with risk of death due to AIDS in women,2 is well known as a risk-factor for cardiovascular disease, lung disease, and cancer.
AIDS in Brazil is estimated to be 20 cases per 100,000 habitants, and the ratio of men to women was 1.6 to 1 in 2009.3 However, though HIV infection has been highly prevalent in Brazil, few studies have been conducted evaluating the pulmonary function in the HIV/AIDS Brazilian population.4 The objective of this study was to evaluate the respiratory parameters in AIDS patients assisted in a university hospital, in accordance with clinical and epidemiological characteristics.
QUICK LOOK
Current knowledge
Antiretroviral treatment in patients with acquired immune deficiency syndrome (AIDS) may cause mitochondrial dysfunction and decline in muscle strength.
What this paper contributes to our knowledge
Respiratory muscle dysfunction, as measured by declining maximal inspiratory and expiratory pressures, is common in patients with AIDS. The etiology is multifactorial.
Methods
The study was conducted at the hospital of the State University of Campinas, São Paulo, Brazil, a 400-bed tertiary-care university hospital that provides all major medical services as the reference hospital for 5 million inhabitants, except for gynecology-obstetrics cases and neonates.
This cross-sectional study included AIDS patients assisted in our infectious diseases ambulatory care clinic from April 2009 to February 2010. AIDS patients over 18 years old were included. Exclusion criteria included: cognitive deficit, presence of pulmonary disease, tuberculosis (cured or not), past myocardial infarction, pneumothorax, recent surgery, abdominal hernia, neurological disorders, cardiac insufficiency, uncontrolled diabetes mellitus, and glaucoma.
Patients were invited to participate in the research and to sign the informed consent authorized by our institution's ethics committee. The following data were collected from their records: age, sex, time of known HIV infection, staging of HIV infection (Centers for Disease Control classification), use of antiretroviral therapy, time under antiretroviral therapy, underlying conditions, opportunistic infections, and latest results of the following exams: hemoglobin, hematocrit, total leukocytes, platelet, fasting glucose (reference < 100 mg mg/dL), serum creatinine (reference male ≤ 1.2 mg mg/dL, reference female ≤ 0.9 mg mg/dL), alanine aminotransferase (reference male < 50 U/L, reference female < 34 U/L), aspartate aminotransferase (reference male < 33 U/L, reference female < 27 U/L), creatine kinase (reference male < 170 U/L, reference female < 145 U/L), CD4 lymphocyte count, and HIV viral load. Subjects were asked about smoking, drinking, use of illicit drugs, and respiratory symptoms (cough, dyspnea, chest pain) at the moment of the interview. Physical examination, anthropometric measurements, and pulmonary auscultation were performed. Cardiac risk5,6 and body mass index were determined. Individuals were classified according to criteria established by the World Health Organization as to nutritional status.7,8
Pulmonary Function Tests: Maximal Respiratory Pressures and Spirometry
Maximum expiratory (PEmax) and inspiratory (PImax) pressures were assessed using a digital manovacuometer (MVD, +300/–300 cm H2O, Globalmed, São Paulo, Brazil). The same investigator (Morsch) did all the measurements. The tests followed the recommendations of Black and Hyatt (1969).9 PEmax was measured near the total lung capacity after the maximal inspiration, and PImax was measure near the residual volume after a maximal expiration The maneuvers were repeated 3 times, and the highest value was recorded. Determination of the predicted values of the maximal respiratory pressures were calculated adjusting to sex and age,10 as follows:
The lower limit of the normal predicted value was calculated using the equation11
The results of PEmax and PImax achieved by the subjects were considered normal when their values were inside the intervals of the predicted and normal inferior limit values.
Spirometry was performed according to the American Thoracic Society recommendations,12 using the MicroLoop spirometer (MicroMedical Technologies, Chatham, Illinois). FVC, FEV1, and FEV1/FVC values were obtained by FCV maneuver. Spirometry results were recorded in percentages of the reference values described for Brazilian populations.13
Statistical Analysis
Categorical variables were analyzed using the chi-square and Fisher tests. For continuous variables, analysis of variance (Mann-Whitney/Wilcoxon 2-sample test) was used. The categorical parameters of lung function were analyzed by logistic regression, and the associate variables of numeric parameters of lung function were analyzed by linear regression analysis. Univariate and multivariate models and the stepwise criteria to select variables were applied. A P value ≤ .05 was considered significant. The following variables were not included in the univariate and multivariate analysis of PImax, PEmax, and in the linear regression analysis of FVC, FEV1 and FEV1/FVC: hemoglobin, hematocrit, total leukocytes, platelet, fasting glycemia, serum creatinine, alanine aminotransferase, aspartate aminotransferase and creatine kinase. Statistical analysis was performed using the SAS System for Windows, version 9.1.3, SAS Institute, Cary, North Carolina.
Results
Characteristics of the Study Population and Demographic Data
Eighty-six patients were invited to participate in the study. PImax and PEmax were assessed in 73 (92.4%) subjects, and spirometry was performed in 54 (68.4%) subjects. Seven patients did not complete the respiratory function tests and were excluded. The distribution of our adult population, according to sex and age, was similar to the Brazilian AIDS population characterized in a publication of the Ministry of Heath bulletin.3 Mean age for men and women was 43 ± 10 years and 42 ± 7.7 years, respectively. The ratio of men to women was 1.5 to 1, and 44 (60.3%) were male.
In 55 subjects, HIV infection as acquired by sexual route. Forty-three subjects (44%) were category C (Centers for Disease Control classification), and the mean time of HIV infection (in years) was similar for men (8.5 ± 5.1 y) and women (10.4 ± 4.2 y, P = .13). HIV viral load was undetectable in 62 (85%) subjects. The mean CD4 cells/mL was higher in women (782 ± 332.7 cells/mL) than in men (608.4 ± 270 cells/mL) (P = .01). Forty-nine (62%) subjects had CD4 count ≥ 500 cells/mL, 21 (26.6%) from 350 to 499 cells/mL, and only 9 (12%) subjects had CD4 ≥ 200 to 349 cells/mL.
Smoking was more frequent in women (10, 34.5%) than in men (6, 13.6%) (P = .03). Cardiovascular risk was low in 70 (88.6%) subjects, intermediate in 6 (7.6%), and only 3 (3.8%) subjects were classified as high cardiovascular risk. The mean value of body mass index of our population was 24.45 ± 4.2 kg/m2; 45 (57%) subjects had normal weight, 31 (39.2%) were overweight or obese, and 3 (3.8%) were underweight. Most of our subjects had the results of blood tests inside the normal range of the reference values (Table 1).
Distribution of the Blood Tests Results of the 79 AIDS Subjects
Antiretroviral therapy was administrated to 94.5% of our study population. The mean time of use of antiretroviral therapy was 8.5 ± 4.1 years for women and 7.7 ± 4.1 years for men (P = .46). The triple therapy, azidothymidine (AZT) + 2′,3′-dideoxy-3′-thiacytidine (3TC) + efavirenz, was prescribed for 39 (49.4%) subjects, and salvage therapy regimens were used in 24 (30.4%) subjects. AZT + 3TC was used in 52 subjects; protease inhibitors (lopinavir + ritonavir or atazanavir + ritonavir) were prescribed for 27 subjects, and tenofovir for 17 subjects. Other antiretrovirals were less frequently prescribed. Subjects under prolonged time of antiretroviral usage were likely to have elevated creatine kinase values (9.6 ± 4.1 years vs 7.4 ± 3.9 years, P = .05).
Respiratory symptoms at the time of the interview were as follows: dyspnea in 12 (15.2%) subjects, cough in 13 (16.5%) subjects, and chest pain in 4 (5.10%) subjects. Forty-five percent (33/73) of the subjects had reduced vesicular murmur, and 11 (15%) subjects had rales in the pulmonary auscultation. Subjects with reduced breath sounds were not correlated, in the univariate analysis, with prolonged time of HIV diagnosis (P = .062), age (P = .56), time of use of antiretroviral therapy (P = .96), time of smoking (P = .13), or smoking (P = .10).
Opportunistic infections occurred in 50 subjects (63.3%), and the most frequent opportunistic infections were: oral or esophageal candidiasis, 28 episodes; pneumocystosis, 10 episodes; central nervous system toxoplasmosis, 10 episodes; and herpes zoster, 17 episodes. The occurrence of opportunistic infection was not associated with abnormal values of PEmax (P = .50) and PImax (P = .20), and, interestingly, previous pneumocystosis was not associated with maximal pressures values below predicted values or with altered spirometry.
Maximal Respiratory Pressures
PImax values were normal in 35 (48%) subjects and PEmax values were normal in 48 (66%) subjects (Fig. 1). Twenty-seven (37%) subjects had normal values of PEmax and PImax, 17 (23%) had both PEmax and PImax below the inferior limit, and 29 (39.7%) had PEmax or PImax below the inferior limit. Normal values of PImax and PEmax were achieved similarly by men and women (PImax P = .24, PEmax P = .23) (Table 2).
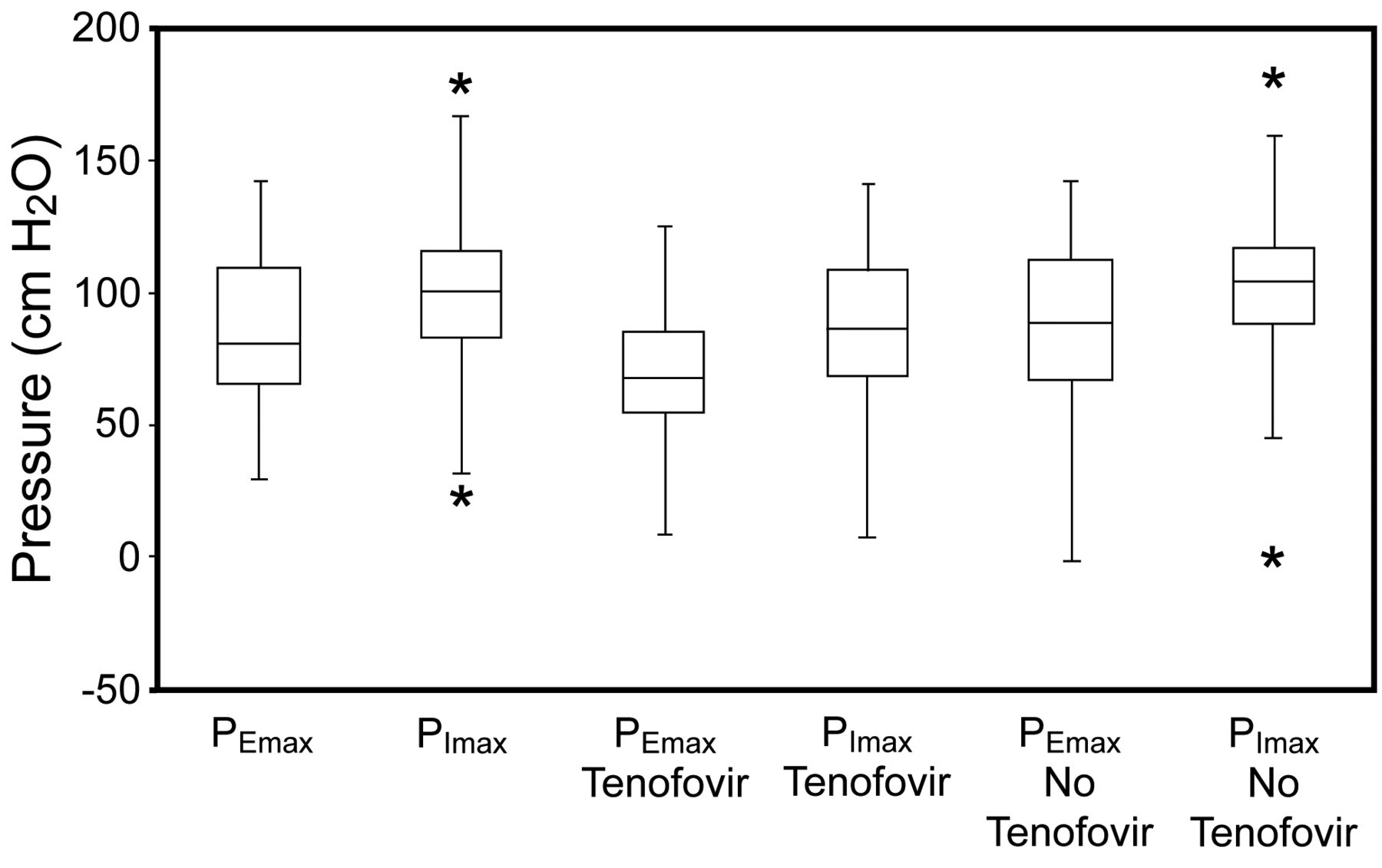
Box plot presentation of the maximal respiratory pressures of 73 AIDS subjects. PEmax = maximal expiratory pressure. PImax = maximal inspiratory pressure. The box part of the box and whisker plot represents the central 50% of the data or the interquartile range. The lower edge of the box plot is the first quartile or 25th percentile. The upper edge of the box plot is the third quartile or 75th percentile. (* P = .04).
Maximal Respiratory Pressures and Spirometry Parameters
No statistical significant variable was associated with reduced values of PImax in the multivariate analysis. However, independent variables associated with reduced PEmax were the presence of cough (P = .01) and the use of tenofovir (P = .039). Subjects under use of tenofovir had 4.2 times higher risk of having reduced PEmax value (Fig. 1, Table 3). Of note, in subjects presenting both PEmax and PImax below the inferior limit, tenofovir was prescribed in 8 (47%) of the 17 subjects. Cough was independently associated with reduction in PEmax, and subjects with cough, at the time of the interview, had 6.8 times higher risk of having PEmax results below the predicted value.
Variables Independently Associated With Altered Lung Function Tests
Spirometry
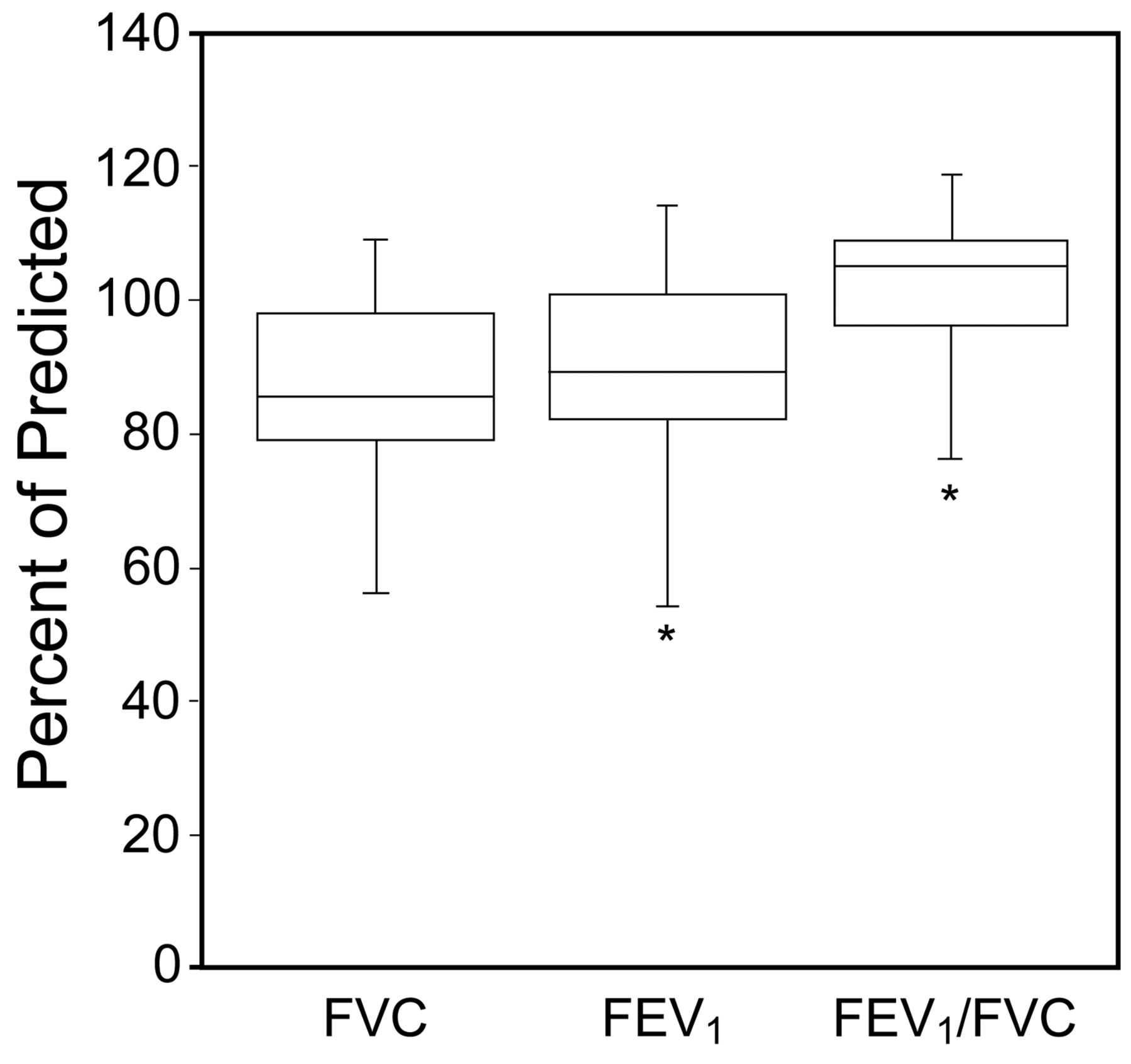
The spirometry parameters were normal in 45 (83.3%) subjects, obstructive in 1 (1.0%), and 8 (14.8%) subjects had restrictive parameters. FVC was reduced in 14 (26.4%) subjects and was independently associated with high and/or intermediate cardiovascular risk (P = .002), and with reduced vesicular murmur in auscultation (P = .047). Nine (17%) subjects had reduced FEV1, and FEV1 results were significantly lower in subjects with prolonged time of smoking (P = .02) and high and/or intermediate cardiovascular risk (P = .003). FEV1/FVC reduced ratio was associated with smoking (P = .041) (see Table 1, Fig. 2).
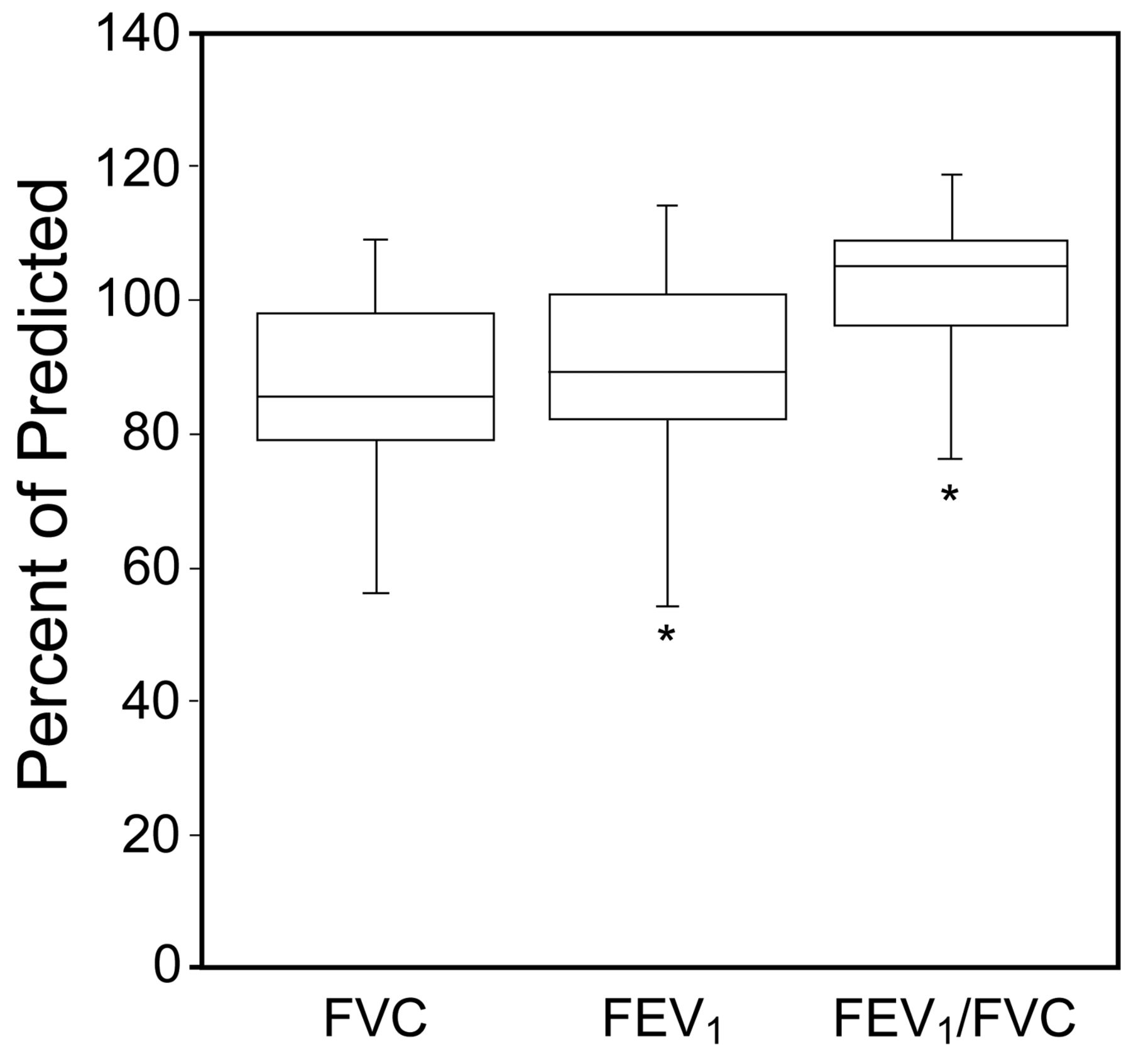
Box plot presentation of spirometry results of 54 AIDS subjects. The box part of the box and whisker plot represents the central 50% of the data or the interquartile range. The lower edge of the box plot is the first quartile or 25th percentile. The upper edge of the box plot is the third quartile or 75th percentile. * Minimum and maximum outliers.
Discussion
Antiretroviral therapy has revolutionized the care of patients with HIV infection. However, the lungs remain frequently affected by opportunistic infections and other non-infectious diseases in this population.
We conducted a cross- sectional study in an attempt to evaluate lung function in patients assisted in our AIDS ambulatory care, and we found that our study population had important reduction in respiratory muscle strength expressed by reduced maximum respiratory pressures. Only 37% of our subjects achieved the predicted maximum respiratory pressure values. A previous study conducted elsewhere in Brazil reported that only 39.4% and 60% of AIDS subjects achieved the predicted values of PEmax and PImax, respectively.4 Reports in the literature have shown abnormal airway function in 33% of AIDS subjects.14 Schulz et al15 showed that 23% and 32% of the control subjects achieved significantly higher values of PImax and PEmax, respectively, when compared to HIV subjects. Lung infections have been associated with permanent declines in pulmonary function,16 and pneumocystosis and bacterial pneumonia were associated with permanent decreases in FEV1, FVC, and FEV1/FVC.
In our study population, high/intermediate cardiovascular risk, smoking, and prolonged time of smoking were important independent variables associated with altered spirometry tests (see Table 3), and our results might suggest that we should work harder in reducing smoking in AIDS patients. Smoking was significantly associated with reduced FEV1. Several studies on lung function in HIV subjects have shown a reduction in carbon monoxide transfer factor17 and continuing lung damage in subjects who are clinically stable and have no overt lung disease.18 Moreover, tobacco was associated with an increased risk for opportunistic infection in HIV subjects.19 In our study group, 32 (43%) subjects had a history of smoking; 16 (21.6%) subjects at the time of the interview were still smoking, with a mean time of smoking of 20.3 years (range from 6 to 41 years), and 16 had quit smoking. Surprisingly, 34.5% of the women in our group were smokers, and it is known that smoking affected the prognosis of HIV women leading to a higher risk of non-AIDS-related death.2 Of note, smoking in HIV/AIDS subjects also doubled the risk for pneumocystosis and for developing tuberculosis,19 and there is evidence of continuing lung damage in HIV-positive subjects who are clinically stable.18
The use of tenofovir was interestingly associated with PEmax values below the inferior limit in our subjects. PEmax is intrinsically linked to the ability of the respiratory muscles, and reduced pressure values infer several physical and pulmonary conditions, including neuromuscular disorders. Tenofovir has mitochondrial toxicity,20 leading to different grades of myopathy that might have contributed to a reduced PEmax in our subjects. However, HIV also is known to cause myopathy in infected subjects, and to distinguish myopathy caused by the virus or drug-related has proved to be difficult.21
AIDS patients in Brazil have free access to medical assistance, antiretroviral therapy, and to prophylactic drugs for opportunistic infections. We did not include patients with active or past history of tuberculosis, because tuberculosis is the most important pulmonary infection in patients with AIDS in Brazil. Thus, we expected that our subjects might have relative good lung function parameters. However, the results observed in our study were disappointing, whereas only 25.7% of our study population had normal parameters of maximal respiratory pressures and spirometry.
Conclusions
In conclusion, our results suggested that the respiratory tract was highly affected in the AIDS population assisted in our ambulatory care clinic. The use of tenofovir was the only variable independently associated with decline in the respiratory muscles; moreover, tenofovir has been prescribed more frequently by doctors in Brazil and might represent an additional risk, compromising the function of the respiratory muscles. However, further studies will have to be conducted to get additional information. Additionally, smoking was definitely associated with abnormal airway function.
The high percentage of patients with decline in respiratory muscle strength might be due to multiple factors and not to any one factor. We suggest that lung function tests should be implemented as part of the routine tests for HIV patients.
Footnotes
- Correspondence: Maria Luiza Moretti MD, Internal Medicine Department, Faculty of Medical Sciences, State University of Campinas, Rua Tessália Vieira de Camargo 126, Cidade Universitária Zeferino Vaz, 13083–887 Campinas, São Paulo, Brazil. E-mail: mlmoretti{at}hc.unicamp.
The authors have disclosed no conflicts of interest.
- Copyright © 2012 by Daedalus Enterprises Inc.









{kind=link}
{kind=link}