

Abstract
The history of oxygen from discovery to clinical application for patients with chronic lung disease represents a long and storied journey. Within a relatively short period, early investigators not only discovered oxygen but also recognized its importance to life and its role in respiration. The application of oxygen to chronic lung disease, however, took several centuries. In the modern era, physiologists pursued the chemical nature of oxygen and its physiologic interaction with cellular metabolism and gas transport. It took brazen clinicians, however, to pursue oxygen as a therapeutic resource for patients with chronic lung disease because of the concern in the 20th century of the risks of oxygen toxicity. Application of ambulatory oxygen devices allowed landmark investigations of the long-term effects of continuous oxygen that established its safety and efficacy. Although now well established for hypoxic patients, many questions remain regarding the benefits of oxygen for varying severity and types of chronic lung disease.
Introduction
As used in clinical medicine, the word “oxygen” is a misnomer. It actually denotes elemental oxygen with an atomic number of 8 and a symbol of “O” rather than the “oxygen” we clinicians intend, which is dioxygen, or “O2,” and the stable molecular form of elemental oxygen (“O”). Oxygen's name also represents a misnomer, because it stems from the Greek roots “oxys,” meaning “sharp” in reference to the sour taste of acids and the assumption by Lavoisier that it was an essential element for all acids, and “-genes,” which means “begetter.”
Despite these irregularities, the word “oxygen” entered common usage during the late 18th century (despite opposition from leading scientists of the day) because of its mention in a popular book of poems, The Botanic Garden (1791) written by Erasmus Darwin, the grandfather of Charles Darwin.1
Although eventually established as being a nonessential moiety in acids, the naming of oxygen as “begetter” proved correct, considering the essential role it plays in sustaining life on our planet. In terms of mass, it is the third most abundant element in the universe, following hydrogen and helium. It constitutes 50% of the earth's crust and comprises a third of the mass of humans, finding its way into essential molecules such as proteins, carbohydrates, and fats in addition to non-cellular structural elements such as bones and teeth. But its role in aerobic respiration sparks the greatest interest for oxygen among pulmonary physicians and respiratory therapists. Oxygen serves as the final electron acceptor in catabolic reactions that convert biochemical energy from nutrients into adenosine triphosphate, which fuels the human body. Because of its highly reactive nature, oxygen serves as an effective electron accepter, or oxidizing agent. But this reactive nature that forms oxides when oxygen comes into contact with almost all other elements explains why it can exist in a free gaseous form only through ongoing generation by photosynthesis. Consequently, oxygen was a relatively recent addition to our atmosphere, beginning to accumulate only 2.5 billion years ago after plant life with sufficient photosynthetic capacity populated the planet.
The story of oxygen as a therapeutic agent for patients with chronic lung disease mirrors its dual planetary roles, both as an essential molecule in support of life and an aggressive oxidizer of other molecules that can result in the degradation of biological tissues. The duality of assisting patients with hypoxia and at the same time potentially causing pulmonary injury has complicated clinicians' willingness to apply long-term oxygen therapy (LTOT) in clinical practice. This review highlights the milestones in our understanding of the safe use of oxygen for patients with lung disease, and identifies some of the limits to our knowledge.
Discovery
The laboratory discovery of oxygen occurred in 1771, when Carl Wilhelm Scheele, a German-Swedish pharmaceutical chemist, generated what he called “fire air” by heating mercuric oxide, silver carbonate, magnesium nitrate, and other nitrate salts.2 Isaac Asimov, the American writer of science and science fiction books, called Scheele “hard luck Scheele,”3 because he was the first to discover oxygen and a number of other elements, including molybdenum, tungsten, barium, hydrogen, and chlorine, but credit went to others. Scheele had communicated his oxygen discoveries by letter to Antoine Lavoisier in 1774, but did not document his discovery until 1775, when he sent to a publisher his Chemical Treatise on Air and Fire, which was not published until 1777. His hard luck continued when he died prematurely from mercury poisoning that resulted from the heating of mercuric oxides for the generation of oxygen.
For many years the discovery of oxygen was incorrectly attributed to Joseph Priestley, an 18th-century English theologian with a political dissenter's inclination, natural philosopher, chemist, and educator, who heated red mercuric oxide and isolated oxygen as a colorless gas causing a candle to burn more brightly. He was “first to press,” having published his generation of oxygen in 1774, 3 years after Scheele's discovery. Priestley, however, never understood the implications of his own work. He used his observations to argue for the phlogiston theory of gases and against atomic theory, which was emerging at the time. Priestley had other controversial opinions on a number of political and theological issues, which aroused suspicion and resulted in a mob burning his home and church and his flight from England to central Pennsylvania for the final years of his life.
Although not the independent discoverer of oxygen, as he claimed, Antoine Lavoisier is recognized for advancing scientific knowledge of oxygen's chemical nature and role in normal respiration. His 1774 communications with both Priestley and Scheele allowed him in 1775 to repeat their experiments using more sophisticated laboratory equipment. He named the odorless gas “oxygen” based on his belief that it was essential for all acids. He proposed the role of oxygen in oxidizing metals and in respiration, demonstrating that it was taken up by the body during inhalation to allow slow combustion of organic substrates and that carbon dioxide was exhaled as a by-product. He proved that oxygen was a chemical element, which discredited the phlogiston theory. And he proposed that the composition of air contained oxygen (“vital air”) and nitrogen (“azote” or “lifeless air”) in his 1777 book, Mémoire Sur la Combustion en General (On Combustion in General). Like Scheele and Priestley before him, his life followed a difficult course; he was sent to the guillotine during the French revolution, when it was discovered that royal funds supported his laboratory.
Application of Oxygen in Medicine
The potential value of oxygen for patients with respiratory conditions was quickly recognized after its discovery. Thomas Beddoes, considered the father of respiratory therapy, worked with the inventor James Watt to generate oxygen and other gases, and opened a Pneumatic Institute in Bristol, England, in 1798, using oxygen and nitrous oxide to treat asthma, congestive heart failure, and other ailments.4 The institute closed after 3 years because of a typhus epidemic that consumed England's health resources, but oxygen remained available at apothecaries during the 18th and early 19th centuries, through generation by electrolysis.4 The first cylinders for storing oxygen were developed in 1868,5 which allowed its use in general anesthesia. By 1885, George Holtzapple used oxygen to manage a young patient with pneumonia, and established its role in acute care.6
The 20th century saw the dawn of oxygen use in clinical medicine and a rapid succession of discoveries of its physiologic effects and technological advances that allowed its clinical application. Haldane's expedition to Pike's Peak in 1911 generated the first descriptions of the effects of hypoxia and served as the foundation for his commonly quoted observation, “Anoxaemia not only stops the machine but wrecks the machinery.”7 Haldane subsequently described the Haldane effect, perfected a method for measuring oxygen content in blood, and did experiments on hyperbaric oxygen exposure. Other legendary scientists who fostered our modern understanding of oxygen in clinical medicine include Christian Bohr, Karl Hasselbalch, Joseph Barcroft, August Krogh, John Priestley, Yandell Henderson, and Herman Rahn.4
But effective use of oxygen in clinical practice also required more pragmatic advances. In 1907, Arbuthnot Lane devised rubber tubing that served as a nasal catheter for oxygen administration, and Haldane developed designs for modern-day oxygen masks. The oxygen tent was invented in the 1920s by Leonard Hill and constructed out of canvas with slots cut for patient access but no means of ventilation.8 Alvan Barach (Fig. 1) modified the tent using ice chunks for cooling and soda lime to absorb exhaled carbon dioxide, which allowed closed tent systems.9 Barach went on to perfect other oxygen delivery systems and became the first to report in the modern era the use of oxygen in support of hospitalized patients with pneumonia.10 Both Barach and Haldane developed “meter masks” with valves that diluted oxygen with room air, thereby allowing the adjustment of delivery oxygen concentrations. Barach also developed hoods to provide patients with constant positive airway pressure.

Dr Alvan Barach (1895–1977) introduced oxygen therapy to the United States and refined its application through a series of pioneering innovations, books, and journal publications. His work included design of oxygen delivery devices, application of constant pressure breathing, and popularization of aerosol therapy. (From Reference 9, with permission.)
Barach laid the foundation for our use of LTOT for chronic lung disease. In 1936 he noted that “Oxygen therapy in suitable cases relieves difficult breathing, restores strength, and helps reduce the swelling of the patient's legs and back”.11 He went on to design and use the first portable oxygen devices for patients with emphysema. In the 1950s he used transfilled oxygen bottles for ambulatory patients with exertional dyspnea.12,13 During the same period, Coats and Gilson14 and Pierce15 used oxygen in small, portable, compressed gas cylinders, noting subjective improvement in symptoms in patients with lung disease.
Early Scientific Evidence of Oxygen Benefits in Chronic Lung Disease
LTOT, however, had only marginal data on outcomes during the first years of its use to justify its expense and support its safety. Its broad application was slowed because of concerns about risks of CO2 narcosis. In 1966, the Veterans Administration cooperative study of the course and outcomes of patients with COPD reported the natural history of COPD and factors associated with a poor survival, one of which was hypoxia.16 Concurrently, Thomas Petty (Fig. 2) at the University of Colorado was gaining experience with a newly available liquid oxygen transfilling system, and began investigating its value for patients with advanced COPD. In 1967, he and his colleagues reported 6 patients with severe emphysema, pulmonary hypertension, and secondary polycythemia who were stabilized for one month in an in-patient setting and underwent right heart catheterization.17 In the second month they were treated with oxygen to maintain PaO2 values in the 60–70 mm Hg range. Repeat catheterization demonstrated that 3 patients had decreased mean resting pulmonary artery pressures, and 4 of the 5 with data available for their baseline red cell mass demonstrated decreased polycythemia. Patients also reported subjective improvements in exercise capacity, global sense of well-being, and their ability to engage in activities of daily living. Shortly thereafter, a study from Birmingham, England, confirmed similar benefits in reducing pulmonary hypertension and polycythemia for 6 patients with advanced COPD and chronic hypoxia treated with oxygen therapy.18 In 1968 Petty and Finigan reported an additional 20 COPD patients who benefited from oxygen therapy.19 Petty's group also emphasized that hypercapnia rarely occurred in 175 pulmonary rehabilitation patients treated with oxygen and subsequently introduced the concept of controlled oxygen delivery.20

Dr Thomas Petty (1932–2010) was a junior faculty physician at the University of Colorado in 1965, when he was assigned on one particular day a routine task of unpacking newly arrived prototype equipment for ambulatory oxygen therapy. He developed a passion for oxygen therapy and “brazenly” went counter to conventional wisdom that oxygen was dangerous for patients with COPD. His early research established the safety and scientific basis for ambulatory oxygen therapy. He was a leading investigator in planning and conducting the Nocturnal Oxygen Therapy Trial. (Courtesy of American Association for Respiratory Care.)
But these studies still had not confirmed the survival benefit from oxygen suggested by the Veterans Administration cooperative study. In 1970, Neff and Petty reported their experience with 182 patients with COPD enrolled in a pulmonary rehabilitation, of whom 33 received continuous oxygen.21 They compared the survival rates of these subjects with those reported in the Veterans Administration cooperative study16 and observed improved survival with oxygen in those patients with cor pulmonale and heart disease, matched for age and severity of disease. A survival benefit was not observed in the absence of heart failure. Although an uncontrolled trial, the large differences in mortality of 28% versus 62% in patients with cor pulmonale treated with and without oxygen stimulated interest in ambulatory oxygen therapy for its potential survival effect.
Groups then began to focus on the duration of oxygen therapy necessary to improve clinical outcomes. Stark et al demonstrated in 1972 that as little as 12–15 hours of oxygen a day improved hemodynamics as effectively as 24 hours of oxygen use.22 These findings created the ethical equipoise to propose multicenter trials to test the effects of duration of oxygen therapy on patient outcomes.
Multicenter Trials of Long-Term Oxygen Therapy
In 1974, the Surgarloaf conference on the Scientific Basis of Respiratory Therapy sponsored by the National Heart, Lung, and Blood Institute of the National Institutes of Health convened experts on chronic lung disease and respiratory therapy to review the evidence for benefit from oxygen therapy. The attendees identified the need for a prospective randomized trial designed to establish benefit and determine the necessary duration of oxygen administration each day to maximize clinical benefit.23 The conference recommendations spawned the prospective randomized Nocturnal Oxygen Therapy Trial (NOTT) that randomized patients to nocturnal oxygen (goal of 12 h) versus continuous (goal of 24 h) ambulatory oxygen to determine effects on survival and hemodynamic outcomes.24 The study enrolled patients in Chicago, Denver, Detroit, Los Angeles, San Diego, and Winnipeg, with a clinical diagnosis of emphysema, with or without chronic bronchitis, and either PaO2 at rest breathing room air ≤ 55 mg Hg during a 3-week steady state period, or PaO2 ≤ 59 mm Hg with electrocardiographic evidence of right ventricular hypertrophy, clinically determined right heart failure, or a hematocrit > 55% (Table 1).
Comparison of the Nocturnal Oxygen Treatment Trial (NOTT) and the Medical Research Council (MRC) Trials
In 1980, the NOTT reported the results of 203 patients with a mean of 19.3 months follow-up. Use of continuous oxygen (17.1 ± 4.8 h of oxygen use) conferred significant benefit, with a relative risk of death of 1.94 (1.17–3.24) for the nocturnal oxygen group (12.0 ± 2.5 h of oxygen use).25 The mortality differences between the continuous and nocturnal oxygen groups at 12 months and 24 months were 11.9% versus 20.6%, and 22.4% versus 40.8%, respectively. Continuous oxygen improved pulmonary vascular resistance and decreased the severity of polycythemia. None of the subjects with preexisting pulmonary hypertension, however, normalized their pulmonary vascular resistance. No differences were noted between groups in arterial blood gases, FEV1, lung volumes, maximum work attained, mean pulmonary artery pressures, or cardiac index.
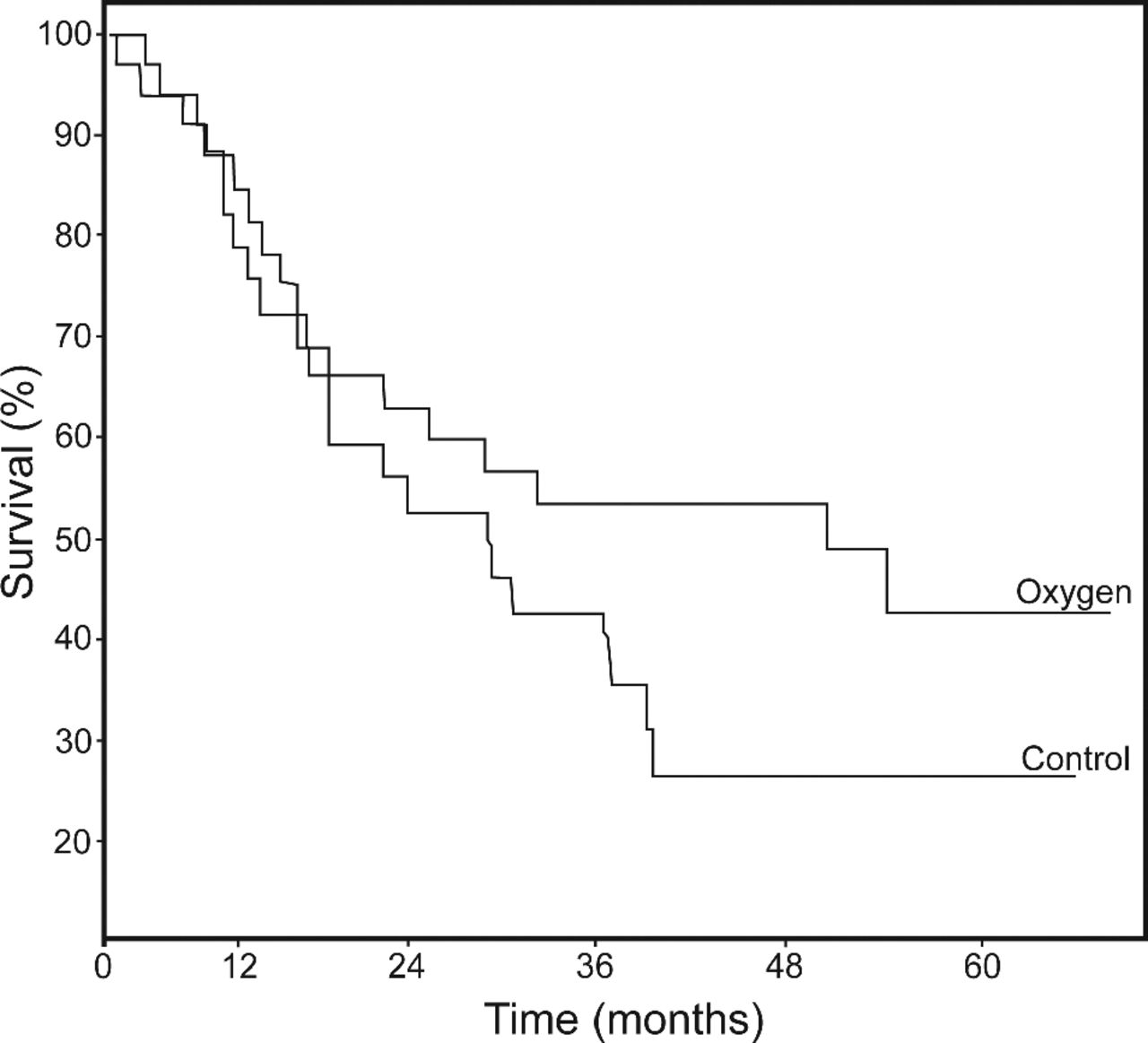
In 1981, the Medical Research Council (MRC) in the United Kingdom reported the results of a long-term oxygen trial that differed from the NOTT in comparing 15 hours of oxygen, which included nocturnal use, with no supplementary oxygen therapy (see Table 1).25 The trial enrolled 87 patients with COPD (chronic bronchitis or emphysema) who had irreversible airways obstruction, severe arterial hypoxemia, carbon dioxide retention, and mild pulmonary hypertension. The study demonstrated a survival advantage at 3 years and beyond, with a mortality of 45.2% and 66.7% for the oxygen treated and control groups, respectively (Fig. 3). Among secondary outcomes, no benefit was noted from supplemental oxygen in days spent working, days spent in the hospital for COPD exacerbations, polycythemia, or pulmonary hemodynamics. The mortality advantage, however, appeared greater in the subgroups with the highest PaCO2 and red cell mass values at baseline.
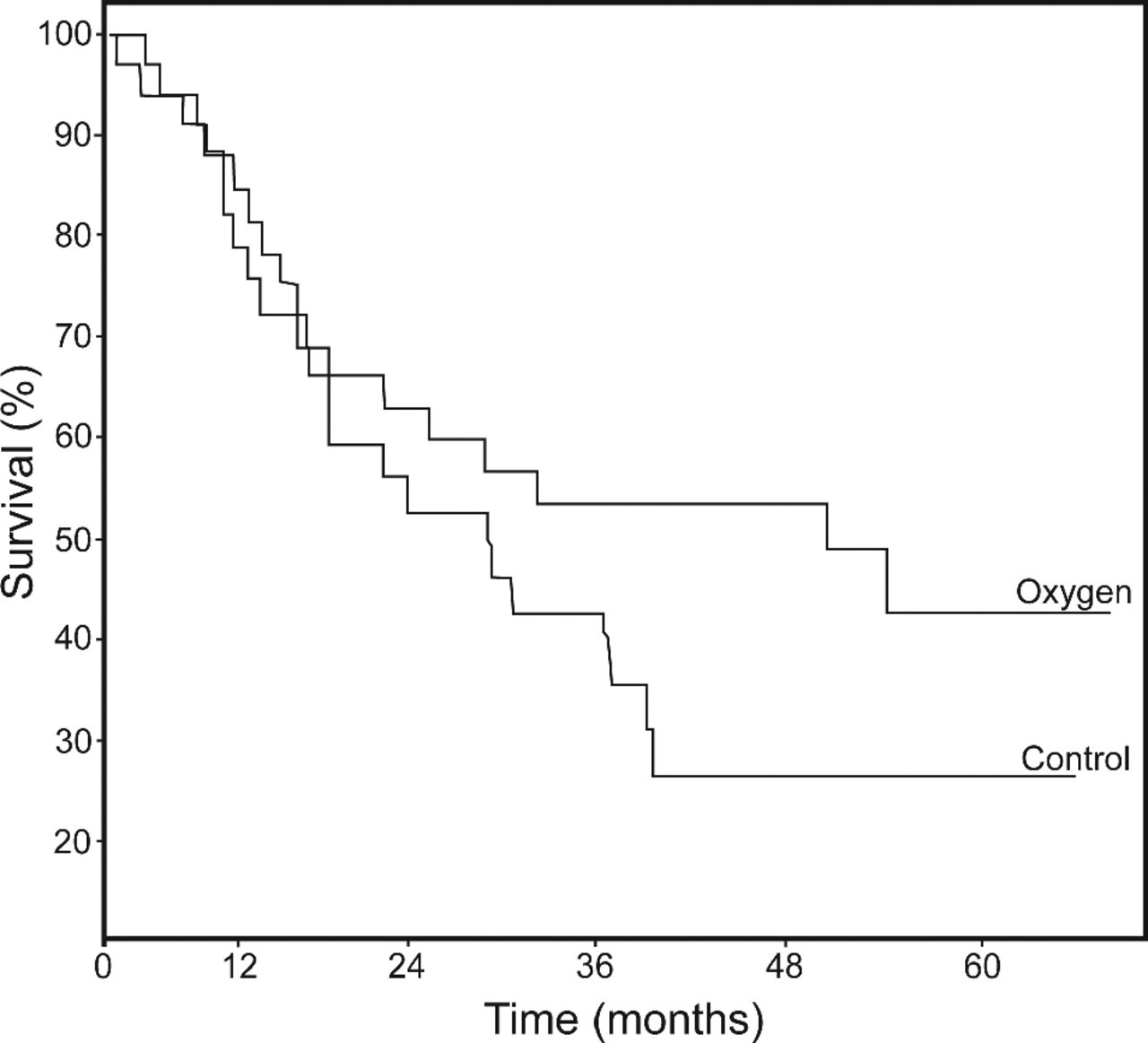
Mortality in male patients enrolled in the Medical Research Council oxygen trial. (From Reference 25, with permission.)
Petty proposed that the demographic, physiological, and clinical features of patients enrolled in both the NOTT and MRC studies were sufficiently similar to allow collective analysis of the survival data.26 When analyzed in this way, an oxygen dose response was noted, with poorest survival in the group not treated with oxygen from the MRC study, intermediate survival in the 12–15 hour oxygen groups combined from the NOTT and MRC studies, and the best survival in the continuous oxygen group reported in the NOTT study (Fig. 4).27 Subsequent uncontrolled trials of ambulatory oxygen therapy have generally produced survival results consistent with the dose response curves noted in the combined NOTT and MRC trials.28–33 Based on the original observations from the NOTT and MRC trials, LTOT became recognized as one of the few available therapeutic interventions that improve survival in patients with advanced COPD, which still is the primary justification for its use in COPD. These studies established our modern-day criteria for payment for oxygen therapy. They also generated support for supplemental oxygen for hypoxic patients with other chronic pulmonary conditions, even though these conditions were not included in the NOTT or MRC trials.
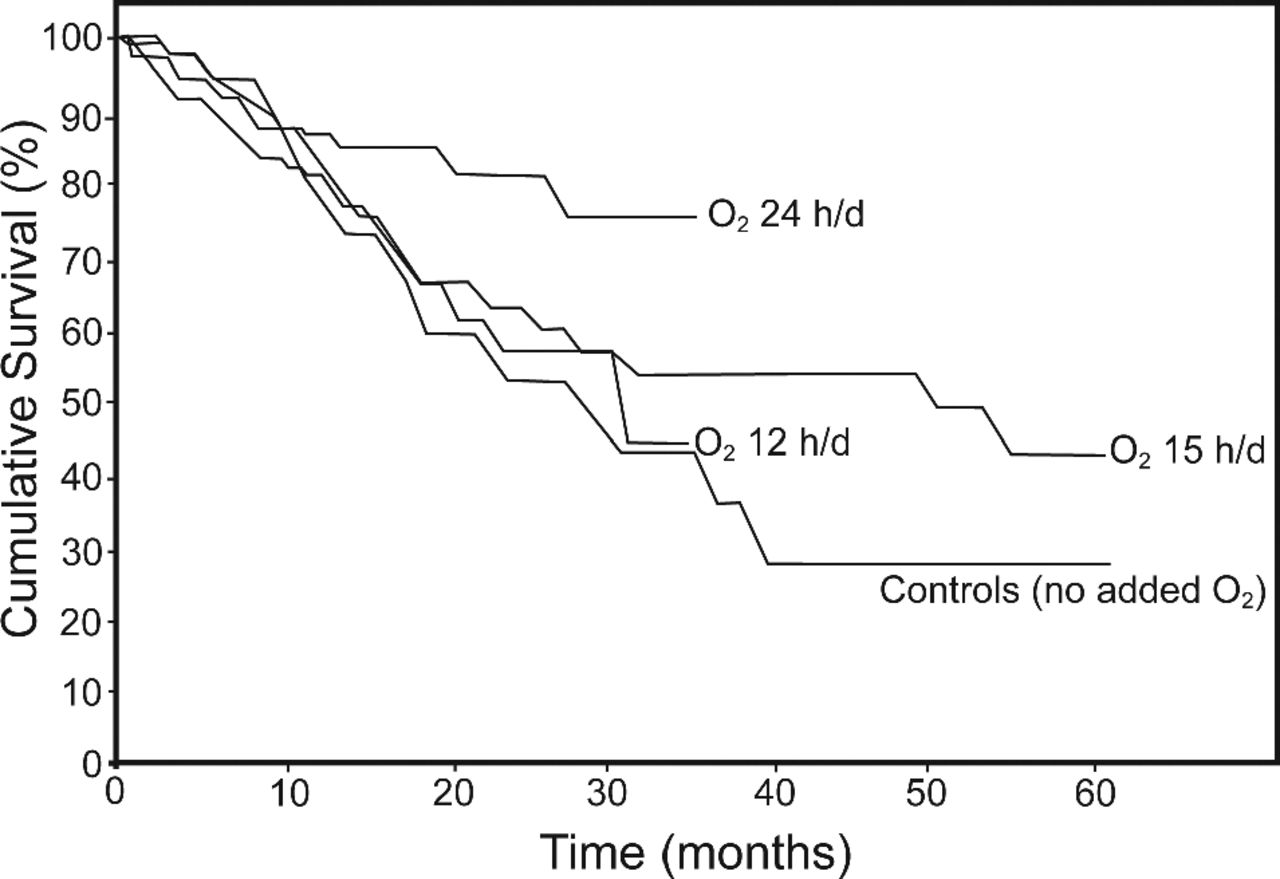
Overlapped survival curves from the Medical Research Council oxygen trial and the Nocturnal Oxygen Treatment Trial study, showing a dose-response curve to the duration of oxygen administration. (From Reference 27, with permission.)
Limitations of Knowledge
Although the NOTT and MRC studies were foundational in establishing a survival benefit of supplemental oxygen for patients with advanced COPD, many gaps remain in our understanding of the role of LTOT for patients with COPD and other forms of chronic lung disease (Table 2). Some of these gaps result from limitations of the NOTT and MRC data (see Table 1).34 These trials were not entirely comparable, in that patients in the MRC study continued to smoke, but no data were provided regarding the impact of smoking on measured outcomes; data on smoking rates were not provided in the NOTT study report. Patients in the MRC study also had more severe resting hypercapnia and pulmonary hypertension. And, finally, the MRC study noted no effect of oxygen therapy on physiologic variables, in contrast to the NOTT study, which observed improved pulmonary vascular resistance and hematocrit. The NOTT study, however, did not observe a causal relationship between these physiologic variables and survival.
Persistent Research Questions Regarding Long-Term Oxygen Therapy
Also of note, our complete understanding of the benefits of LTOT on survival and the justification for billions of dollars spent on oxygen therapy rest largely on the NOTT and MRC trials and a handful of other randomized controlled trials performed during the last 30 years, that enrolled a total of 501 subjects.18,24,35,36 These and other studies29,37,38 have demonstrated secular trends in COPD outcomes, with the better survival noted in more recent studies (Fig. 5).39 Questions consequently remain regarding the indications for oxygen therapy, considering the heterogeneity of COPD, and other therapeutic interventions for COPD that have become available since the MRC trial and NOTT.40 Recent analyses directed at these limitations34,40–42 coincide with the recently launched multicenter National Heart, Lung, and Blood Institute trial (the Long-Term Oxygen Treatment Trial [LOTT]), that will address the use of supplemental oxygen for patients with COPD and moderate hypoxemia at rest or with desaturation only with exercise.43 The remainder of this review highlights some of the important open questions that remain regarding LTOT.
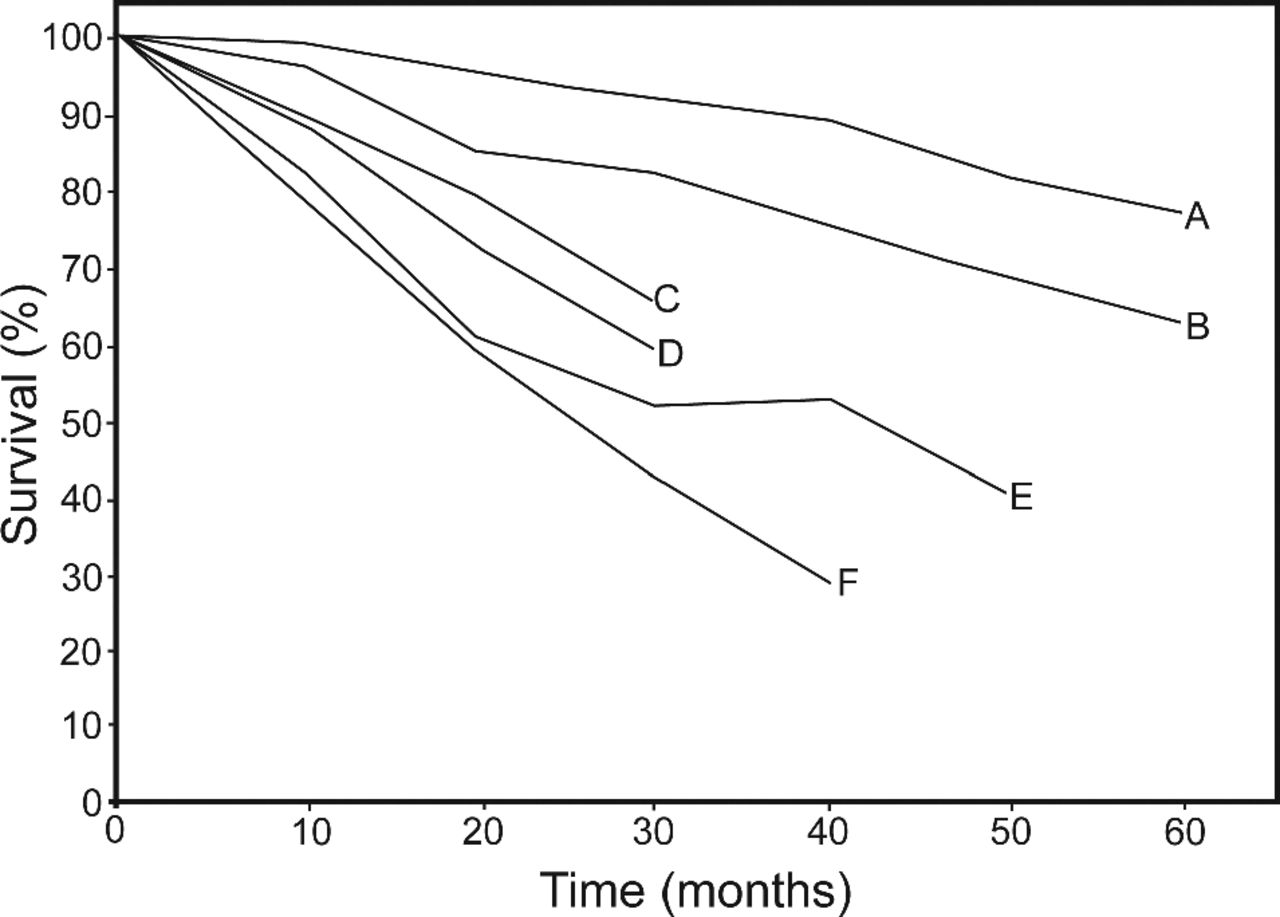
Survival of subjects enrolled in long-term oxygen therapy trials during a 19-year period. Note the trend toward improved survival in the most recent trials.24,25,29,37,38 A: Carrera et al 1999.38 B: Cooper et al 1987.37 C: Nocturnal Oxygen Therapy Trial group 1980.24 D: Strom 1983.29 E: Medical Research Council25 (with oxygen). F: Medical Research Council25 (without oxygen). (From Reference 39, with permission.)
Oxygen Effects on Brain Function
Krop and Block were the first to show improved brain function with oxygen therapy, compared with a placebo treatment with compressed air, in patients with advanced COPD.44 Noting this report, Petty et al made similar observations in a cohort of patients with COPD enrolled in pulmonary rehabilitation, and recommended in 1979 that “impaired neuropsychiatric function associated with COPD” represented an indication for LTOT.45 The NOTT had reported that impaired neuropsychiatric function was a predictor of benefit from continuous oxygen therapy and that cognitive function improved in both the nocturnal and continuous oxygen groups.24 A rationale for improved brain function with oxygen therapy was supported in 1982, when Grant and co-workers reported an inverse correlation between PaO2 and degree of cerebral dysfunction in COPD.46 A follow-up study of the NOTT noted comparable modest improvement in brain function in both the nocturnal and continuous oxygen groups 6 months after LTOT initiation, but no improvement in mood or emotional status.47 A more rigorous study of only 10 hypoxic patients with COPD, who were cognitively impaired, as compared with age-matched controls, demonstrated that 3 months of LTOT resulted in a trend toward improved neuropsychological function, cerebral blood flow velocity, and autonomic function, although the benefits were not statistically significant.48
Based on these reports, we know that hypoxia has a negative effect on cognitive performance.46,49,50 We also know that supplemental oxygen improves cerebral oxygenation and possibly brain function for patients who may not otherwise fulfill indications for LTOT.51 We do not know, however, how to measure and define neuropsychiatric impairment in a manner that ensures benefit from oxygen therapy, nor do we know how to confirm a beneficial effect, considering the co-administration of other therapies that produce a sense of improved well being.52
Benefits of LTOT for Pulmonary Hypertension in Severe COPD
The benefits of LTOT for managing pulmonary hypertension represent an important focus of investigation, because more than 20% of patients with advanced COPD have pulmonary hypertension, which is usually mild to moderate, but may be severe and poorly correlated with FEV1.34 The presence of pulmonary hypertension is associated with increased mortality, increased rates of exacerbations, and longer hospitalizations during exacerbations, independent of FEV1.53,54 Although the NOTT study demonstrated improvement in hemodynamic parameters, the duration of this benefit and its impact on survival remain uncertain.40 One study demonstrated that oxygen therapy > 15 h/d in hypoxic COPD patients reversed a worsening trend in severity of pulmonary hypertension,55 while another study demonstrated that 2 years of LTOT for 14–15 h/d was associated with only a small reduction in pulmonary pressures.33 The latter study, however, demonstrated that pulmonary hypertension returned to baseline values after 6 years of oxygen, although pressures remained stable subsequently, despite a worsening of FEV1 and hypoxia.55 The effects of acute administration of oxygen on pulmonary hemodynamics do not appear to predict the potential for LTOT to improve survival in COPD.56 Consequently, the effects of LTOT on the course of pulmonary hypertension in COPD remain poorly established. Also, data do not exist for other chronic respiratory conditions, other than COPD, that are associated with pulmonary hypertension.
Red Cell Mass
Patients with COPD in the NOTT study who had pulmonary hypertension and elevated hematocrits had the highest mortality and the greatest survival benefit with oxygen therapy.24 Patients with advanced COPD, however, also experience hypoxia-induced depression of erythropoiesis, which can result in low hematocrits, which, in retrospective studies, identified patients with poor survival.57,58 Data are needed, therefore, on the impact of oxygen therapy on erythropoietin production and survival across the spectrum of hematocrit abnormalities that occur in COPD.34
Oxygen Therapy in Mild to Moderate Hypoxia
The NOTT and MRC trials examined patients with severe hypoxia, as indicated by a PaO2 ≤ 55 mm Hg or evidence of cor pulmonale (56 ± 65 mm Hg). We have sparse data regarding the effects of LTOT for patients with mild to moderate resting hypoxia.41,59 Two small, randomized controlled trials with a total of 163 patients with mild to moderate hypoxemia noted no survival benefits during 1–3 years of follow-up.35,60 Neither study, however, used other clinical measures of COPD severity, nor assessed mortality risk as inclusion criteria, so the generalizability of these data are limited.42 Moreover, patients used oxygen only for 13.5 h/d; achieving benefit in the setting of less severe hypoxia may require oxygen administration for closer to 24 hours a day, considering that being off of oxygen therapy for only 3 hours is sufficient to cause acute worsening of pulmonary hypertension.40
The appropriate end points for measuring oxygen benefit in this patient group are uncertain. Survival may not be appropriate or even feasible to study because of the large number of subjects required. No studies exist regarding the impact of LTOT for these patients, in terms of decreasing exacerbations, improving exercise tolerance, enhancing quality of life, or reversing neuropsychologic dysfunction.40 Multiple clinical characteristics may also need to be identified that serve as indications of LTOT for subgroups of patients with mild to moderate hypoxemia, such as pulmonary hypertension, low body mass index, poor exercise capability, frequent exacerbations, or comorbid cardiac disease.40
Oxygen Benefits During Exercise
A subgroup of patients with COPD experience oxygen desaturation only during exercise as a result of ventilation/perfusion mismatching, diffusion limitations, shunting, and reduced oxygen content of mixed venous blood.61 Only a few small studies suggest that arterial oxygen desaturation limited to exercise is associated with decreased survival.62–67 The National Emphysema Treatment Trial (NETT), however, showed, in a retrospective analysis of the study data, no differences in survival among subjects with exertional desaturation and resting normoxemia who were treated with or without oxygen in a nonrandomized manner.68 On the other hand, the NETT did report that exercise-related hypoxia was associated with a poor prognosis.68 Consequently, the rationale for ambulatory oxygen in patients with exercise-induced desaturation is not based on survival benefits but on the concept that desaturation may hinder exercise, promote deconditioning, and degrade quality of life.
Oxygen may improve endurance by several potential effects.69 An increased PaO2 directly inhibits carotid body stimulation,70 thereby decreasing breathing frequency, prolonging the expiratory phase, and relieving hyperinflation associated with exercise in COPD both during exertion71,72 and in the recovery phase of exercise.73 Increased arterial oxygen content improves muscle oxygenation, thereby decreasing lactic acid production and carotid body stimulation. And, finally, improved oxygenation can dilate pulmonary vasculature by relieving hypoxic vasoconstriction74 and improve cardiac output and delivery of oxygen to exercising muscles.75
Early studies in the 1970s with ambulatory supplemental oxygen suggested that patients using portable liquid oxygen systems, as compared with liquid air, were more comfortable during exercise and could walk longer distances.76–78 More recent studies in patients with exercise-induced desaturation report improved ventilatory function, breathlessness, and exercise endurance with the acute administration of oxygen.69,70,79–87 These studies, however, were short-term and applied oxygen as an acute intervention. No long-term follow-up studies exist. A recent systematic review found inconclusive results for benefit in exercise tolerance in COPD patients treated with oxygen.88
Only 6 small, randomized controlled trials have assessed the effects of supplemental oxygen on exercise training and performance for patients with or without exertional desaturation who were undergoing pulmonary rehabilitation.80,89–93 The results of these studies have been inconsistent, but no clear beneficial effect emerges.94 Moreover, we do not have data on the interaction between supplemental oxygen and other supportive adjuncts, such as noninvasive ventilation, on the physiological adaptations to exercise in this patient population,69 nor do we have knowledge of the effects of oxygen during exercise for patients with different COPD phenotypes.94 Moreover, a recent randomized controlled trial of oxygen provided for 12 weeks to 143 COPD patients during activities of daily living found no effect on functional status, health status, or dyspnea.95 No predictive factors, such as desaturation to less than 88% during exercise, predicted benefit for the subset of patients who did experience improved status.
Investigations in this field are limited by an absence of explicit definitions of exertion-related hypoxia and standardized exercise protocols to demonstrate its presence.41 It remains unclear whether continuous oxygen therapy improves survival in normoxic patients with exercise desaturation, and the impact of ambulatory oxygen on other parameters remains to be firmly established. Whether each patients need to be individually tested to establish symptomatic improvement from oxygen therapy during exercise remains undefined.85
Transient Hypercapnia
Some patients with COPD develop transient hypercapnia during exacerbations and after exercise testing but do not otherwise have indications for LTOT.96 After recovery, hypercapnia resolves and PaO2 remains above 60 mm Hg. Although guidelines do not recommend oxygen therapy in these patients, a rationale exists if supplemental oxygen could delay respiratory muscle fatigue, improve diaphragmatic work capacity, and prevent hypercapnia.97 The NOTT suggested that stable hypercapnic patients with COPD may benefit from LTOT, in that survival benefit was observed in patients with PaCO2 levels above but not below 43 mm Hg.24 At least one study demonstrates that LTOT stops the decline of endurance time and reduces exertional dyspnea after one year, compared to control normoxic patients with COPD and reversible hypercapnia.60
Health-Related Quality of Life
Most patients with COPD report that their disease limits what they can do,98 with resulting decreased quality of life.99 The benefits of LTOT on health-related quality of life (HRQOL) were not addressed in the MRC trial.25 The NOTT did assess HRQOL,24 but it used the Sickness Impact Profile, which is a general health rather than a respiratory specific measure. Nevertheless, the NOTT demonstrated HRQOL improvement after 6 months of treatment in both the continuous oxygen and nocturnal oxygen treatment arms. The investigators did not, however, stratify their analysis for the continuous oxygen group alone, and they did not have an untreated control group to assess the impact of oxygen therapy on HRQOL measures, as compared with no oxygen.34 In the absence of more extensive data, concern exists that LTOT may have potential negative effects on HRQOL, because of lack of mobility or because of perceived social stigma.
The ability to do randomized controlled trials on HRQOL effects of oxygen therapy is limited by ethical issues that prevent inclusion of a control placebo group. Okubadejo and colleagues, using a before-after design, reported no effects on HRQOL among patients with severe COPD who received oxygen therapy with a concentrator for 6 months.100 Andersson and colleagues found improved HRQOL in subjects treated with liquid oxygen systems, but decreased HRQOL in those treated with small portable oxygen cylinders.101 Another study using short-term ambulatory oxygen noted improved HRQOL in COPD patients who did not have chronic hypoxia but who did have exertional desaturation to ≤ 88%.102 Benefits, however, could not be predicted by baseline characteristics or acute response to oxygen administration. Moreover, a substantial number of patients declined LTOT, despite measured improvements in HRQOL.
Nocturnal Desaturation
Patients with COPD without obstructive sleep apnea can develop desaturation during sleep, even when oxygenation is normal while awake,103–107 which has been associated with increased mortality, as compared with patients who do not have nocturnal desaturation.108 Also, elevated mean pulmonary arterial pressures are noted in COPD patients with nocturnal oxygen desaturation.109 Administration of nocturnal oxygen for these patients can prevent desaturation during sleep.110
Benefits from achieving normoxemia during sleep, however, are poorly defined. Limited and contradictory data exist on improving sleep quality,104,111 hemodynamic effects, and mortality.35,36,108 Challenges to research in this field include no definition of the threshold and duration of nocturnal hypoxemia that defines isolated nocturnal desaturation. But, based on existing data, it is unknown whether nocturnal oxygen therapy improves survival or other clinically important end points in patients with COPD and isolated nocturnal oxygen desaturation.34,41
Oxygen Delivery
Major progress has occurred in the design of oxygen delivery devices, but additional advances are needed. Studies are required to develop smart systems that deliver oxygen at appropriate times and that consider the relationship between demand and supply in varying life circumstances.40 Application of accelerometers or arterial oxygen sensors presents promise. In broader terms, we are not certain that 24 hours a day is better than 18 hours, which is important because of challenges with patient adherence.24,35,112 Future research is needed to develop more tolerable oxygen delivery devices and to test their effectiveness in improving patient outcomes.
Oxygen for Chronic Lung Diseases Other Than COPD
Although almost the entirety of evidence for benefit from LTOT derives from studies of patients with COPD, this evidence has justified LTOT use for other chronic lung diseases associated with hypoxia. We do not know, however, if LTOT provides similar benefits to patients with conditions such as pulmonary fibrosis, kyphoscoliosis, or cystic fibrosis, which may have different mechanisms for hypoxia and dyspnea. Patients with interstitial lung disease, for instance, develop rapid and shallow breathing at low lung volumes during exercise, rather than at higher lung volumes with air trapping, as characterized by COPD.113 Studies have demonstrated improved endurance times with high flow oxygen for patients with a variety of interstitial lung diseases, but oxygen was administrated acutely and low flow oxygen was not assessed.114,115 One retrospective study reported improved exertional capabilities, oxygen saturations, and dyspnea scores among 52 patients with interstitial lung disease, but quality of life was not assessed.116 In contrast to COPD, impaired gas exchange and circulatory limits represent the major impediments during exercise in patients with interstitial lung disease, in contrast to abnormal ventilatory mechanics experience with COPD.117,118 LTOT may have different effects and different indications for use in these different pathophysiologic settings. Moreover, the effects of oxygen therapy on HRQOL measures in these conditions have been rarely investigated.119
LTOT and Comorbidities
COPD has increasingly been recognized as a multisystem condition with clinical expression beyond the lungs.120 Comorbidities affect prognosis and the clinical course of patients with COPD across all severity classes of the disease.121–124 These comorbidities, however, have not been considered in studies of LTOT. Because the mechanisms for hypoxemia in COPD complicated by congestive heart failure differ from those in patients with COPD alone,125 differing effects of oxygen therapy in these 2 settings may be inferred. Investigations are needed to assess the LTOT on all-cause mortality in patients with various constellations of comorbidities and COPD phenotypes.34 To do these studies, standardized methods for identifying and grading COPD comorbidities are needed yet do not exist today.
Summary
The history of oxygen from discovery to application in the care of patients with chronic lung disease represents a storied journey marked by contributions from many bold scientists, brazen practicing physicians, and pioneering clinical investigators. The fundamental importance of oxygen to life on this planet ensures its place in the care of patients with respiratory disorders. Existing survival data derive largely from the 1970s and 1980s, from a very select and limited number of study subjects who do not represent the heterogeneity of COPD phenotypes or the diversity of other chronic respiratory conditions for which oxygen is now used.34 Although the indications for LTOT have been refined by consensus conferences over the years,126,127 limitations on our understanding of the nature of oxygen benefits, how to measure those benefits, and more nuanced indications for its use in a variety of patient populations require even greater investigative efforts in the future.
Discussion
Pierson:*
I'll take the prerogative of the first response. As you were giving that splendid review, John, I couldn't help thinking about the technological developments that have occurred during the lifetime of these conferences, and how they have facilitated the clinical history and development of oxygen. The development that occurred to me most was pulse oximetry. The NOTT1 and MRC2 studies were based on arterial blood gas analysis, which was the gold standard for assessing oxygenation in COPD with respect to LTOT. In 1981, when John West went to Mount Everest,3,4 he lugged with him a bulky, heavy Hewlett-Packard ear oximeter, which was the available noninvasive assessment of oxygenation at that time. Within the next several years in the United States there was an explosion of pulse oximetry technology, and the devices became smaller, less expensive, and widely available. By the time the first Medicare LTOT guidelines were released in 1985, they included O2 saturation from pulse oximetry as an alternative to arterial PO2 from blood gas analysis.5 This was the only place in the world at that time where pulse oximetry was officially acknowledged for the clinical determination of hypoxemia in COPD, and it initiated a whole period of incredible technological development. We're going to hear presentations on new technology for home and ambulatory O2, for delivering high-flow nasal oxygen, and other advances, but it struck me how profound the impact of pulse oximetry has been on every aspect of oxygen: the topic of this conference.
Heffner:
I think that's a good observation that probably also relates to many of the studies that examined the impact of O2 therapy. For instance, the study by Levine and Petty6 of their original 6 patients treated with oxygen, first, they stabilized the patients, and after they had stabilized them, they later ended up excluding many from the study because they were no longer hypoxic. Which meant that we really had 2 sets of blood gases at 2 points in time—snapshots of these individuals rather than a continuous profile. Patient selection may have been different had we had continuous, or at least more frequent, measures of oxygenation, such as by oximetry. If such studies enrolled patients based on oximetry, different study populations may have resulted in different observations regarding continuous O2 therapy. Any other comments or thoughts?
Jeffrey Ward:
Just to finish on Dave's comments, it was interesting that the discovery and invention of pulse oximetry was serendipitous. In the early 1970s Takuo Aoyagi was experimenting with ear oximetry for cardiogreen dye densitometry, to measure cardiac output noninvasively. He developed a method to cancel pulsatile variations at infrared wavelengths (900 nm), where cardiogreen is transparent, from the 630 nm red signal. However, he noticed that the technique resulted in unsteady signals. The problem was oxygen desaturation. As saturation dropped, the infrared increased and red light decreased. Aoyagi's static turned out to be the signal that became of interest to all of us. In addition, from the corporate perspective, he didn't get much money out of the discovery, as his company, Nihon Kohden, neither developed a market for the their initial ear oximeter in Japan nor marketed it abroad.7 Thirdly, the evidence for pulse oximetry actually making a big difference in patient outcomes is pretty thin.8–10
Acknowledgments
This article is dedicated to Alvan Barach, Thomas Petty, Thomas Neff, Louise Nett, and the other pioneers who ensured the delivery of oxygen to respiratory patients in need.
Footnotes
- Correspondence: John E Heffner MD, Providence Portland Medical Center, 5050 NE Hoyt Street, Suite 540, Portland, OR 97213. E-mail: john_heffner{at}mac.com.
Dr Heffner presented a version of this paper at the 50th Respiratory Care Journal Conference, “Oxygen,” held April 13–14, 2012, in San Francisco, California.
The author has disclosed no conflicts of interest.
↵* David J Pierson MD FAARC, Emeritus, Division of Pulmonary and Critical Care Medicine, Harborview Medical Center, University of Washington, Seattle, Washington.
- Copyright © 2013 by Daedalus Enterprises Inc.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.
- 31.
- 32.
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.
- 64.
- 65.
- 66.
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.
- 78.↵
- 79.↵
- 80.↵
- 81.
- 82.
- 83.
- 84.
- 85.↵
- 86.
- 87.↵
- 88.↵
- 89.↵
- 90.
- 91.
- 92.
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.
- 106.
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.↵
- 119.↵
- 120.↵
- 121.↵
- 122.
- 123.
- 124.↵
- 125.↵
- 126.↵
- 127.↵









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}