

Abstract
BACKGROUND: The purpose of this study was to compare the ability of 3 portable oxygen concentrators (POCs) to maintain SpO2 ≥ 90% during exercise in patients with chronic lung disease.
METHODS: Twenty-one subjects with chronic lung disease (18 with COPD, 3 with pulmonary fibrosis) and documented room air exertional SpO2 ≤ 85% performed four 6-min walk tests: a control walk using the subject's current oxygen system and prescribed exertional flow rate, and 1 walk with each of the 3 POCs (Eclipse 3, EverGo, and iGo) at their maximum pulse-dose setting.
RESULTS: SpO2 was significantly higher pre-walk and post-walk with the Eclipse 3, compared to the other POCs (all P < .01). The subjects also walked farther and maintained a mean SpO2 ≥ 90% with the Eclipse 3 (both P < .01), which delivers the largest oxygen bolus. The subjects indicated that they preferred the EverGo's physical characteristics, but that the Eclipse 3 responded best to their breathing. The iGo was rated less favorably than Eclipse 3 or EverGo.
CONCLUSIONS: The Eclipse 3 was best at meeting the subjects' clinical needs. POC users should be appropriately tested during all activities of daily living, to ensure adequate oxygenation. The healthcare provider should provide information and help to direct the subject toward the most clinically appropriate oxygen system, while being mindful of the patient's preferences and lifestyle. (Clinicaltrials.gov NCT01653730).
Introduction
Long-term oxygen therapy (LTOT) is indicated for patients with chronic lung disease, and is universally accepted for its effect on mortality in patients with COPD and persistent hypoxemia.1,2 Supplemental oxygen improves exercise performance, enhances exercise training, and reduces dyspnea.3,4
Patients with chronic lung disease using LTOT benefit from an active lifestyle, and portable oxygen systems are of particular interest to this patient population. The challenge for clinicians is in selecting the most appropriate portable oxygen system and meeting the patients' current and future clinical and physical needs.5–13 The 6th LTOT consensus conference recommended that physicians, patients, and home-medical-equipment providers effectively collaborate to ensure LTOT users have access to the most appropriate technologies for their clinical and lifestyle needs.14
Portable oxygen concentrators (POCs), whose only daily requirement for maintenance is access to electricity to re-charge the batteries, present an attractive option when compared to compressed gas and liquid oxygen systems. However, studies have shown that POCs do not always maintain adequate oxygenation during exercise,5,7,13 and bench studies have shown decreases in FIO2 in POCs as breathing frequency increases.9,12 These studies give reason for concern, since evidence suggests that maintaining SpO2 ≥ 90% offers a survival advantage.15
A small number of studies have examined how variations in the technical specifications between POCs affect clinical outcomes in exercising patients. Subramaniam et al10 compared 3 POCs during a 10 min treadmill test and found no statistical differences in SpO2 or walking distance. However, a second group did find a difference between 3 POCs during a treadmill test, concluding that higher oxygen delivery capacity was associated with improved exercise outcomes and oxygenation.5,13
In an attempt to reconcile the disparity in these results and to determine if POCs are capable of meeting patients' oxygen needs during exercise (SpO2 ≥ 90%), we chose to evaluate 3 POCs using a standardized 6-min walk test (6MWT) in patients with chronic lung disease with severe exertional oxygen desaturation. We also measured patients' personal POC preferences.
QUICK LOOK
Current knowledge
Supplemental oxygen during exercise reduces dyspnea and improves exercise performance in patients with hypoxemia due to chronic lung disease. Portable oxygen concentrators promote mobility, but their ability to reverse exercise-related hypoxemia is suspect.
What this paper contributes to our knowledge
The portable oxygen concentrator with the largest oxygen pulse-dose volume was best at meeting subjects' clinical needs. Home oxygen patients should be tested during all activities of daily living, including exercise, to ensure adequate oxygenation. Patients should be directed toward the most clinically appropriate portable oxygen system, but also consider patient preferences and lifestyle.
Methods
This study was approved by the Ottawa Hospital Research Ethics Board (2009845-01H). All subjects gave written informed consent before their screening assessment.
Study Design and Setting
A within-subject, repeated-measures design was used to compare 3 POCs during an exercise test. The subjects attended 2 sessions at the Respiratory Services, CANVent Program of the Ottawa Hospital Rehabilitation Centre. During the initial screening session, clinical characteristics were measured to determine the patient's eligibility for the study. Eligible patients then returned for a second session, where they completed 4 6MWTs: 1 with their usual portable oxygen source, and 1 with each of the 3 POCs.
6-Min Walk Test
The 6MWT is a reproducible, self paced, walk test, reflective of activities of daily living.16 A physiotherapist and a respiratory therapist conducted all of the walks using the American Thoracic Society 6MWT standards and script.17
Subjects
Oxygen dependent patients with an existing diagnosis of COPD or pulmonary fibrosis who had completed the pulmonary rehabilitation program at the Ottawa Hospital Rehabilitation Centre between January 30, 2008, and March 31, 2011, were invited to participate in the study. While the pathophysiology of pulmonary fibrosis is different than COPD, and the ability of POCs to maintain oxygenation during exercise may differ, this patient population also benefits from and partakes in an active lifestyle. They therefore need access to and/or guidance on the appropriateness of portable oxygen systems. For these reasons patients with pulmonary fibrosis were included in the study.
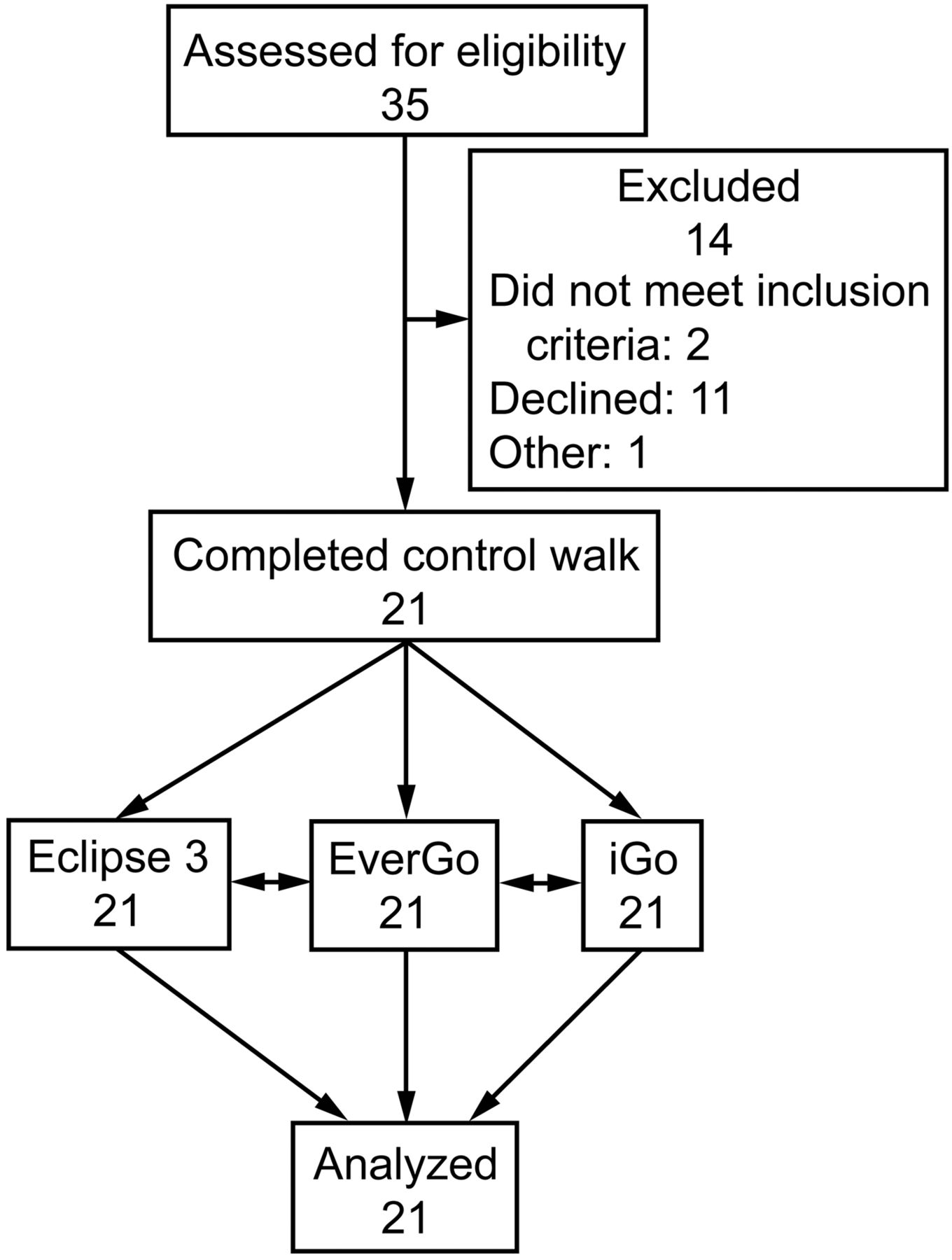
During the screening session, patients completed a 6MWT on room air to determine their eligibility for the remainder of the study. Patients who maintained SpO2 > 85% during the walk were excluded (Fig. 1).

Flow chart.
Equipment
We selected the 3 POCs with the highest oxygen production capabilities (mL/min) that were available in our region: EverGo (Respironics, Murrysville, Pennsylvania), iGo (DeVilbiss Healthcare, Summerset, Pennsylvania), and Eclipse 3 (Caire Medical, Ball Ground, Georgia). Technical specifications can be found in Table 1. We tested these POCs' ability to meet the subjects' oxygenation needs. Since POC pulse-dose settings are most frequently used by patients on LTOT, to conserve battery power, each unit was set at its maximum pulse-dose setting. For the control walk the subjects used their personal portable oxygen device, on the setting prescribed for paced exercise (Table 2).
Technical Specifications of the Tested Portable Oxygen Concentrators
Oxygen Systems, Pulse-Dose Settings, and Oxygen Flows by Number of Subjects
Screening Session
On the day of the screening assessment the subject's medical history was obtained and FEV1 and FVC were measured (CPFS/D, Medical Graphics, St Paul, Minnesota). The subject then performed a qualifying room air 6MWT while SpO2 was monitored.
POC Testing Session
Qualifying subjects returned to the clinic within 3 weeks for a second session. These subjects each performed 4 separate 6MWTs during this second session. Two walks were completed in the morning, followed by a minimum 2-hour lunch break, and then 2 walks in the afternoon. The first 6MWT was a control walk in which the subject used his or her usual oxygen system set at the prescribed exertional oxygen flow (maximum 4 L/min). The subject then performed a 6MWT with each of the 3 POCs, set at the unit's maximum pulse-dose setting. The Eclipse 3 was the only device with adjustable rise time and triggering sensitivity features. For all the subjects the sensitivity was set at “1” (most sensitive) and rise time set at “Fast.”
The order in which POCs were used was randomly assigned for each subject, using a sequence generator to minimize order effects. Subjects completed the walk using their usual mode of ambulation (eg, walker with basket). Each 6MWT was separated by a minimum 20-min rest period to allow their SpO2 to return to baseline, during which the subject used his or her own oxygen system at the prescribed resting setting. Subjects were placed on the assigned POC 10 min prior to the next walk. The therapist terminated a walk if the subject's SpO2 reached ≤ 85% for any length of time. Subjects also had the option to terminate a walk at any time, based on their own judgment of perceived exhaustion.
Outcome Measures
SpO2 was measured continuously during the walk, using a forehead probe (OxiMax Max-Fast, Covidien, Mansfield, Massachusetts) with headband, and an oximeter (OxiMax N-600 or N600x, Covidien, Mansfield, Massachusetts). Heart rate was monitored during the walk to ensure probe connectivity and to ensure subject safety, but is not reported. After each walk, oximetry data were downloaded to a computer (Profox Oximetry Software, Profox Associates, Escondido, California). SpO2 and dyspnea (as measured by the 10-point Borg dyspnea scale)18 were manually recorded before the start (pre-walk) and at the end (post-walk). Total distance walked and time spent with SpO2 ≥ 90% was recorded. Post-walk the subjects completed a self-administered questionnaire designed by the researchers to allow them to rate the POCs (Fig. 2).
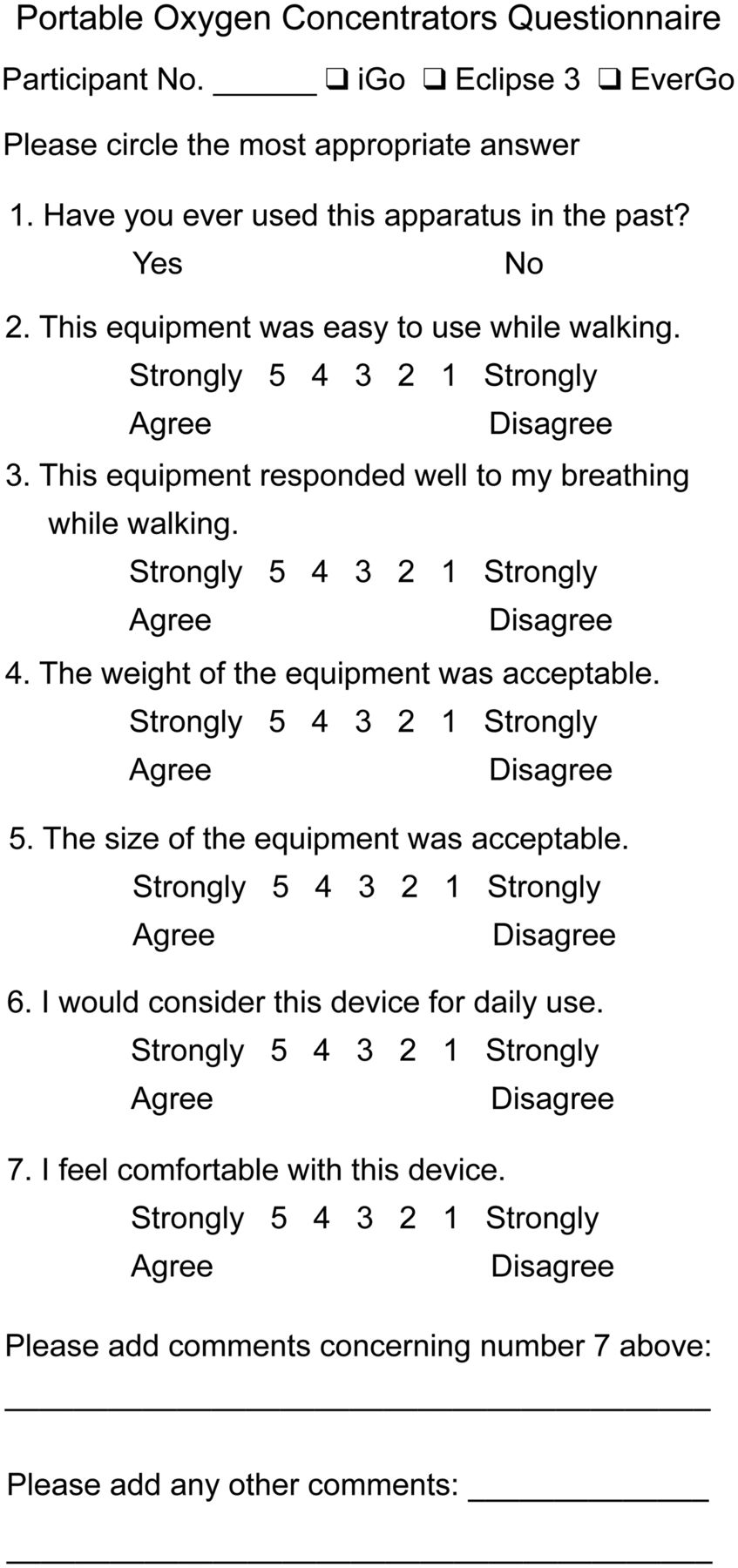
Self-administered questionnaire about portable oxygen concentrators.
Statistical Analysis
Pre-walk and post-walk SpO2 saturations and Borg scores were analyzed using repeated-measures analysis of variance with time point (pre-walk vs post-walk) and POC type as within-subject repeated factors. Pairwise post hoc comparisons applying Bonferonni corrections for multiple comparisons were done to further examine significant effects. A second repeated-measures analysis of variance was completed for outcomes measured only once (walk distance, time with SpO2 ≥ 90%) with POC type as the within-subject repeated factor. Questionnaire data were examined with descriptive analyses. All analyses were completed with statistics software (SPSS 18 or 19, SPSS, Chicago, Illinois).
Results
Subject Demographics and Baseline Characteristics
Of the 35 patients who completed the rehabilitation program and were oxygen dependent, 24 agreed to participate, 2 of whom failed to meet the SpO2 criteria during the screening room air 6MWT, and another was excluded due to poor SpO2 tracking, leaving 21 subjects in the analyses (12 females). The subjects had a mean ± SD age of 66.57 ± 8.36 y (range 53–82 y). Eighteen subjects were diagnosed with COPD, and 3 with pulmonary fibrosis. The mean percent-of-predicted FEV1 was 32.22 ± 11.67% in the subjects with COPD, and 61.0 ± 7.94% in the subjects with pulmonary fibrosis. The mean FEV1/FVC was 42.22 ± 16.35% in the subjects with COPD, and 85.67 ± 4.04% in the subjects with pulmonary fibrosis.
Fifteen subjects used a wheeled walker to carry the POCs, and 6 used the manufacturer provided POC wheeling device.
6-Min Walk Test Results
The 6MWT results and reasons for walk termination are presented in Table 3. Eighty-six percent of the subjects walked for the full 6 min using the Eclipse 3, as compared to 52% using either the iGo or the EverGo. One walk was terminated by the subject, during an EverGo trial; all other terminations were initiated by the therapist, due to oxygen desaturation.
6-Min Walk Test Results, and Reasons for Walk Termination
There was a significant interaction between POC type and the pre-walk versus post-walk SpO2 measurements (P = .006). Post hoc tests showed that SpO2 was higher pre-walk (P < .001) and was highest with the Eclipse 3 (P < .001 for all comparisons of Eclipse 3 to iGo and EverGo). The Eclipse 3 had higher mean SpO2 both pre-walk and post-walk, and the SpO2 decrease between pre-walk and post-walk was the smallest with Eclipse 3 (Fig. 3).

SpO2 before and after four 6-min walk tests: control (subject's usual portable oxygen system), with the iGo POC, with the Eclipse 3 POC, and with the EverGo POC. * Significant SpO2 difference between Eclipse 3 and EverGo or iGo.
The during-walk SpO2 of the 3 subjects with pulmonary fibrosis were within the distribution of all the subjects. With the Eclipse 3, 2 of the 3 subjects with pulmonary fibrosis maintained SpO2 ≥ 90% for the duration of the walk, and the 3rd subject maintained SpO2 > 85%. The subjects with pulmonary fibrosis did not maintain SpO2 > 85%, nor did 7 of the 18 subjects with COPD, with the iGo or EverGo.
While the mean Borg score was significantly higher post-walk than pre-walk (P < .001), there was no significant Borg score difference between the POCs (P = .20).
There was a significant difference between the POCs for time spent with SpO2 ≥ 90% (P < .001) and total distance walked (P = .001). Post hoc analyses indicated that the subjects walked farther with the Eclipse 3 (control P = .01, EverGo P = .009, iGo P = .008) and spent more time with SpO2 ≥ 90% (control P < .001, EverGo P < .001, iGo P = .001). The Eclipse 3 was the only POC to maintain a mean SpO2 ≥ 90% for the duration of the walk.
Questionnaire Responses
The subjects consistently gave neutral (3) or disagree (1 or 2) questionnaire responses for the iGo. The subjects rated the EverGo most favorably for the questions about the device's physical characteristics (86% of subjects rated EverGo 4 or 5 for each statement), whereas the Eclipse 3 received the most favorable response regarding the device's ability to respond to breathing (95% of subjects gave a rating of 4 or 5). The EverGo and the Eclipse 3 received comparable responses to the remaining statements, with ratings of 4 or 5 in 81% and 76% of the subjects for “easy to use while walking,” 50% and 48% for “felt comfortable with device,” and 52% and 43% for “would consider for future use” (Table 4).
Summary of Questionnaire Data
Discussion
This study compared the ability of 3 POCs to maintain adequate oxygenation during a 6MWT in a well defined group of subjects with chronic lung disease. Despite using the maximum pulse-dose setting for each device, the Eclipse 3 was the only POC to maintain a mean SpO2 ≥ 90% for the duration of the 6MWT, and showed significantly better performance on all outcome measures. The difference in walk distance between the Eclipse 3 and the other 2 POCs was also clinically important.19 Furthermore, the subjects rated the Eclipse 3 as the best to respond to their own spontaneous breathing patterns during exercise.
Although the Eclipse 3 and the iGo have the same high oxygen production capability (3,000 mL/min), they did not demonstrate equivalent performance. This is in contrast with the results found by McCoy et al,5,13 who concluded that having a POC with a greater oxygen production capacity improved SpO2 and exercise outcomes. Instead, we found that post-walk SpO2 and walk distance were more similar between the EverGo and the iGo than the Eclipse 3, despite the fact that the EverGo has a published oxygen production capability about one third that of the other 2 POCs (1,050 mL/min). Based on these POCs' technical specifications, we speculate that the most probable characteristic contributing to the performance differences was the O2 pulse-dose bolus volume. While the bolus volume ranges of the iGo and EverGo are similar, the Eclipse 3 is much larger (see Table 1). In line with results reported by Chatburn and Williams,9 we suggest that the larger O2 pulse bolus volume of the Eclipse 3 was an important contributing factor enabling it to better meet the subjects' oxygen needs during exercise.
In spite of the Eclipse 3's superior performance for meeting clinical needs, subjects rated the EverGo and the Eclipse 3 similarly when asked if they would use the device in the future. Clearly, the physical characteristics of the EverGo, as the lightest and smallest POC, were important to subjects. Clinicians should educate patients that the goal of supplementary oxygen is to satisfy blood oxyhemoglobin needs and that this should be the first consideration in selecting a POC. The current study tested 3 specific POC models, and, although the technology will change, the recommendations and principles for determining the best POC for patients will remain. It is important to consider not only production capability but also bolus volume when helping patients choose the right POC.
During the control 6MWT most of the subjects desaturated to unacceptable levels. It is clear that subjects' usual paced walking prescription and oxygen device were unable to meet the oxygen requirements of strenuous exercise. During rehabilitation, patients are instructed in how to pace themselves during exercise, in order to minimize oxygen desaturation. Clinicians should ensure that patients are aware of the limitations of their devices and have appropriate oxygen prescriptions for all activity levels. This study should raise awareness of POC variability and that clinicians should focus on clinical outcomes under conditions as close as possible to real life. Clinicians and patients should test any potential new device to ensure it meets their clinical needs during activities of daily living. Patients' preferences (ie, for lighter, smaller, or more convenient devices) should only be considered once potential devices have been demonstrated to meet their oxygen needs.
Limitations
We did not test whether these POCs met their advertised product specifications. Our interpretation therefore assumes that no product defects or anomalies were present. Further, although subjects with COPD and pulmonary fibrosis were included in the sample, there was an insufficient number of subjects with pulmonary fibrosis to do group analyses. Despite this, visual inspection of the data suggests that the subjects with pulmonary fibrosis had patterns of performance on the different POCs similar to the subjects with COPD. Future studies should aim to recruit more subjects with pulmonary fibrosis, to determine if their needs are different from subjects with COPD. Additionally, due to methodological constraints we did not measure breathing frequency, which might have affected these POCs' ability to meet subjects' oxygen needs. Future studies should measure breathing frequency during ambulation.
Inhaled medication use was also not specifically monitored. Although none of the subjects was observed taking rescue inhaled medication, the subjects were not always visible to the therapists conducting the testing, in particular during lunch breaks and between walks. Nevertheless, since the measurements were made within subjects, and the order in which the POCs were used was randomly assigned, it is unlikely that there would be an effect of bronchodilator use that would have affected any one POC more than another.
Finally, it should be recalled that this study involves selected subjects who desaturated to below 85% during a room air walk test, so our results do not preclude the possibility that any of the POC devices tested could provide adequate oxygenation for subjects who have lesser degrees of desaturation.
Conclusions
These findings suggest that subjects with chronic lung disease exhibit considerable improvement in their ability to maintain SpO2 when exercising with the Eclipse 3. We have shown that bolus size can be an important factor in determining the effectiveness of a POC, and healthcare professionals should be mindful of patients' current and future oxygen needs at all activity levels when guiding them in the selection of their own POC.
Acknowledgments
We thank the subjects who participated in this research; Paula Baxter RRT at the Ottawa Hospital Rehabilitation Centre, who assisted in coordinating the testing sessions; and Ronald Racette who assisted with the grant and ethics proposals.
Footnotes
- Correspondence: Carole J LeBlanc RRT CRE, Ottawa Hospital Rehabilitation Centre, 1201-505 Smyth Road, Ottawa, Ontario K1H 8M2, Canada. E-mail: cleblanc{at}ottawahospital.on.ca.
The portable oxygen concentrators were donated by the manufacturers for this study. The manufacturers had no role in the design or conduct of the study. This research was partly supported by a grant from the Institute for Rehabilitation Research and Development, the Ottawa Hospital Rehabilitation Centre, Ottawa, Ontario, which had no role in the study design, data collection or analysis, or preparation of the manuscript. The authors have disclosed no other conflicts of interest.
Ms LeBlanc presented a version of this study at the Canadian Respiratory Care Conference, held April 28–30, 2011, in Niagara Falls, Ontario, Canada. Ms Lavallée presented a version of this study at the Canadian Physiotherapy Association Congress, held May 23–27, 2012, in Saskatoon, Saskatchewan, Canada.
See the Related Editorial on Page 1711
- Copyright © 2013 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}