

Abstract
Disease processes can impair ciliary function, alter secretion production and mucus rheology, and interfere with the cough reflex. Airway clearance therapy has been a cornerstone of therapy aimed at minimizing the devastating effects of airway obstruction, infection, and inflammation due to mucus stasis on the conducting airways and lung parenchyma. Although challenges to performing clinical studies evaluating the effectiveness of airway clearance therapeutic modalities exist, resources are available in the literature. In addition to device evaluations and original clinical research, the expert opinion, systematic reviews, and evidence-based practice guidelines can be found. These tools can be used to develop protocols and pathways to guide our practice. Monitoring and reporting patient, process, and financial outcomes are essential steps germane to the implementation of evidence-based care.
- airway clearance devices
- cough
- mucociliary transport
- postural drainage
- active cycle of breathing
- positive expiratory pressure
- oscillatory positive expiratory pressure
- HFCWO
- secretion clearance
Introduction
The mucociliary escalator and cough reflex maintain optimal function of the respiratory system by removing secretions and preventing airways obstruction. In health, 10–100 mL1 of airway secretions are continuously produced and cleared by the centripetal movement of the mucociliary escalator, and with the aid of transient increases in expiratory air flow.2 There are a variety of factors that can interfere with the body's natural defense mechanism, making it difficult to mobilize and evacuate secretions from the airways. The aging process, tobacco use, and environmental exposures reduce the efficacy of ciliary structure and function.3–6 Disease processes such as progressive neurodegenerative conditions inhibit the normal cough reflex.7,8 Pulmonary disorders such as cystic fibrosis (CF), COPD, and bronchiectasis alter the production and composition of mucus, and mucociliary clearance disorders, such as primary ciliary dyskinesia, reduce the efficacy of ciliary structure and function.9–11
Airway obstruction and structural damage to the airways and lung parenchyma result from recurring secretion retention, infection, and inflammatory changes. As a result, airway clearance techniques (ACTs) and devices are used to aid in mucus mobilization and expectoration. The objectives of this paper are to describe and review the need for ACTs, discuss methodological challenges and limitations to study design, and to describe methods for applying evidence to clinical practice.
Airway Clearance Therapy: What Is It and Why Is It Needed?
ACT utilizes physical or mechanical means to manipulate air flow, aid in the mobilization of tracheal bronchial phlegm cephalad, and facilitate evacuation by coughing.12 Breathing maneuvers,13 gravity assisted drainage,14 manual techniques,15 and/or mechanical devices16–18 can be used to alter air flow and/or produce a cough or cough-like effect (Table 1). Patient age, disease severity, ease of use, comfort, and cost affect device selection, adherence to prescribed plan, and the efficacy with which secretions are removed.
Types of Airway Clearance Modalities Available to Facilitate Secretion Removal
There are a number of disease processes that impair ciliary function, alter secretion production and mucus rheology, and interfere with the cough reflex. Secretions that accumulate or are stagnant obstruct conducting airways, are conduits for bacterial colonization and infection, evoke inflammatory response, and contribute to airway and parenchymal damage (Fig. 1).

Physiological factors that reduce the efficacy of mucociliary escalator function.
Impairment of Secretion Clearance and Pulmonary Disease
Rare genetic disorders such as primary ciliary dyskinesia and Kartagener syndrome impair cilia structure and function.19,20 Although manifestations of these disorders also include chronic sinusitis, sinus hypoplasia, and secretory otitis media, repeated lower-respiratory-tract infections contribute to the development of bronchiectasis.21 Ciliary function is also altered with chronic pulmonary disease such as asthma, COPD, and CF. The literature reports impaired ciliary function, and changes in the flow or surface properties of mucus contribute to impaired mucociliary transport during exacerbations of asthma, as well as with chronic bronchitis. Thomas et al evaluated the epithelial ultrastructure and ciliary function of patients with varying degrees of asthma severity and healthy controls. Subjects with severe asthma had a significantly lower number of ciliated cells and higher dyskinesia and cilia immotility indices, compared to healthy controls or those with mild or moderate asthma.22 Ciliary disorientation and a reduction in mean cilia beat frequency were found in subjects with moderate and severe asthma.22 Mucus hypersecretion and airways inflammation limit air flow during exacerbations of asthma. Typically, as bronchodilator and anti-inflammatory agents reverse the air-flow limitations, secretion clearance functions are restored.
An increased number of abnormal cilia are found with chronic bronchitis as well. Ciliary dysfunction is exacerbated by continued cigarette use. Compared to non-smokers and ex-smokers with chronic bronchitis, those who continued to smoke had the highest percentage of ciliary abnormalities, as well as the presence of ciliary paralysis, features comparable to that found in bronchiectasis.23 Unlike asthma, mucociliary transport does not fully recover in chronic bronchitis. Recurrent infections and inflammation further reduce the number of ciliated epithelium. Hypersecretion of mucus with similar rheological characteristics to the mucus of those with CF limit air flow and affect the ability to generate effective cough flows.24 The increased propensity for mucus retention, recurrent inflammation, and infection damage conducting airways and inhibit restoration of mucociliary function.
Ciliary dysfunction in patients with CF is attributed to an abnormality of the gene that encodes for CF transmembrane conductance regulator.25 Dysregulation of the salt and water content may reduce airway surface liquid, inhibit ciliary function, and create an environment that is conducive to bacterial colonization and infection.26 As a result, an exaggerated inflammatory response occurs. The peripheral airways containing mucus filled bacteria are also host to inflammatory cells, and cellular breakdown products such as neutrophil-derived deoxyribonucleic acid and filamentous actin.27 Airways secretions are more viscous and adhesive, and therefore difficult to clear. This vicious circle of chronic infection, inflammation, and mucus stasis limits air flow in the larger airways and leads to the complete obstruction of the small peripheral airways and the development of diffuse, irreversible bronchiectasis.28,29
Neurorespiratory Dysfunction and Secretion Clearance Problems
Cough is a defense mechanism, initiated either voluntarily or by the stimulation of cough receptors located primarily in the central airways, which aids in the evacuation of secretions, and foreign substances from the respiratory tract.30 Spinal cord pathology and/or diseases of the neurorespiratory system can impact the control of motor nerves, and, depending on the level of insult, interrupt or weaken respiratory muscle function. Cervical spinal cord injuries, especially those occurring between C3 and C5, affect diaphragmatic function, and contribute to respiratory insufficiency. Patients with high cervical injuries often require long-term mechanical ventilatory support. Injuries to the thoracic and lumbar spine interrupt abdominal and intercostal muscle function and impair cough function.31 Lack of an adequate cough contributes to the development of recurrent respiratory-tract infections and atelectasis and remains a major cause of death in this patient population.32
Chronic muscle disease, such as muscular dystrophies, and motor neuron diseases cause muscle fatigue and wasting. Respiratory muscle weakness can impair a cough mechanism by reducing expiratory flow, and the expulsion phase of a cough, which hinders secretion removal and the ability to maintain adequate lung function.33,34 Flow-volume loops may be performed and evaluated for the presence of cough spikes to determine cough effectiveness. Cough spikes are large increases in expiratory flow generated from the presence of enough intrathoracic pressure to cause dynamic compression of air within the large airways as the glottis is opened during a cough maneuver.35 In a study of 53 patients with motor neuron disease, Chaudri et al reported that subjects unable to generate cough spikes were at increased risk for pulmonary infection and death (79% mortality rate), compared to those with the ability to generate cough spikes (50% mortality rate).36
Indications for Airway Clearance
ACT is indicated for individuals whose function of the mucociliary escalator and/or cough mechanics are altered and whose ability to mobilize and expectorate airways secretions is compromised. Early diagnosis and implementation of ACT, coupled with medical management of infections and airways inflammation, can reduce morbidity and mortality associated with chronic pulmonary37,38 and neurorespiratory disease.39 Today a variety of interventions may be used to enhance airway clearance, with the goal of improving lung mechanics and gas exchange and preventing atelectasis and infection. Choosing the most appropriate airway-clearance device or technique for an individual patient requires integral knowledge of device function and limitations, as well as an assessment of the patient's cognitive ability and the severity of pulmonary impairment (Table 2).
Age and Device Attributes to Consider When Matching Airway Clearance Techniques or Devices to Patient Need
Where to Look for Current Evidence
There is a lack of empirical evidence to support the superiority of any particular airway-clearance device or technique. There is much interest in developing evidence-based airway clearance protocols to guide device/technique selection. Searching through the literature to find the evidence may be a time-consuming venture. Therefore, it is important to become familiar with resources that are available to synthesize information, and the barriers that exist with respect to airway clearance research.
Studies
Evidence available in the literature can be categorized into pre-appraised levels40 (Fig. 2). Device evaluation and clinical studies lie at the base of this hierarchical structure. It is time and effort intensive to sift through the plethora of studies evaluating airway clearance techniques and devices. Moreover, there is a dearth of high level airway clearance research. High-level studies are prospective, randomized, blinded, placebo-controlled, and assess patient-important outcomes. As a result, several methodological challenges to ACT research exist. Many clinical studies have very small sample sizes and are not adequately powered. It is often difficult for a single center, especially with disease conditions that are rare, to obtain a sufficient number of subjects, and therefore report results with small samples of subjects.41 Other challenges to designing and conducting valid clinical trials exist. Due to the size and design of ACT modalities, it is difficult to mask the treatment assignment to the subject and/or the research team, making blinding nearly impossible. Knowledge of the type and/or sequence of ACT provided may influence the subject's decision to enroll in or to continue with study participation. There is also the risk that the subject's personal preferences or the researcher's knowledge of the device being used may bias study outcomes. It is also difficult to control for variations in practice and use of ACTs.
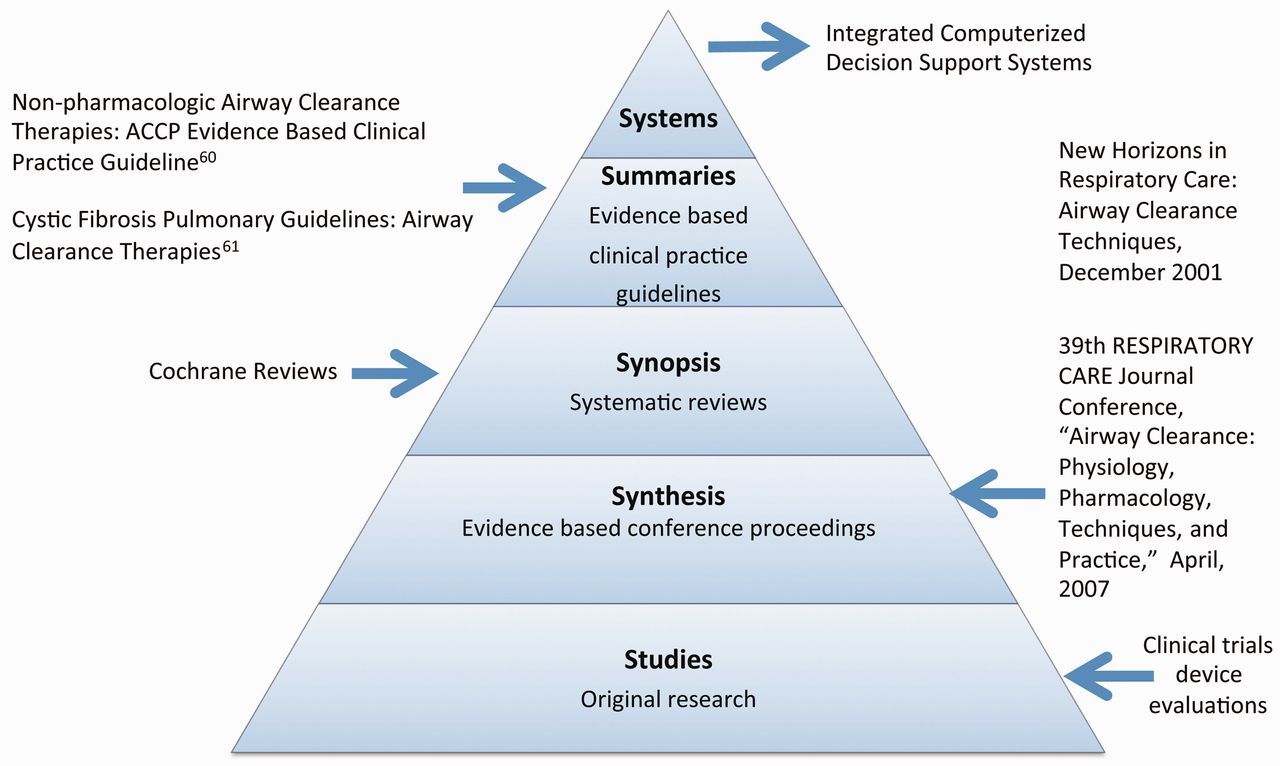
A hierarchical structure for classifying pre-appraised evidence, which can be used to evaluate the resources available to clinicians interested in appraising airway clearance research. (From reference 40, with permission.)
Alterations in device use and adherence to protocol can unintentionally influence outcomes. For example, if percussion, postural drainage, and vibration were to be provided for a 30 min period to10 consecutive patients by the same clinician, how could the researchers guarantee that the clapping and vibration were provided with the same intensity for each of those subjects? The length of the treatment of intervention may also have an impact. Since ACT is time-consuming, poor adherence to the study protocol, and/or lack of device use may occur.42 Several studies have suggested that poor adherence to prescribed ACT exists across all age ranges. For example, school-age children demonstrated ACT adherence rates of 51–74%,42 approximately 50% during adolescence,43 and 30–32% among adults.44 Lack of adherence has been linked to lengthy treatment times,45 perceived lack of efficacy for the prescribed intervention,46 coping mechanisms,47 level of education,48 and personal preference49 for the ACT device or modality. To accurately evaluate the effectiveness of ACTs it is essential to monitor and determine adherence to therapy.
There is also sparse use of sham treatment.50 Sham treatment is a medical procedure, analogous to a placebo, which is given to a control group of subjects, to enable the effects of the supposedly “active” treatment to be assessed objectively. A sham treatment is not necessarily expected to be ineffective. Rather, the purpose of a sham treatment group is to identify any specific benefit of one element of a medical treatment above and beyond all benefits that might be attributed to everything else about that treatment. Since ineffective mucociliary clearance leads to increased morbidity and mortality, ethical considerations deter the use of sham treatment in ACT research.
Synthesis
Conference proceedings review the clinical evidence and scientific basis for diagnosis and treatment of diseases or the use of therapeutic modalities. For respiratory therapists the New Horizons Symposiums and Respiratory Care Journal Conferences provide a venue for clinical experts and scientists to review and present evidence specific to our practice. Conference proceedings are then published in Respiratory Care. Two conference proceedings were dedicated to airway clearance: the New Horizons Symposium, presented at the 47th AARC Congress in December, 2001, and the 39th Respiratory Care Journal Conference, conducted in April, 2007. The scientific evidence with respect to the physiology of mucus production and cough, pharmacologic management, and non-pharmacologic approaches to airway clearance were presented and discussed, and findings summarized. The aforementioned narrative reviews also provide recommendations for new directions and opportunities for future research and clinical care.
Systematic Reviews
A systematic review is a summary of the literature that uses an organized method to thoroughly search, critically appraise, and statistically combine data from valid studies in the literature.51 This evaluation is performed systematically and rigorously, the results of which are based on the strength of the evidence found in the literature. Systematic ACT reviews are available and include reviews of specific techniques, such as active cycle of breathing,52 positive expiratory pressure devices,53 and oscillatory positive expiratory pressure devices,54 as well as sequencing pharmacologic agents,55,56 and comparing therapeutic modalities for specific diseases such as CF57 or COPD.58
Evidenced-Based Clinical Practice Guidelines
In the last decade, 2 airway clearance clinical practice guidelines have been published. Guided by systematic review of the literature from multiple databases and hand searches, authors constructed recommendations for the non-pharmacologic management of secretion clearance in pulmonary disease59 and the use of airway clearance for the treatment of CF lung disease.60 The authors acknowledged methodological limitations of airway clearance research, and reported recommendations made through these guidelines were derived from a “fair” level of evidence, or data that were valid enough to make plausible conclusions in the absence of rigorously conducted scientific studies. Recommendations were provided with respect to the general needs for airway clearance, as well as for treatment of individual patients. A summary of the pertinent findings from these guidelines can be found in Table 3.
A Summary of Clinical Practice Guideline Recommendations
Putting Evidence Into Practice
The lack of empirical evidence to determine superiority of any airway-clearance device or technique supports the need for protocols to guide device/technique selection. The literature supports the use of respiratory therapist-driven protocols. Studies demonstrate that protocol use improves appropriate allocation of respiratory services, by reducing over-ordering and under-ordering of respiratory therapies, and the cost of care.61–64 A few studies report that matching ACT to clinical need improves patient adherence and reduces missed therapy, especially when the patients are educated consumers of care and actively engaged in the ACT selection process.65–68
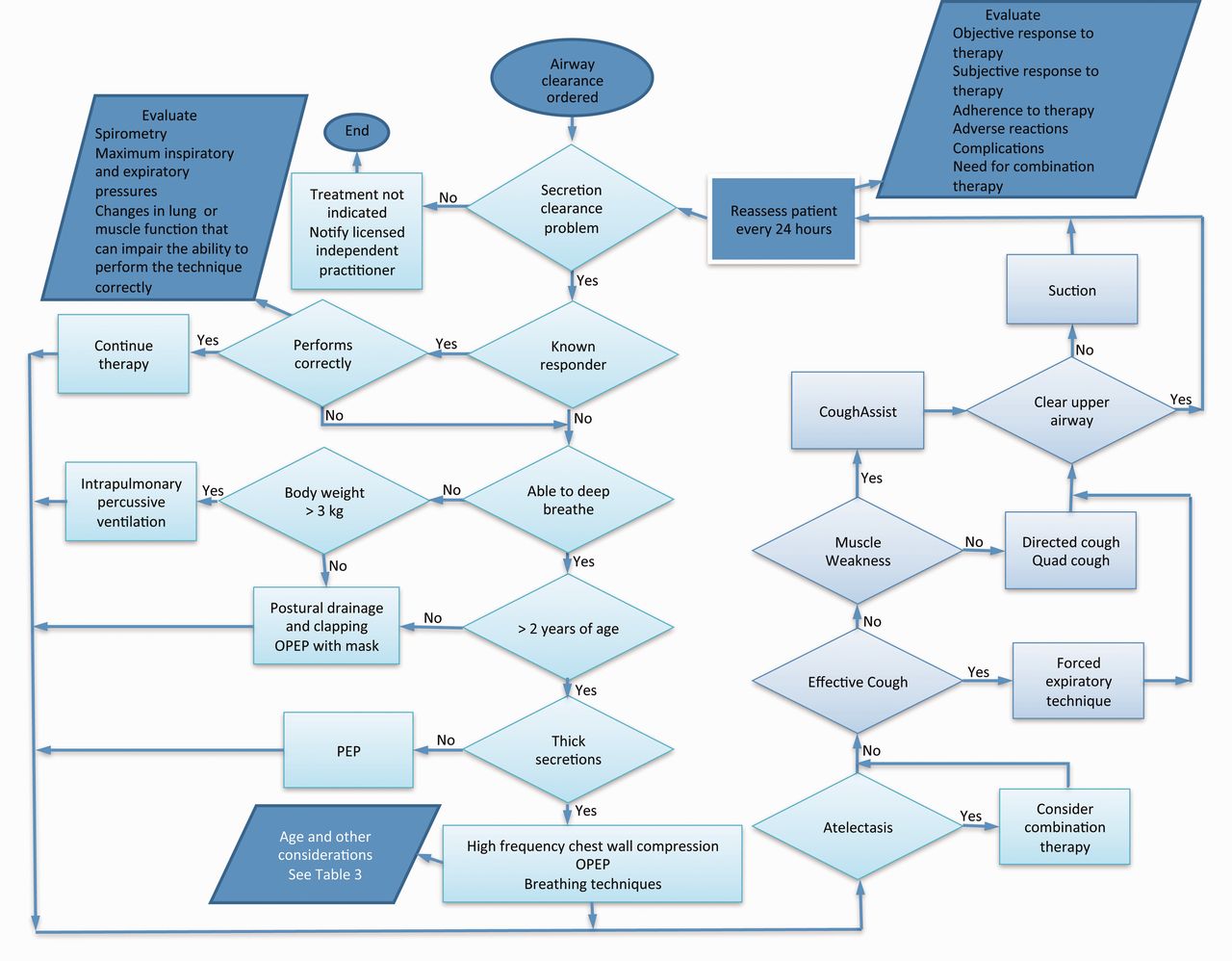
An algorithm for guiding ACT was proposed17 but did not account for an assessment of the patient's ability to perform therapy, determination of cough characteristics, or frequency of re-evaluation. This algorithm recommends to “continue effective therapy” if the patient is a “known responder.”17 However, decline in pulmonary and/or muscle function can occur during exacerbations or with time, as a function of the natural progression of the disease. The rate of decline in muscle and/or pulmonary function can affect treatment efficacy and patient outcomes. Evaluation of the need for ACT and use of a particular device or technique must include initial and ongoing assessment of the patient's lung function, muscle strength, and cognitive ability to perform the therapy. Figure 3 integrates expert opinion,12,17 evidence from published systematic reviews,52–54,57,58 and clinical practice guidelines59,60 to construct an algorithm to guide the use of ACT. The establishment and evaluation of patient, process, and financial outcomes are crucial elements in protocol implementation. A computerized system provides an efficient and cost-effective method for evaluating outcomes.69
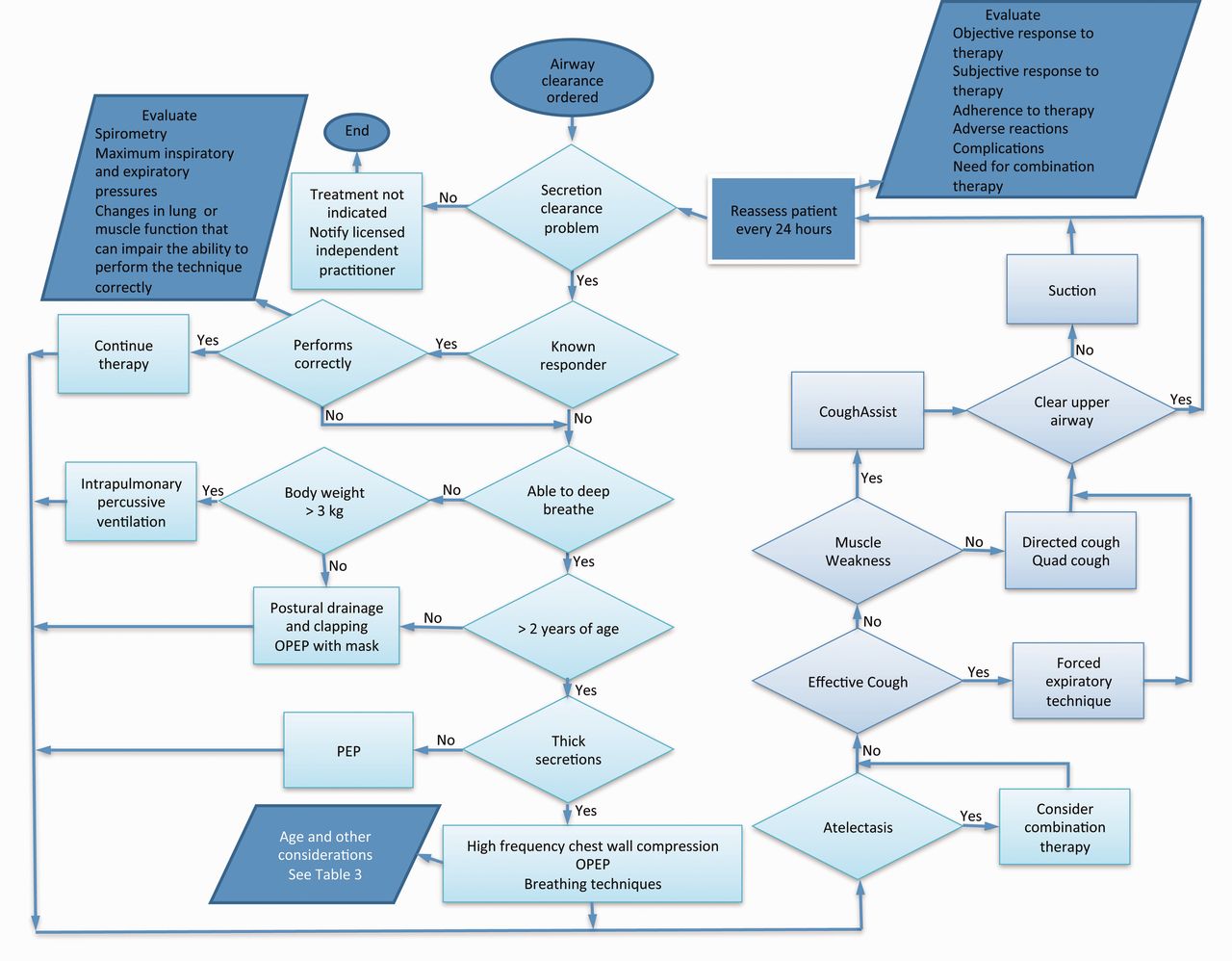
Respiratory therapist driven algorithm to guide airway clearance use. OPEP = oscillatory positive expiratory pressure.
An electronic medical record provides the potential to create an integrated system to guide practice, store health information, and evaluate patient and process outcomes (Fig. 4). It is important not only to house protocols and clinical pathways, but also to have an electronic health record that can easily perform protocol or pathway audits to determine allocation of services and patient and process outcomes. Collecting outcome variables, such as hospital or ICU stay, re-visitation rates, delays in care, missed therapy, and order variances, can waste human capital if the data collection process is cumbersome and time-consuming.
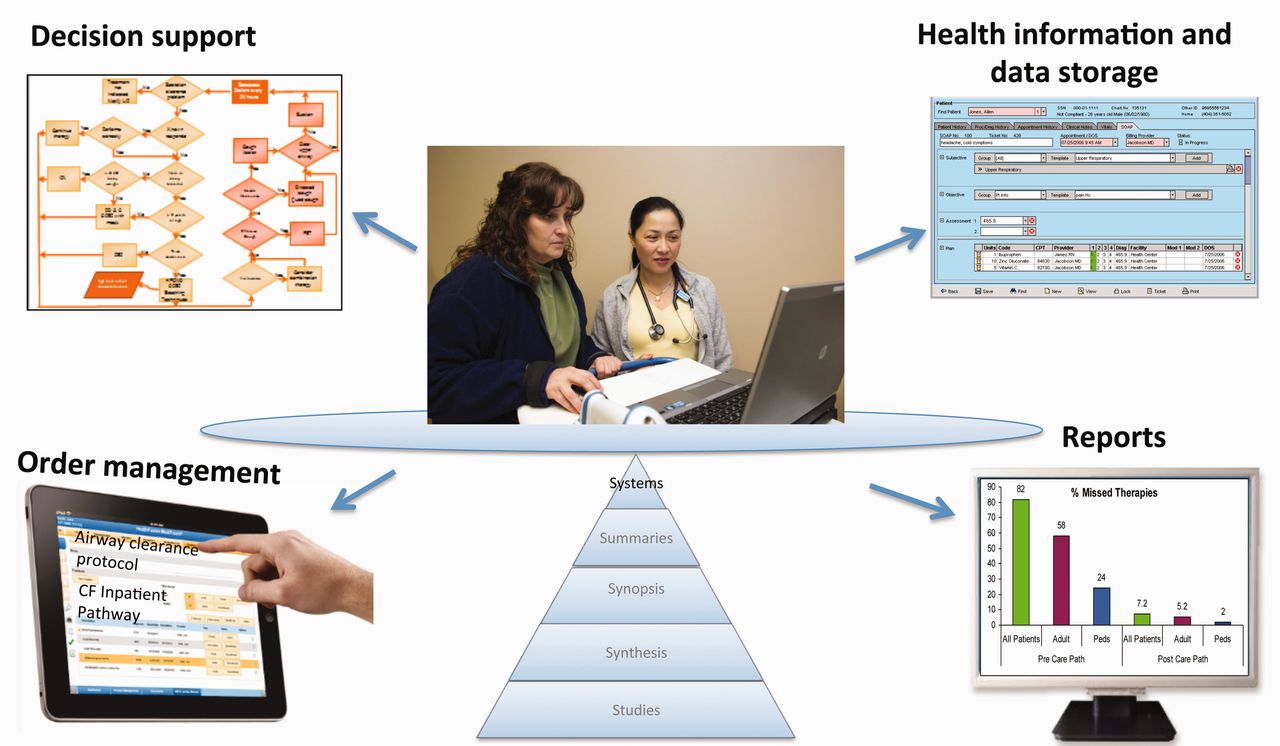
An example of an integrated system for storing health information, guiding and evaluating clinical care.
Summary
ACT has for decades been considered one of the cornerstones of therapy for the prevention and treatment of pulmonary disease and neurorespiratory dysfunction. Although there are methodological challenges that make it difficult to evaluate the clinical efficacy of ACTs clinically, literature does exist to guide our practice. An integral knowledge of ACTs (limitations of use derived from the literature, recommendations from narrative and systematic reviews, and evidence-based clinical practice guidelines), device performance, and patient characteristics (disease state, lung and muscle function, cognitive ability, preferences) is needed to construct evidence-based approaches to guide care.
Footnotes
- Correspondence: Teresa A Volsko MHHS RRT FAARC, Department of Respiratory Care, Akron Children's Hospital, One Perkins Square, Akron OH 44308. E-mail: tvolsko{at}chmca.org.
Ms Volsko presented a version of this paper at the 28th New Horizons in Respiratory Care Symposium, “The Scientific Basis for Respiratory Care,” at the AARC Congress 2012, held November 10–13, 2012, in New Orleans, Louisiana.
The author has disclosed no conflicts of interest.
- Copyright © 2013 by Daedalus Enterprises
References
- 1.↵
- 2.↵
- 3.↵
- 4.
- 5.
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.
- 63.
- 64.↵
- 65.↵
- 66.
- 67.
- 68.↵
- 69.↵









{kind=link}
{kind=link}
{kind=link}
{kind=link}