

Abstract
BACKGROUND: Growth-arrest-specific protein 6 (GAS6) is a vitamin K-dependent protein expressed by endothelial cells and leukocytes participating in cell survival, migration and proliferation and involved in many pathological situations. The aim of our study was to assess its implication in ARDS and its variation according to PEEP setting, considering that different cyclic stresses could alter GAS6 plasma levels.
METHODS: Our subjects were enrolled in the ExPress study comparing a minimal alveolar distention (low-PEEP) ventilatory strategy to a maximal alveolar recruitment (high-PEEP) strategy in ARDS. Plasma GAS6, interleukin-8 (IL-8), and vascular endothelial growth factor (VEGF) levels were measured at day 0 and day 3 by enzyme-linked immunosorbent assay in blood samples prospectively collected during the study for a subset of 52 subjects included in 8 centers during year 2005.
RESULTS: We found that GAS6 plasma level was elevated in the whole population at day 0: median 106 ng/mL IQR 77–139 ng/mL, with significant correlations with IL-8, the Simplified Acute Physiology Score II and the Organ Dysfunction and Infection scores. Statistically significant decreases in GAS6 and IL-8 plasma levels were observed between day 0 and day 3 in the high-PEEP group (P = .02); while there were no differences between day 0 and day 3 in the low-PEEP group.
CONCLUSIONS: GAS6 plasma level is elevated in ARDS patients. The high-PEEP strategy is associated with a decrease in GAS6 and IL-8 plasma levels at day 3, without significant differences in day 28 mortality between the 2 groups. (Clinicaltrials.gov NCT00188058).
Introduction
Growth-arrest-specific protein 6 (GAS6) is a vitamin-K-dependent protein, sharing 43% of homology with a natural anticoagulant, protein S.1 GAS6 is expressed in various cell types, including endothelial cells, particularly in pro-apoptotic conditions.2 Leukocytes have also been found to release GAS6.3–4 It is a ligand for 3 tyrosine kinase receptors (Axl, Tyro3, and Mer), whose signaling is implicated primarily in cell survival but also in cell proliferation, adhesion, and migration.5
Among several functions, previous studies have reported the implication of GAS6 in the inflammatory process, particularly in the physiopathology of severe sepsis.3,4,6,7 Indeed, GAS6 enhances the interplay of cells implicated in the inflammatory response, endothelial cells, leukocytes, and platelets during different conditions of experimental inflammation.4 Models of endotoxemia also suggest an important role in modulation of the immune response.4–5,8–11
Given the involvement of GAS6 receptors in experimental sepsis, and the potentially major role of leukocyte apoptosis in the pathophysiology of severe sepsis, previous clinical studies have focused on GAS6 in septic and non-septic critical care patients.3,6–7 As compared to healthy subjects, GAS6 levels were higher in critical care patients with one or several failing organs, the highest values being observed in patients with severe sepsis.3 Specifically, in severe sepsis patients a correlation was observed between the number of organ dysfunctions (as reflected by scores such as the Sepsis-Related Organ Failure Assessment and the Organ Dysfunction and Infection score) reflecting the degree of tissue injury, and the GAS6 plasma concentration.3,6
GAS6 can be released by endothelial cells and leukocytes, which are largely implicated in the pathophysiology of ARDS. Since the pulmonary vascular bed is subjected to cyclic stress in patients with ARDS, and despite the lack of in vitro or experimental studies evidencing that GAS6 could be modulated by such cyclic stress, we hypothesized that the course of plasma GAS6 levels could differ according to different ventilatory strategies. We conducted a multicenter randomized controlled trial to compare the course of plasma GAS6 levels in patients with ARDS from the Expiratory Pressure (ExPress) Study Group.12 Briefly, patients were randomly assigned to either a low-PEEP (minimal alveolar distention) strategy or a high-PEEP (increased alveolar recruitment) strategy. The high-PEEP strategy, avoiding in part the consequences of cyclic collapse and excessive hyperinflation, could be associated with less injury and lower plasma GAS6. Additionally, we measured plasma interleukin-8 (IL-8) and vascular endothelial growth factor (VEGF) as established endothelial and leukocyte markers with important implications in ARDS.13–22
QUICK LOOK
Current knowledge
Growth arrest-specific protein 6 (GAS6) is a vitamin-K-dependent protein expressed by endothelial cells and leukocytes, which are important in the pathophysiology of ARDS. GAS6 participates in cell survival, migration, and proliferation.
What this paper contributes to our knowledge
Plasma GAS6 level was elevated in patients with ARDS. An open-lung, high-PEEP strategy was associated with lower GAS6 than was a low-PEEP strategy. The role of GAS6 measurement in guiding ARDS treatment and prognosis remains to be determined.
Methods
We measured plasma GAS6, IL-8, and VEGF in a subset of ARDS subjects enrolled in the ExPress Study. The 767 subjects were randomized into 2 groups. In the low-PEEP group, PEEP and inspiratory plateau pressure were kept as low as possible without falling below the oxygenation targets (SpO2 88% and/or PaO2 55 mm Hg). External PEEP was set to maintain total PEEP (the sum of external and intrinsic PEEP) between 5 and 9 cm H2O. In the high-PEEP group, PEEP was adjusted based on airway pressure and was kept as high as possible without increasing the maximal inspiratory plateau pressure above 28–30 cm H2O. For both groups, tidal volume (VT) was set at 6 mL/kg of predicted body weight.
Plasma GAS6, IL-8, and VEGF were measured in blood samples prospectively collected during the last year (2005) of the ExPress study, at day 0 and day 3 in 8 selected centers. The present study concerned only the year 2005, because the rationale originated from results obtained shortly before 2005, that implicated GAS6 in severe sepsis.3 Given these conditions, 52 subjects were included in the present study: 24 in the low-PEEP group, and 28 in the high-PEEP group. The study protocol (approval number 2002/09, 08-Jul-2002) and the corresponding amendment (amendment 8; 15-Feb-2005) were approved by the ethics committee of the Angers University Hospital (Comité Consultatif de Protection des Personnes dans la Recherche Biomédicale). Measurement of plasma GAS6, IL-8, and VEGF were via enzyme-linked immunosorbent assay, as previously described.23–24
Statistical Analysis
Continuous data are expressed as median and IQR, and were compared using nonparametric tests (Mann-Whitney test, Wilcoxon signed-rank test, or Kruskal-Wallis test, as appropriate). Categorical data are expressed as number and percentage, and were compared with the chi-square test. Correlations were assessed with the nonparametric Spearman correlation test or with the nonparametric test for trend, as appropriate. P < .05 was considered significant. Analyses were performed using statistics software (StatView, SAS Institute, Cary, North Carolina).
Results
Plasma GAS6, IL-8, and VEGF were measured at day 0 and day 3 in 52 subjects from the ExPress study (7% of the 768 subjects). The main clinical characteristics at inclusion, including classification according to the new Berlin definition of ARDS,25 are shown in Table 1. Characteristics at day 3 and relevant physiological and clinical end points until day 28 are shown in Table 2.
Subject Characteristics at Inclusion
Subject Characteristics at Day 3 and End Points Until Day 28
As expected, there was a statistically significant difference in PEEP at day 3 (7 cm H2O [IQR 5–8 cm H2O] versus 15 cm H2O [IQR 10–17 cm H2O]), and there was no difference in PEEP at day 0, nor in VT at day 0 or day 3.
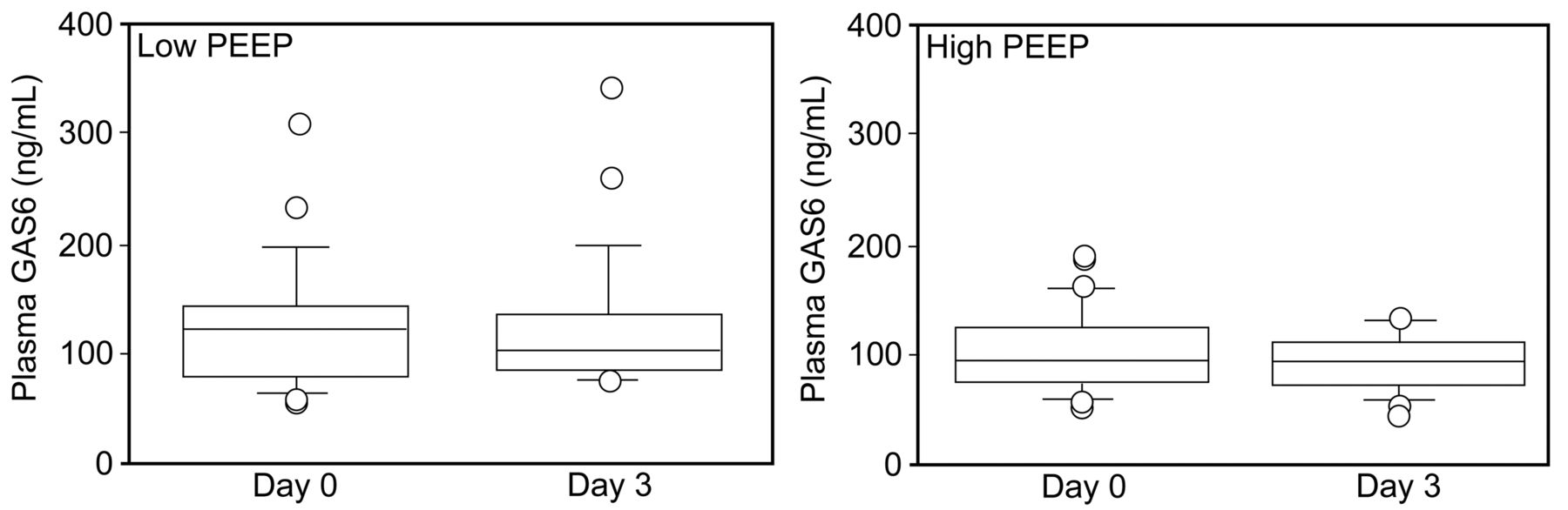
The main biological results at day 0 and day 3 are shown in Table 3. GAS6 was very high in subjects at the onset of ARDS (106 ng/mL, IQR 77–139 ng/mL), with no statistically significant difference between the low-PEEP group and the high-PEEP group: 121 ng/mL (IQR 80–143 ng/mL) versus 93 ng/mL (IQR 73–123 ng/mL), respectively (P = .17) (Figure). Considering all 52 subjects, there was a trend (P = .15) toward lower GAS6 in the subjects with less severe ARDS according to the Berlin classification25: mild ARDS 92 ng/mL (IQR 80–96 ng/mL), moderate ARDS 115 ng/mL (IQR 82–143 ng/mL), severe ARDS 127 ng/mL (IQR 67–144 ng/mL).
Plasma Growth-Arrest-Specific Protein 6, Interleukin-8, and Vascular Endothelial Growth Factor
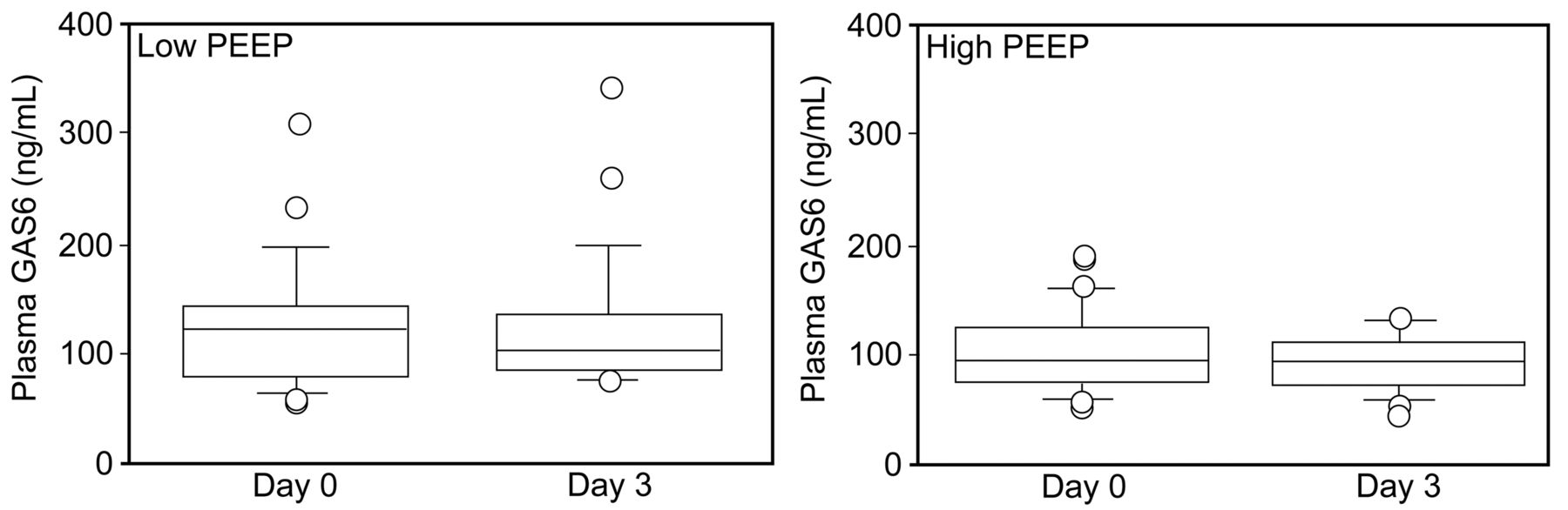
Plasma growth-arrest-specific protein 6 (GAS6) concentration, measured via enzyme-linked immunosorbent assay at day 0 and day 3 in low-PEEP and high-PEEP groups. There was a significant difference in GAS6 between day 0 and day 3 in the high-PEEP group, but not in the low-PEEP group.
GAS6 correlated positively with the severity of disease, as assessed by the Simplified Acute Physiology Score II (ρ = 0.43, P = .002) and the Organ Dysfunction and Infection score (ρ = 0.40, P = .007), which indicates the number of organ dysfunction (varying between 0 and 7, including clinically evident infection as an organ dysfunction). There was no correlation between GAS6 at day 0 and PEEP and VT. There was no difference in GAS6 at day 0 between the septic (n = 33) and the non-septic subjects (n = 19).
A significant difference between plasma GAS6 at day 0 and day 3 was found in the high-PEEP group (P = .02) but not in the low-PEEP group (P = .83). We found elevated IL-8 at day 0, but there was no significant difference between the 2 groups. There was a statistically significant correlation between GAS6 and IL-8 at day 0 (ρ = 0.40, P = .006), but not at day 3. A significant difference between IL-8 at day 0 and day 3 was found in the high-PEEP group (P = .02) but not in the low-PEEP group (P = .63).
We found elevated VEGF at day 0, but there was no significant difference between the 2 groups. There was no statistically significant correlation between VEGF and GAS6 at day 0 or day 3. Similarly, there was no statistically significant correlation between VEGF and IL-8 at day 0 or day 3. There were no significant differences in VEGF at day 0 versus day 3, in either the high-PEEP or the low-PEEP groups. And there were no differences in IL-8 or VEGF at day 0 between the septic and non-septic subjects.
Discussion
As expected, according to a previous study with more heterogeneous critically ill subjects, GAS6 was very high in subjects at the onset of ARDS (106 ng/mL [IQR 77–139 ng/mL]), compared to reference values from spontaneously breathing healthy subjects (54 ng/mL [IQR 49–68 ng/mL]).3 We also found elevated IL-8 and VEGF at the onset of ARDS, confirming previous series.13–15,17,19–21 A positive correlation was found between GAS6 and IL-8. A significant decrease in GAS6 and IL-8 was observed in the high-PEEP group, but not in the low-PEEP group.
This is the first report of elevated GAS6 in a homogeneous group of ARDS patients. Obviously, over-expression of GAS6 was very likely in relation to disease severity, as assessed via Simplified Acute Physiology Score II and Organ Dysfunction and Infection scores) and sepsis (33 subjects in the series). Since it was previously proposed that GAS6 originates from endothelial cells and leukocytes,3,4 increase in GAS6 production could also be partly related to pulmonary neutrophil infiltration and to diffuse pulmonary endothelial damage, which are key features of ARDS.13,26 Moreover, despite the lack of surrounding experimental studies, it was tempting to assume that mechanical ventilation, by applying cyclic stress over pulmonary endothelial cells and increasing leukocyte production, could be a contributing factor to the high GAS6 at day 0 and day 3. As previously described in patients with severe sepsis,3,6 GAS6 correlated positively with the severity of disease, as assessed by the Simplified Acute Physiology Score II and the Organ Dysfunction and Infection score. The correlation values were in the same range as previous reports from our group and others, adding external validity to our results.3,6 However, they are just indicators of association between disease severity and GAS6, and any causal relationship remains to be investigated. We found no correlation between GAS6 at day 0 and PEEP or VT, parameters that obviously influence cyclic stress on the pulmonary vasculature. However, VT at day 0 was approximately 6 mL/kg ideal body weight: a VT known to minimize lung stress.15 Therefore, the chance of observing a statistical correlation between GAS6 and VT as a marker of lung stress was minimized. There was also a rather narrow spectrum of PEEP settings at day 0, which could partly explain the lack of correlation with GAS6 at day 0. Unfortunately, we did not measure transpulmonary pressures, which could have provided a better surrogate of the stress applied to the pulmonary vasculature.
The significant difference between GAS6 at day 0 and day 3 could be partly explained by less stress on the pulmonary vascular and endothelial bed in the high-PEEP group, because higher PEEP decreases cyclic reopening of collapsed lung. Accordingly, we observed no significant variation in GAS6 in the low-PEEP group, in which there was no significant difference in PEEP between day 0 and day 3. In contrast, the high-PEEP group had a significant decrease in GAS6 in parallel with a PEEP increase from 8 cm H2O (IQR 5–10 cm H2O) to 15 cm H2O (IQR 10–17 cm H2O). Such differences according to ventilatory strategy have previously been reported for inflammatory mediators and apoptosis markers, at both the pulmonary and systemic level.13,15 In the same way, PEEP could have impacted GAS6 in our ARDS subjects. We found elevated IL-8 at day 0, in accordance with previous series of ARDS subjects.13–15,17,20,21 Given the implication of IL-8 as an important pro-inflammatory mediator associated with the development of ARDS and with poor outcomes (worse mortality and fewer ventilator-free days), the observed correlation with GAS6 suggests that GAS6 is an important contributor to inflammation in ARDS.
We found elevated VEGF at day 0, confirming previous results from Azamfirei et al.19 However, elevated VEGF was not observed in another series.22 Moreover, differential expression of VEGF at the pulmonary and plasma levels has previously been reported.19 The implication of VEGF in early ARDS is not fully established, since VEGF can increase vascular permeability but can also exert a protective vascular effect.16,19,22 Therefore, the lack of correlation between GAS6 and VEGF could reflect the fact that plasma VEGF probably poorly reflects localized pulmonary inflammation.
In the ExPress study the high-PEEP strategy was associated with better oxygenation, higher lung compliance, more ventilator-free days, and more organ-failure-free days.12 In the present study we observed in a representative subset of subjects a decrease in GAS6 at day 3 in the high-PEEP group, unlike the low-PEEP group. This was in parallel to better oxygenation and higher lung compliance values at day 3, suggesting a possible relationship between those clinical benefits and the biological findings. The animal experiments by Tjwa et al4 also support a relationship between such biological findings and clinical benefits: they reported that GAS6 could be involved in the inflammatory process and could increase the inflammatory response in conditions such as sepsis and ARDS, and inhibition of GAS6 might be a treatment for sepsis. Importantly, such GAS6 inhibition should not be interpreted as a decrease to information to cell survival, but rather as a return to a controlled physiologic state, by limiting GAS6-induced inflammation.
We also found a decrease in IL-8 between day 0 and day 3 in the high-PEEP group, but not in the low-PEEP group. Considering the key role of IL-8 in ARDS, that result suggests benefit from the high-PEEP strategy, and confirms previous series demonstrating a link between ventilator settings and IL-8.13,15
The first limitation to our study is that we cannot distinguish between the distinct effects of pulmonary insult and mechanical ventilation on the GAS6 measurements from healthy subjects, since they cannot be subjected to mechanical ventilation. The generalization of the present results is also a critical point: measurements were possible only in a few ExPress centers, and only during the last year of the study. The 2 groups were clinically comparable and similar to the whole population of the ExPress study, but, given the low number of subjects, we cannot exclude the possibility of type-2 error with regard to baseline characteristics, and especially to the repartition of the subjects between the 3 ARDS categories.
Another limitation is that the measurements were limited to plasma. Our hypothesis is that plasma GAS6 originates at least in part from lungs, but only bronchoalveolar lavage studies in ARDS patients could confirm that hypothesis, and, unfortunately, bronchoalveolar lavage GAS6 measurements were not possible during the ExPress study.
Another limitation is the lack of GAS6 measurements after day 3, precluding any conclusion on the implication of GAS6 in end-stage ARDS. However, it is generally believed that GAS6 is an acute-phase reactant.27
Conclusions
Plasma GAS6 was elevated at ARDS onset, and a high-PEEP strategy was associated with decreased GAS6 at 3 days. Further studies are warranted to confirm that the lungs are a major contributor to the plasma GAS6, to extend our knowledge about the kinetics of plasma GAS6 in the course of ARDS, and to delineate the prognostic and pathogenetic value of GAS6 as a biomarker in ARDS.
Acknowledgments
We thank Véronique Remones for her excellent technical assistance.
Footnotes
- Correspondence: Jean-Luc Diehl MD, Medical Intensive Care, Hôpital Européen Georges Pompidou, 20 Rue Leblanc, CEDEX 15, Paris 75908 France. E-mail: jldiehl{at}invivo.edu.
The ExPress study was supported by the Programme Hospitalier de Recherche Clinique, French Minister of Health. Dr Brochard has disclosed relationships with Dräger, Maquet, Covidien, Phillips, and General Electric. The other authors have disclosed no conflicts of interest.
- Copyright © 2013 by Daedalus Enterprises









{kind=link}