

Abstract
BACKGROUND: Flutter VRP1, Shaker, and Acapella are devices that combine positive expiratory pressure (PEP) and oscillations.
OBJECTIVES: To compare the mechanical performance of the Flutter VRP1, Shaker, and Acapella devices.
METHODS: An experimental platform and a ventilator, used a flow generator at 5, 10, 15, 20, 26, and 32 L/min, were employed at angles of –30°, 0°, and +30° to evaluate Flutter VRP1 and Shaker, whereas Acapella was adjusted at intermediate, higher, and lower levels of resistance, including positive expiratory pressures (PEP) along with air outflow rates and oscillation frequencies.
RESULTS: When the relationships between pressure amplitudes of all air flows were analyzed for the 3 devices at low and intermediate pressures levels, no statistically significant differences were observed in mean pressure amplitudes between Flutter VRP1 and Shaker devices. However, both devices had different values from Acapella, with their pressure amplitude values being higher than that of Acapella (P = .04). There were no statistically significant differences in PEP for the 3 angles or marks regarding all air flows. The expected relationships between variables were observed, with increases in PEP, compared to those of air flows and resistance. Nevertheless, there was a statistically significant difference in frequency of oscillation between these devices and Acapella, whose value was higher than those of Flutter VRP1 and Shaker devices (P = .002). At intermediate pressure levels, the patterns were the same, in comparison to low pressures, although the Acapella device showed frequencies of oscillation values lower than those of Flutter VRP1 and Shaker (P < .001). At high pressures, there were no statistically significant differences among the 3 devices for frequency of oscillations.
CONCLUSIONS: The Flutter VRP1 and Shaker devices had a similar performance to that of Acapella in many aspects, except for PEP.
- Flutter VRP1
- Shaker
- Acapella
- positive expiratory pressure
- PEP
- mucociliary transport
- high-frequency oscillation
Introduction
In normal individuals, respiratory mucus is removed from the lungs by the mucociliary system, but in pathological conditions, such as chronic bronchitis, cystic fibrosis, bronchiectasis, and asthma, there is hypersecretion along with qualitative changes in the bronchial mucus. In these situations, besides modifications in the characteristics of bronchial mucus, epithelium may also be altered, hindering normal ciliary function and resulting in inefficient ciliary mucus clearance, which is partially compensated for by coughing.1–3
Some techniques have been developed for physical therapy to facilitate bronchial clearance of secretions, increasing the quantity of expectorated mucus, preventing infections of the respiratory tract, and improving pulmonary function.4–6 Many recent techniques of bronchial clearance are described in the literature in an attempt to provide patients with greater independence.7–9
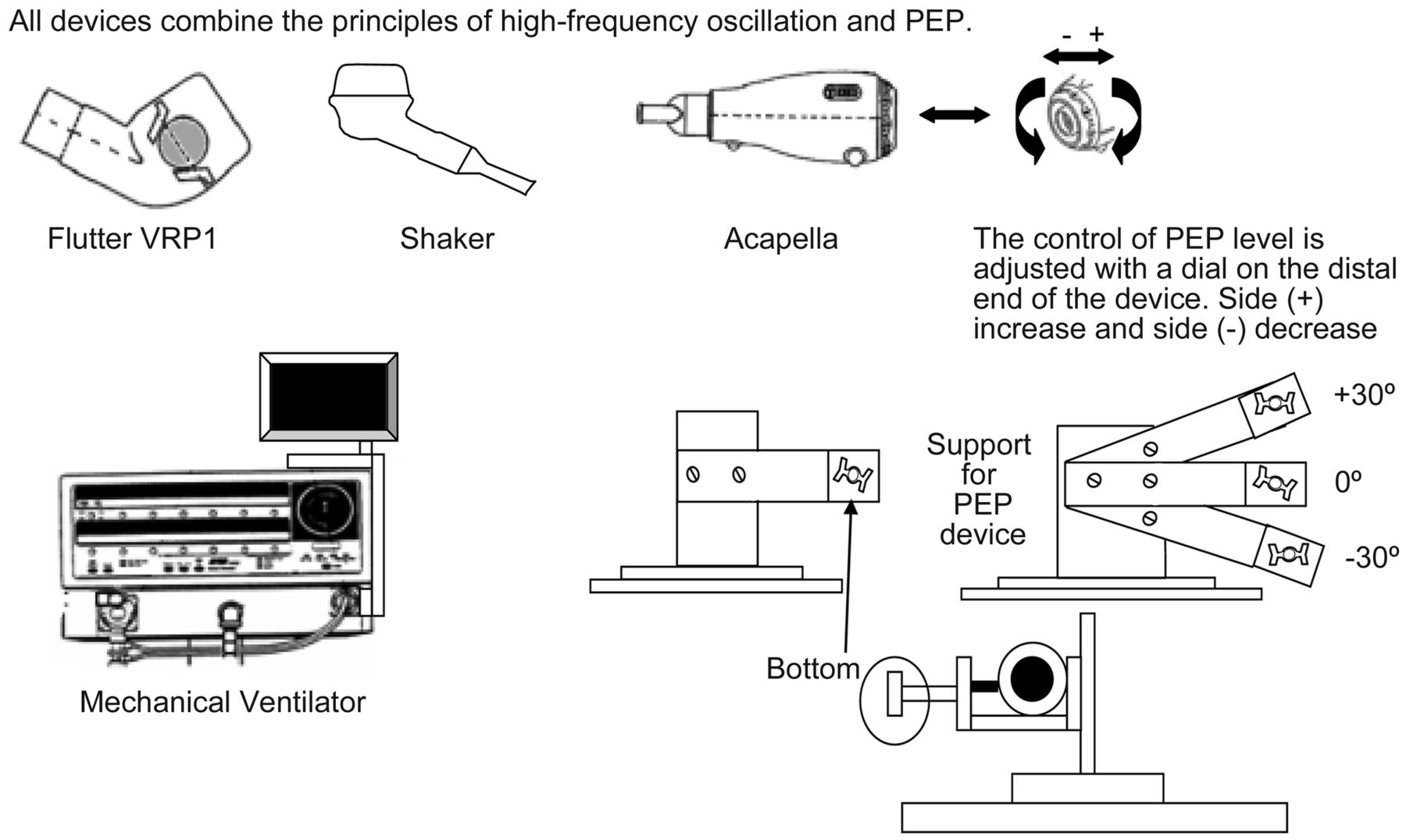
Among these physiotherapy techniques, positive expiratory pressure (PEP) combined with high-frequency oscillation (HFO) can be produced by devices that produce oscillatory positive pressures during expiration. These devices produce short and successive interruptions of the air flow, promoting vibrations during expiration by different mechanisms.9
The Flutter VRP1 was designed by Lindemann (Fig. 1) and is a small, easily manageable pocket device, similar to a pipe.10 The Flutter device is made up of 4 parts: a body with a mouthpiece, a circular cone, a stainless steel sphere, and a protective cap through which air flows when expired. During expiration through the mouthpiece, pressure increases in the mouth and causes up-and-down movements of the stainless steel sphere, creating repetitive open-close cycles and thereby producing pressure oscillations. Displacement of the sphere during expiration is the result of the equilibrium between air pressure, the force of gravity on the sphere, and the angle of contact of the cone.9,11
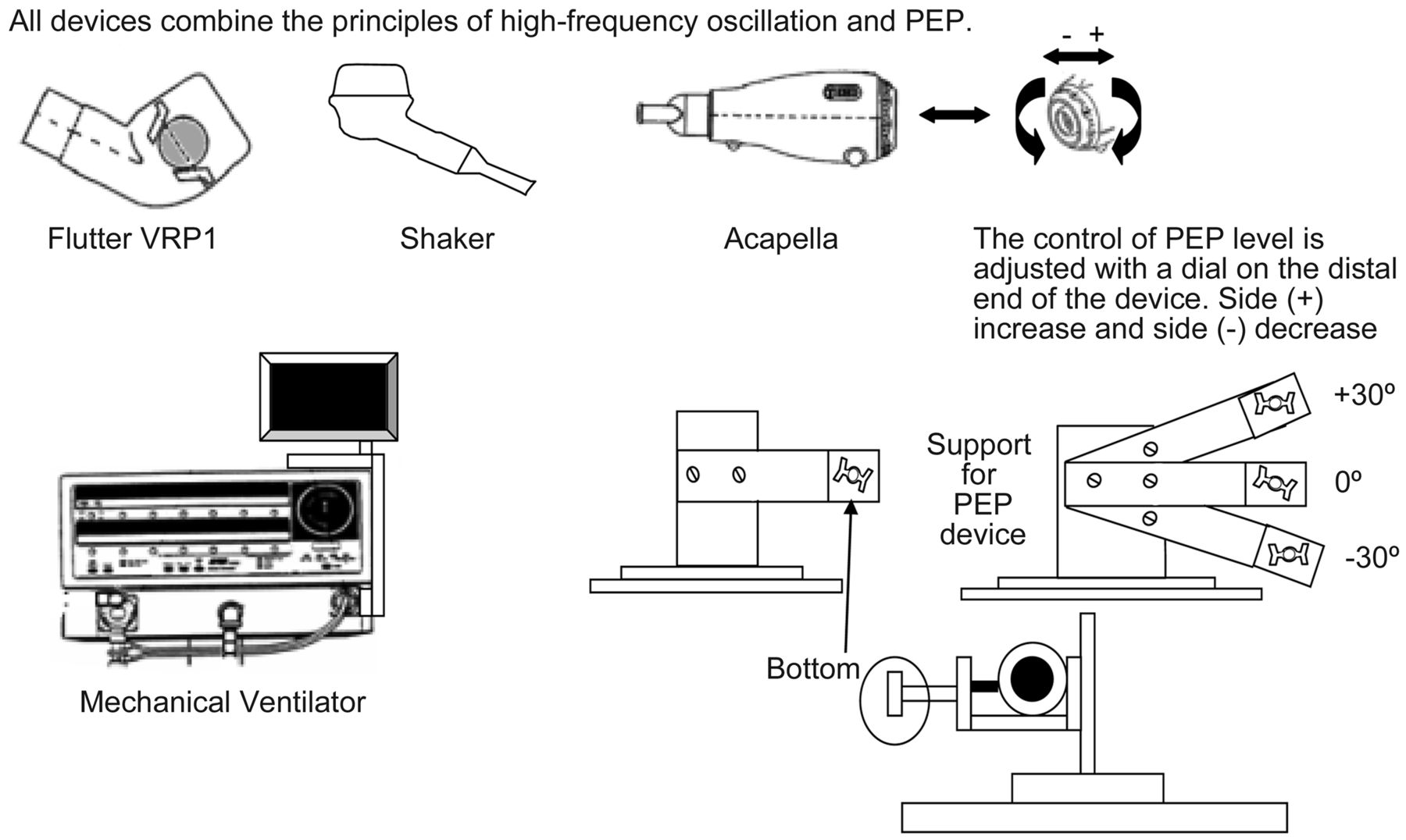
Tested devices (Flutter VRP1, Shaker, and Acapella) and the main components of the the test setup. With −30°, 0°, and 30° testing angles are designated low, intermediate, and high. PEP = positive expiratory pressure.
The Acapella device (see Fig. 1) was developed by DHD Healthcare (Wampsville, New York), which includes 2 types: a blue one for patients who cannot maintain their expiratory flow above 15 L/min for > 3 seconds, and a green one for patients who can maintain expiratory flow above or equal to 15 L/min for at least 3 seconds. Acapella can be used in any position, as its function does not depend on gravity. It has a single control on the posterior portion of the apparatus, that can simultaneously adjust the frequency of oscillation and the resistance to expiratory flow by moving a magnetic counterweight, successively interrupting the expiratory flow.12
Based on the therapeutic responses obtained with the Flutter VRP1, the NCS Indústria e Comércio in São Paulo, Brazil, developed a national prototype called Shaker (see Fig. 1). The Shaker device is made up of a blue plastic measuring 20 × 8 × 3 mm in diameter, containing a circular cone, a protective cap with 12 holes of 3 mm, and a stainless steel sphere weighing 30 g. The dimensions and gravity-dependent mechanism are similar to those of the Flutter, with the possibility of exchanging the mouthpiece position.
Oral oscillation devices for respiratory physiotherapy are an increasingly used alternative to the traditional treatment,7 being well accepted by patients and allowing non-supervised use. These aspects favor their acceptance by patients and adherence to treatment; however, it is also necessary to associate the physiopathological mechanism of the hypersecretion disease to the functioning mechanism of the devices being used.9
Because there are clinical and mechanical evaluation studies using Flutter10–15 and Acapella12,16,17 devices, but none evaluating the Shaker apparatus regarding mechanical functioning or use in patients, it was decided to reproduce the conditions proposed by Lindeman10 and compare the mechanical performance of the 3 devices. The objective of this study was to compare frequency of oscillation, expiratory pressure, and pressure amplitude of the Flutter, Shaker, and Acapella devices.
QUICK LOOK
Current knowledge
Oral oscillation devices for secretion clearance are an increasingly used alternative to the traditional treatment, being well accepted by patients and allowing nonsupervised use. These devices produce short and successive interruptions of air flow, promoting vibrations during expiration, by different mechanisms.
What this paper contributes to our knowledge
The mechanical behavior of the Shaker device is similar to that of Acapella, but with better linearity at higher air flows. The pressure amplitude produced by Flutter and Shaker devices was greater at low and high pressures. The Acapella device produced similar pressure amplitude at intermediate pressure. The frequency of oscillation was higher for the Flutter and Shaker devices at intermediate pressure. The levels of positive expiratory pressure produced by the 3 devices were not different. All 3 devices produce pressure and oscillation, which aid in the transport of respiratory secretions.
Methods
The experimental situation involved Flutter VRP1, Shaker, and Acapella devices connected to a mechanical ventilator (8400 STi, Bird Products, St Paul, Minnesota) equipped with a graphic monitor (Intermed Equipamentos Médico Hospitalar, Cotia, São Paulo, Brazil). The devices were assessed in an experimental setup (Fig. 2) at the ICU. Both experimental setup and ventilator parameters were: controlled volume, squared waveform, tidal volume 2,000 mL, frequency zero, and sensitivity of –1 cm H2O, without PEEP. The mechanical ventilator circuit consisted of inspiratory and expiratory limbs, corresponding to 2 tracheas united by a Y-piece. The devices were attached to a wooden support frame with angle adjustments for –30°, 0°, and +30°.

Experimental setup and pressure and flow waveforms.
The positions of the Flutter and Shaker devices were based on work done by Lindemann.10 Thus, these positions were used to generate low, intermediate, and high pressures. The Acapella was adjusted according to resistance to the expiratory flow control positioned on the back of the device. A rotating ring functioned as a modulator of PEP and frequency of oscillation. By turning the ring all the way to the left, low pressures were obtained; with the ring set at the median mark, intermediate pressures were produced; and by rotating the ring all the way to the right, high pressures resulted (see Fig. 1). Data on expiratory pressure, frequency of oscillation, and amplitude of pressure for each flow determined at each angle or predetermined pressure adjustment were analyzed, as shown in Table 1.
Air Outflow and Resistance Settings
The inspiratory valve was opened by activating the manual trigger control of the mechanical ventilator. Flow was conducted toward the devices (Flutter VRP1, Shaker, or Acapella) through the inspiratory limb of the ventilator circuit and maintained for 3 seconds at each stipulated air outflow level (5, 10, 15, 20, 26, and 32 L/min) at angles of –30°, 0°, and +30° for the Shaker and Flutter VRP1 devices, and at the predetermined marks for Acapella. At the end of this period, the graphic presentation on the monitor was halted. The time frame between the second and third second was selected for analysis of pressure amplitude, PEP, and frequency of oscillation at each angle or mark for all air flows, with this procedure being repeated 3 times. Therefore, after 3 seconds the image on the monitor was halted, and with the help of a manually controlled cursor, the numerical pressure values were read in the time frame between the second and third seconds. The highest values were selected for PEP differences between the maximum and minimum points of pressure amplitude, as well as the number of time variations in the frequency of oscillation. A frequency counting began from the highest expiratory pressure point and finished at the lowest one.
The mean values of all 3 measurements were used for analysis of each variable. Data were analyzed by using 2-way analysis of variance and post-hoc Tukey analysis after correction for multiple analyses with statistical software (SPSS 7, SPSS, Chicago, Illinois) at a significance level of P < .05.
Results
Table 2 shows the mean, minimum, and maximum values regarding frequency of oscillation, PEP, and pressure amplitude. When the relationships between pressure amplitudes of all air flows were analyzed for the 3 devices at low and intermediate pressures levels, no statistically significant differences were found in the mean pressure amplitudes between Flutter VRP1 and Shaker devices. However, both these devices had higher values for pressure amplitude, compared to that of Acapella (P = .04).
Pressure Amplitude, PEP, and Oscillation Frequency
The mean values for pressure amplitude of the Flutter VRP1, Shaker, and Acapella devices were, respectively, 10.48, 10.36, and 6.48 cm H2O at low pressure; 7.26, 7.40, and 9.48 cm H2O at intermediate pressure; and 7.25, 6.41, and 5.15 cm H2O at high pressure (Table 2 and Fig. 3).

Flow versus pressure amplitude, positive expiratory pressure (PEP), and oscillation frequency with the Flutter VRP1, Shaker, and Acapella.
The positive expiratory pressures of the Flutter VRP1, Shaker, and Acapella devices were similar. The mean values were, respectively, 11.18, 11.48, and 10.31 cm H2O at low pressure; 14.53, 14.9, and 13.48 cm H2O at intermediate pressure; and 16.86, 16.88, and 19.41 cm H2O at high pressure (see Table 2 and Fig. 2). The expected relationships between variables were also observed, with increases in PEP, air flow, and resistance (see Fig. 2).
As to the frequency of oscillation regarding all air flows for the 3 devices at low, intermediate, and high pressures, no statistically significant differences were observed between the Flutter VRP1 and Shaker devices. Nevertheless, there was a statistically significant difference between these 2 devices and the Acapella device. At low pressures, the frequency of oscillation of Acapella was higher than those of the Flutter VRP1 and Shaker devices (P = .002). At intermediate pressure levels, the patterns were the same in comparison with low pressures, although the Acapella device showed frequencies of oscillation values lower than those of Flutter VRP1 and Shaker at low pressure (P < .001). At high pressures there were no statistically significant differences between the 3 devices regarding the frequency of oscillations (see Table 2 and Fig. 3).
There were no significant differences among mean oscillation frequencies for the Flutter VRP1, Shaker, and Acapella devices (see Table 2 and Fig. 3).
Discussion
The purpose of the present study was to evaluate the effects of the mechanical behavior of the Flutter, Acapella, and Shaker devices, using different flows, inclinations, and adjustments. Our results show that the 3 devices are reliable and produce pressure oscillations compatible with those necessary for the removal of secretions.
The development of these devices originates from the studies by King et al,18 who obtained higher values for tracheal transport velocity in animals with thoracic oscillations, ranging from 13 to 15 Hz, compared to oral oscillations.19 With regard to Flutter VRP1, in vitro studies assessed the influence of high-frequency oscillations on the properties of respiratory secretion. The results showed that such oscillations can break down the bonds of mucus macromolecules, making the mucus less thick and consequently more easily transported through the airways.20–22
These results were confirmed in patients with cystic fibrosis, with the authors demonstrating a decreased sputum viscoelasticity after therapy with Flutter, in comparison with autogenic drainage, as well as improvements in mucociliary and cough clearability.23
Flutter VRP1 was approved in the present study, and in Alves et al,15 when positioned at –30, 0, and +30 degrees of inclination, as proposed by Lindeman.10 On the other hand, this finding was divergent from that reported by Volsko et al,12 who used inclinations of 0, 20, and 40 degrees. However, the air flows in the present study (5–32 L/min) are similar to those used by Volsko et al,12 but different from those used by Alves et al,15 which ranged from 0.2 to 2.0 L/s. Due to the higher air flows, the maximum values obtained by Alves et al15 are greater than those found by Volsko et al12 and by our study. Indeed, pressure levels ranging from 10 to 20 cm H2O and oscillations between 13 and 15 Hz were obtained by the 3 studies at zero positive degrees of inclination. Another study demonstrated that, when the Flutter is used in positive inclination and with a large air flow, there occurred an increase in expiratory pressure.13
The mechanical characteristics and dynamic behavior of the Flutter VRP1 device were studied by Lépore Neto et al,11 but the air flow values used ranged from 0.55 to 2.2 L/s, lower than those found by Lindemann.10 However, apart from an air flow of 0.55 L/s, the other stipulated air flow values were greater than the rates used for the oscillating PEP maneuver. The main findings of this study were related to movements of the sphere at high air flows in which displacement was vertical, with no shock against the wall of the perforated cone of the Flutter VRP1. Additionally, at lower air flows, dislocation of the steel sphere occurs both vertically and horizontally in rotational and translational collisions with the cone wall, and a harmonious frequency modulation is produced, associated with the oscillatory frequency. Therefore, the frequency of oscillations of the sphere and harmonic modulation frequencies depended on air flow, suggesting that Flutter VRP1 may not produce the desired effects during forced expirations.
Volsko et al12 and Alves Silva et al16 also evaluated the mechanical behavior of the Acapella device. Interestingly, the present study and Volsko et al's used similar air flows, as did others authors15,16 in their studies. Nevertheless, the minimum and maximum values of PEP (4.8–15.6, 6–21, and 3–23 cm H2O) and frequency of oscillation (8–17, 13–30, and 8–21 Hz) obtained in the 3 studies are similar.
With regard to the Shaker device, its gravity-dependent mechanism is similar to that of Flutter VRP1, with the advantage of having a rotary mouthpiece that allows the patient to use the device in different positions. The results of this study showed that the mechanical behavior of the Shaker device is similar to that of Acapella, but with better linearity at higher air flows. The pressure amplitude produced by Flutter and Shaker devices was greater at low and high pressures, whereas the Acapella device also produced similar amplitude pressure but at intermediate pressure. The frequency of oscillation was higher for Flutter and Shaker devices at intermediate pressure, whereas the Acapella device had similar frequency oscillation at lower pressure. The levels of PEP produced by the 3 devices were not different, regardless of the experimental pressures. Although the pressure and frequency of oscillation can reach values suitable for removal of secretions, the loss of linearity suggests that patients are not instructed to perform forced exercises.
In Brazil, the Flutter, Acapella, and Shaker devices cost, respectively, $437.50, $98.99, and $31.25. As their mechanical behaviors are reliable, price may be a criterion for acquiring the most suitable device.
We believe that this study is important because the behaviors of HFOs were analyzed at air flows compatible with their clinical use. Thus, it would also be possible to suggest that they could be adequate and safe for adults with increased airway secretions. In some studies, authors used air flow values significantly greater than those normally used in clinical practice,10,11,14 which justifies a more detailed study of the mechanics of these devices.
Children with moderate to severe cystic fibrosis treated with oscillating PEP obtained expiratory flow of 13–24 L/min. Healthy adults submitted to this maneuver showed expiratory flow of 18–37 L/min.12 The oscillating PEP maneuver consists in making the patient take a breath with a volume greater than the tidal volume, but without reaching total lung capacity, and then performing a non-forced expiratory activity without surpassing the functional residual capacity.24
These characteristics are more evident for angles of 0° and +30°. All air flow levels were relative to the lowest point of oscillatory pressure. The Flutter VRP1 and Shaker devices maintained their positive pressure during the entire expiratory procedure for the experimental air flow levels, even with oscillations of the stainless steel sphere inside the perforated cone. This effect was enhanced with increased resistance to the expiratory flow, increased PEP, and decreased pressure amplitude, all maintaining the inferior oscillatory pressure above baseline, or zero.
With regard to the HFO, it was noted that at low pressures all 3 devices, particularly the Acapella, could generate values allowing an easy transport of mucus within the airway. The Flutter VRP1 and Shaker devices showed low-pressure levels smaller than that of the Acapella device, which, on the other hand, showed values closer to those favoring better transport of mucus at all air flows.24–26 Therefore, at low pressure the use of both Acapella blue and green devices was more appropriate to facilitate mucus transport, compared to the other 2 devices. At the intermediate pressure level, the Flutter VRP1 and Shaker devices demonstrated similar HFO values at all air flows. The Flutter VRP1 and Shaker devices showed oscillation frequencies above the optimal point for mucus transport at air flows of 20, 26, and 32 L/min for the former and of 26 and 32 L/min for the latter.15,18 Therefore, with HFO levels lower than those of the other 2 devices, both Acapella devices operated at oscillation frequencies within the acceptable range, to ease transport of bronchial mucus at all air flows. Expectoration can be optimized if the pressure coincides with ciliary movement range25 or respiratory resonance frequency.11
A study of Flutter VRP1 concluded that positive inclinations optimize positive expiratory pressure and flow-amplitude effects, and, consequently, the mobilization of secretions.15 Another important study described that when the Flutter is used in positive inclination and with a large air flow there was an increase in expiratory pressure.13 These 2 devices also had frequency values within the acceptable range for the best transport of bronchial mucus at air flows of 5–15 L/min. Consequently, for air flow up to 15 L/min, all 3 devices are appropriate for clinical use with respect to frequency of oscillations.
It is important to emphasize that in the present study a continuous air flow was used in the experimental model, and the results should be interpreted judiciously, as the clearance rate by airway oscillation is determined by the interaction between air flow, time, the device's oscillations, the airway's oscillations, and displacement during inspiration and expiration.27
Conclusions
The Flutter VRP1, Shaker, and Acapella devices can produce the pressure and oscillation that are recommended to help the transport of respiratory secretions. Flutter VRP1 and Shaker had a performance similar to that of Acapella in many aspects, except for the PEP variable. Further studies are necessary, mainly regarding clinical resources for respiratory interventions.
Footnotes
- Correspondence: Eliane Maria de Carvalho PhD, Curso de Fisioterapia, Universidade Federal de Uberlândia, Avenida Jeronimo Maia Santos 95, Apto 101, Santa Maria, Uberlândia, Minas Gerais 38408–014, Brazil. E-mail: elianemc{at}faefi.ufu.br.
The authors have disclosed a relationship with Intermed Equipamento Médico Hospitalar, which provided the ventilators used in this study. The authors have disclosed no other conflicts of interest.
- Copyright © 2013 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}