

Abstract
BACKGROUND: The utilization of respiratory therapist (RT) driven protocols for single interventions, such as oxygen titration and bronchopulmonary hygiene, and protocols consisting of multiple interventions have been associated with improvements in resource utilization. Based on this, we started a quality improvement project to transition the delivery of respiratory care services from physician-ordered treatments to RT-driven protocols. During the first phase of our quality improvement project, we compared the frequency of bronchodilator administration and its associated costs, between a physician-ordered bronchodilator strategy and a RT-driven bronchodilator protocol strategy.
METHODS: This was a retrospective analysis of prospectively collected data obtained during the initial phase of a quality improvement project. Over a period of 2 weeks, RTs administered physician-ordered bronchodilator treatments. During this time they assessed the subjects' clinical status and what they would have recommended in regard to bronchodilator treatment frequency following an RT-driven protocol.
RESULTS: Forty-eight subjects were ordered bronchodilator treatments, which resulted in 88 assessments. The utilization of a protocol would have resulted in 42 (47.7%) bronchodilator orders administered “every 6 hours, as needed,” and 27 (30.6%) orders administered “every 8 hours,” compared with 2 (2.2%) and 2 (2.2%), respectively, in the physician-ordered group (P < .001). Conversely, physician-ordered treatments were prescribed “every 4 hours” in 56 (63.6%) cases, compared with 10 (11.3%) in the RT-driven protocol group (P < .001). Total bronchodilator therapy cost in the physician-ordered group was $1,672.85, whereas it would have been $904.53 in the RT-driven one. Per patient costs were $19.0 ± 6.9 in the physician-ordered group, and would have been $10.3 ± 9.4 in the RT-driven bronchodilator protocol group (P < .001).
CONCLUSIONS: The application of an RT-driven bronchodilator protocol can hypothetically reduce the frequency of bronchodilator treatments, compared with a physician-ordered strategy, resulting in a theoretical reduction of costs in patients who require bronchodilator therapy.
Introduction
Over the last few years, the healthcare system has been experiencing important changes. Particularly, discussions have been focusing on specific concepts such as effectiveness, efficiency, and quality improvement (QI). In respiratory care these goals are achieved through standardization of therapies: specifically, utilizing respiratory therapist (RT) driven protocols. This strategy has already demonstrated optimal outcomes, improvement of resource utilization, and higher concordance with recommended standards of care.1 Several studies have demonstrated that misallocation of therapy represents an area of greatest concern, with a prevalence of over-ordered and under-ordered respiratory treatments as high as 72% and 21%, respectively.2,3 The impact of the previously described misallocation carries important economic consequences. Direct and indirect costs are increased due to ordered but not indicated therapies, and due to poor outcomes related to missing and delayed treatments. Previously published studies have focused on protocols addressing single interventions, such as oxygen titration4 or bronchopulmonary hygiene,5,6 as well as protocols consisting of multiple and simultaneous interventions (ie, oxygen titration, bronchopulmonary hygiene, hyperinflation therapy, and bronchodilator treatments).7–10 Studies addressing the benefits of bronchodilator protocols (as a single intervention) are lacking.11
Based on this reality, the Respiratory Care Department at Creighton University Medical Center conducted a QI project designed to transition the delivery of respiratory care from physician-ordered treatments to RT-driven protocols. The first phase of this QI project was devoted to the development of protocols. A described set of protocols designed at the Cleveland Clinic years ago9 was modified and adjusted according to the needs of our institution. In the second phase, RTs were educated in the utilization of an evaluation tool, which was developed to categorize patients according to their level of severity. They were also trained in the interpretation and application of algorithms contained in the aforementioned protocols. During this period, RTs administered treatments following physicians' orders. Simultaneously, they collected information regarding patients' level of severity, and used the RT-driven protocol guidelines to determine optimal treatment frequencies. This study assesses resource utilization associated with aerosolized bronchodilator therapy. Frequencies of administration of aerosol therapy and direct costs were compared between physician-ordered treatments and those treatments that would have been delivered if protocols had been utilized.
QUICK LOOK
Current knowledge
Respiratory therapist (RT) driven protocols improve resource utilization and patient care and reduce unnecessary treatments and under-treatment in selected populations.
What this paper contributes to our knowledge
Hypothetically, an RT-driven aerosolized bronchodilator protocol can reduce the frequency of therapy, compared to physician-ordered therapy. Using a quality improvement project to compare physician ordered therapy to an RT-driven protocol would have resulted in a cost savings of 46%. Implementation of this quality improvement project is necessary to determine the actual impact on costs and patient outcomes.
Methods
This was a retrospective analysis of prospectively collected data obtained during the initial phase of a QI project. It was exempt from review by the Creighton University Medical Center institutional review board. This phase of the project included patients admitted in the general ward at Creighton University Medical Center from January 15 to January 31, 2012. All subjects, independent of the admitting diagnosis, were deemed eligible. Patients admitted to the ICU were excluded.
RTs collected demographic information, admitting diagnosis, type of aerosolized bronchodilator ordered, system of delivery (nebulization vs metered-dose inhaler [MDI]), and frequency of administration. Data were collected on a daily basis, as long as respiratory care services were requested. Simultaneously, RTs evaluated subjects according to an evaluation tool (Fig. 1). This instrument permits categorization of subjects according to their level of severity. A level of 1 implies high severity and/or instability, whereas a level of 5 indicates low severity and clinical stability. Once a level of severity was assigned to the subject, the frequency of aerosol treatments was determined according to a predefined chart that associates levels of severity with frequencies of treatments (Fig. 2). Of note, even though the protocol includes criteria for the selection of bronchodilator delivery mode (ie, MDI vs small-volume nebulizer), the primary goal of this first phase of the QI project was focused on bronchodilator frequencies and their resulting costs. Therefore, we assumed the delivery mode would remain unchanged from what was originally ordered by the physician and only the treatment frequency would vary.
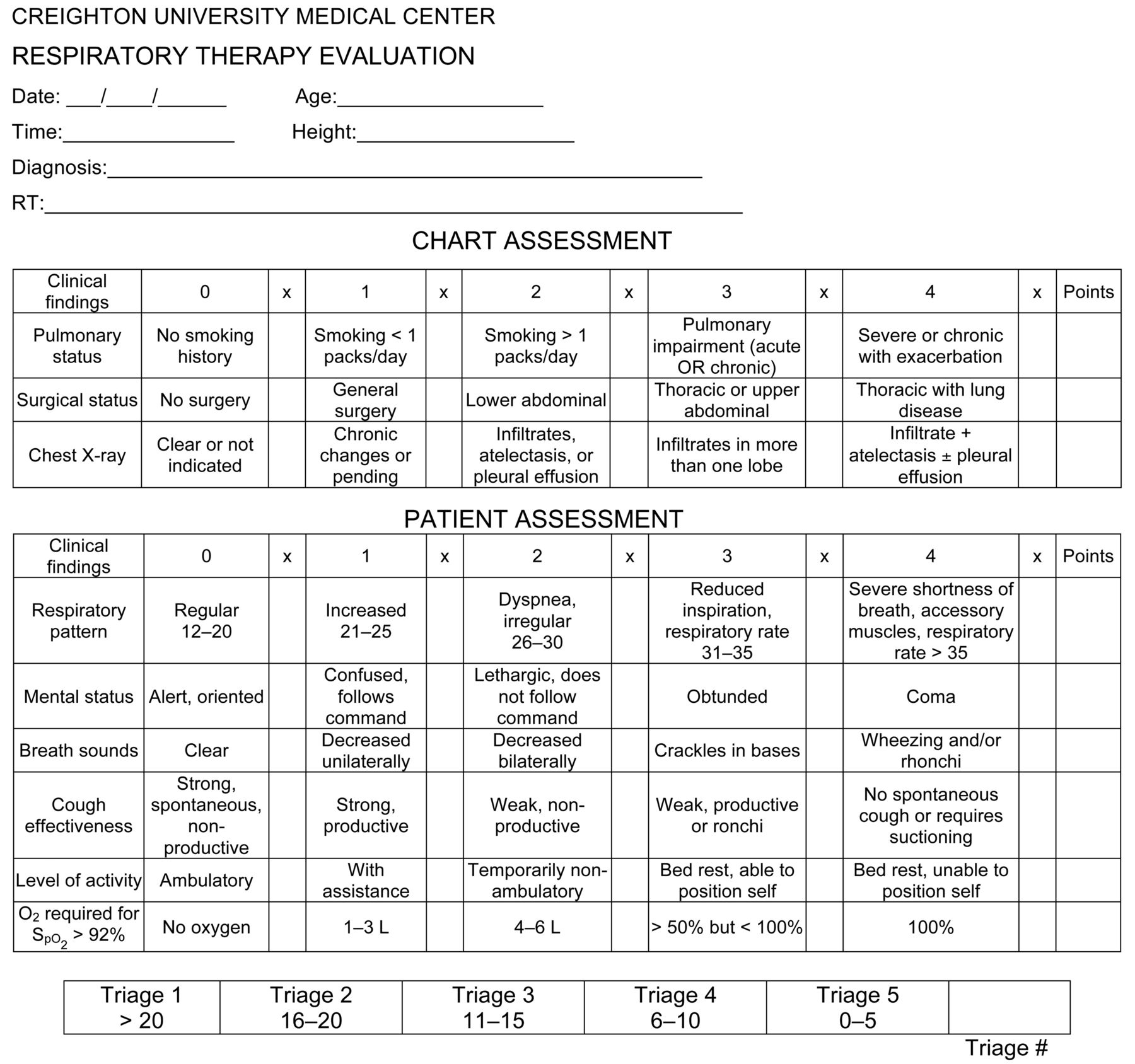
Respiratory therapist evaluation tool to adjudicate levels of severity.
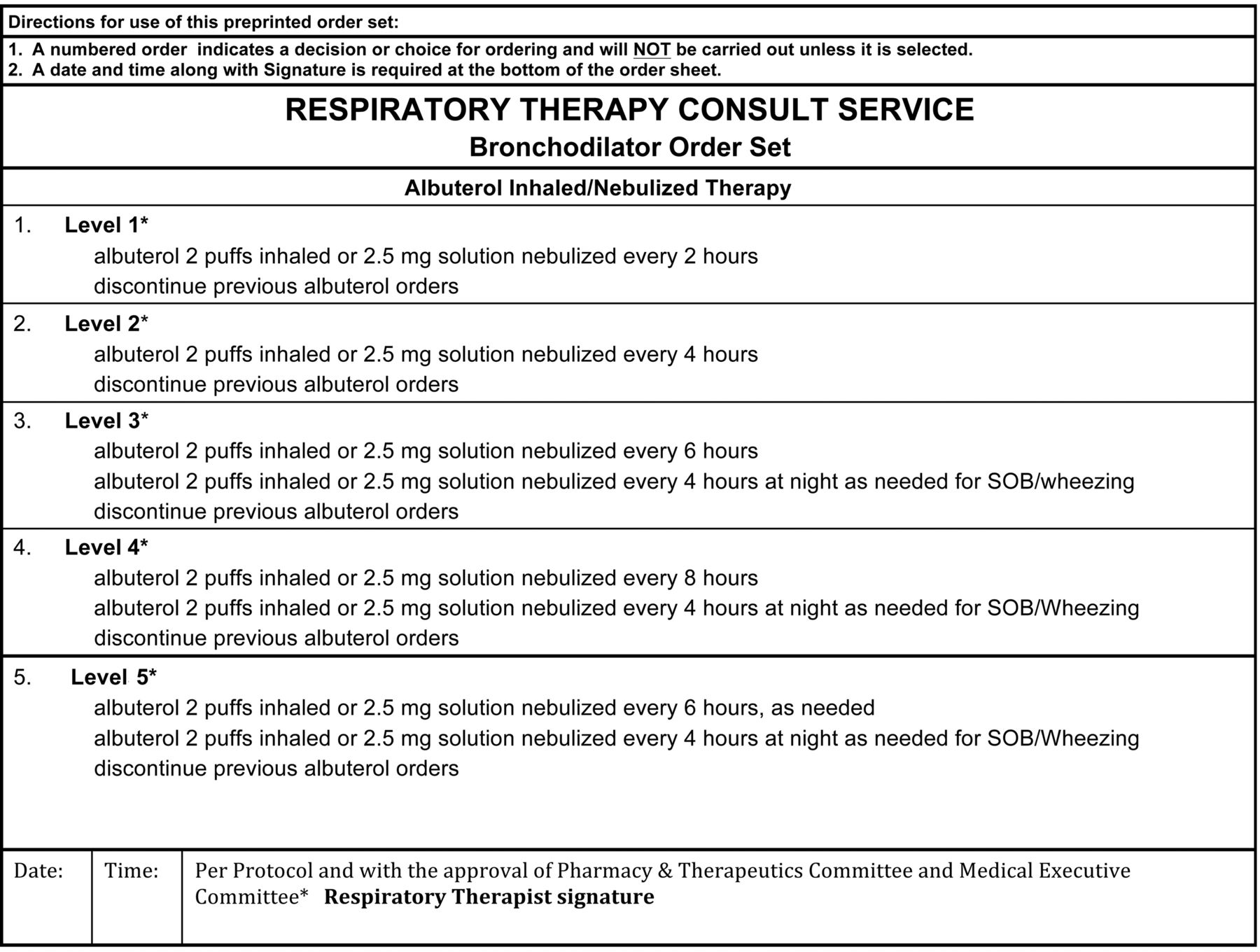
Form utilized at Creighton University Medical Center to administer bronchodilator treatments according to levels of severity. SOB = shortness of breath.
Cost of bronchodilator therapy was calculated as the sum of RT labor cost, plus hand-held nebulizer device, aero-chamber, and bronchodilator medication costs. Labor and device costs were obtained from the respiratory therapy department, whereas contractual costs for Creighton University Medical Center of albuterol, ipratropium, and their combination, in nebulization vial, as well as in MDI form, were obtained from the pharmacy department. In order to calculate labor costs, the mean hourly salary of RTs working at Creighton University Medical Center was utilized as the reference. Based on the average time for delivering a nebulization treatment (10 min) with our hand-held nebulizer (Micro Mist, Hudson RCI, Research Triangle Park, North Carolina), proportional RT labor cost per treatment was calculated. MDI inhalations were assigned a 5-min period per treatment. Bronchodilator treatments administered on an “as needed” basis were not included in the cost analysis, as predicting hypothetical “as needed” treatments in the RT-driven protocol group becomes speculative.
Statistical Methods
Continuous variables are reported as mean ± SD, and percentiles. Categorical variables are reported as frequencies and percentages. the Student t test was utilized to compare continuous variables, and the chi-square statistic was used to compare categorical data. Direct costs were calculated by adding RT labor costs, hand-held nebulizers, aero-chambers, and medication costs. We used statistics software (SAS 9.1.3, SAS Institute, Cary, North Carolina) for all analyses.
Results
Forty-eight subjects were ordered to receive bronchodilator therapy during the initial QI project phase, and this resulted in a total of 88 assessments by RTs. The mean age of the subject population was 61 ±15 years, and 22 (46%) were men. Seventeen (35%) subjects were smokers, whereas 19 (39%) were former smokers. Thirty-five (72%) subjects were admitted due to cardiopulmonary diseases. Specifically, 12 (25%) subjects were admitted due to pneumonia, and 8 (17%) due to COPD exacerbation. Thirteen (28%) subjects were admitted due to a non-cardiopulmonary reason. Despite the admitting diagnosis, 42 (87%) subjects had a medical history of pulmonary disease such as COPD, asthma, bronchiectasis, interstitial lung disease, or obstructive sleep apnea. Forty (83%) subjects were chronically treated with inhaled medications. Table 1 shows the subjects' demographics, admitting diagnoses, and prior pulmonary diagnoses.
Demographic Data, Admitting Diagnoses, Chronic Pulmonary Diagnoses, and Chronic Respiratory Medications (n = 48)
Out of 88 assessments, 60 (68%) orders included aerosol treatments in nebulization form, and 28 (32%) in MDI. Albuterol, ipratropium, and the combination albuterol/ipratropium were administered on 20 (22.7%), 3 (3.5%), and 65 (73.8%) occasions, respectively. Levels of severity according to the evaluation tool were determined for each subject on a daily basis. Six (7%) subjects were categorized as level 1 (high severity), 10 (11%) as level 2, and 30 (34%), 34 (39%), 8 (9%) as levels 3, 4, and 5 (low severity), respectively. Table 2 shows the frequencies of bronchodilator therapy comparing physician-ordered treatments to RT-driven protocol. Interestingly, the most common order among physicians was bronchodilator therapy every 4 hours, which represented 56 (63.6%) out of 88 bronchodilator orders. Only 10 (11.3%) orders would have been prescribed with this frequency in the RT-driven protocol group (P < .001). The utilization of the RT-driven protocol would have resulted in 42 (47.7%) bronchodilator orders administered “every 6 hours, as needed,” and 27 (30.6%) orders administered “every 8 hours.” These same frequencies were utilized in 2 (2.2%), and 2 (2.2%) orders, respectively, in the physician-ordered bronchodilator group (P < .001).
Frequency of Bronchodilator Treatments: Physician-Ordered Versus Respiratory Therapist-Driven Protocol
Concordance between physician-ordered treatments and protocol-driven treatments was assessed. Notably, there were only 12 (13.6%) instances of concordance. Conversely, discordances were seen in 86.4% of all orders. Protocol-driven treatments would have provided more frequent bronchodilator treatments than physician-ordered ones on 7.9% of occasions. On the other hand, RT-driven protocol orders would have provided less frequent therapies in 78.5% of the cases.
Table 3 shows direct costs associated with bronchodilator treatments in the physician-ordered versus RT-driven protocol group. Briefly, total costs in the physician-ordered group were U.S.$1,672.85, whereas they would have been $904.53 in the protocol-driven group. Per subject costs were $19.0 ± 6.9 in the physician-ordered bronchodilator treatment group, and they would have been $10.3 ± 9.4 in the RT-driven bronchodilator protocol group (P < .001). The application of an RT-driven bronchodilator protocol would have reduced the full-time employee need by 0.38 units (from 1.0 to 0.62 full-time employees). Furthermore, estimated annual cost savings with the application of the RT-driven bronchodilator protocol (assuming no significant change in outcomes) could be up to U.S.$18,440.
Bronchodilator Therapy Costs: Physician-Ordered Versus Respiratory Therapist-Driven Protocol
Discussion
The present study yields the following conclusions. The application of an RT-driven bronchodilator protocol can hypothetically reduce the frequency of bronchodilator treatments, compared with a physician-ordered strategy. The cost of providing bronchodilator therapy may theoretically be reduced when RT-driven protocols are utilized. Concordance between the frequency of physician-ordered treatments and the frequency of treatments suggested by a bronchodilator protocol is poor.
A report by the Institute of Medicine defined quality of healthcare as a combination of 6 domains, calling for healthcare to be safe, effective, patient-centered, timely, efficient, and equitable.11,12 In order to achieve quality as mentioned, multiple healthcare societies have been supporting the application of protocols.13,14 Protocols permit standardization of algorithms for patient care. Their application reduces variability of care, and guarantees that evidence-based proven therapies are delivered. The first time the term “respiratory care protocol” was utilized was in 1981.15 In this paper the authors described the use of algorithms for the application of therapeutic modalities related to respiratory care. Ever since, numerous publications supported their use, as protocols showed improvement in the allocation of respiratory care services.1,16,17 The concepts of “allocation” and “efficiency” are intrinsically related. According to prior studies, misallocation by over-ordering respiratory care services ranges from 32% to 72%.2,5,7,18 On the other hand, the rate of under-ordering respiratory treatments ranges from 7% to 21%.3,19 Consequently, increased costs due to delivery of unnecessary treatments, and those related to poor outcomes associated with under-treatment become an undesirable reality. The experience with the Respiratory Therapy Consult Service at the Cleveland Clinic, which included the implementation of an RT-driven protocol for titrating supplemental oxygen in postoperative patients, showed a shortening of the total duration of oxygen therapy (due to better allocation) and produced concomitant cost savings of $21.73 per patient, with an estimated annual cost savings of $263,346.1,4,17 Another observational study, which focused on the utilization of protocols for bronchopulmonary hygiene therapy, revealed that protocols resulted in a 61% reduction of bronchopulmonary hygiene therapy outside the ICU, with concomitant cost savings of more than $250,000.5 No adverse events were identified in any of the previously described studies. Nevertheless, the strongest evidence of the effectiveness of RT-driven protocols comes from 2 randomized controlled trials published by Stoller and Kollef.
Stoller et al9 conducted a randomized controlled trial in which 145 adult non-ICU patients at the Cleveland Clinic were randomized to receive respiratory care orders as placed by physicians, or to have treatments delivered based on RT-driven protocols. Importantly, algorithms contained in these protocols were based on clinical practice guidelines developed by the American Association for Respiratory Care. The strategy based on RT-driven protocols conferred several advantages, which included a higher concordance with a gold standard respiratory care plan (82% vs 64% using stringent agreement criteria, P < .001), and a trend toward lower median respiratory care cost per patient ($130 vs $152, P = .51), although this was not statistically significant.
The randomized controlled trial published by Kollef et al10 allocated patients to 3 different firms (A, B, and C). Firm A delivered treatments based on a RT-driven protocol, whereas patients in firms B and C received respiratory care based on physician orders. Notably, firm A required fewer respiratory therapy treatments (A 10.7, B 12.4, and C 12.3, P = .009), and had greater percentage of bronchodilators administered via MDI (A 89%, B 77%, C 78%, P = .01). Furthermore, RT-driven protocols had lower mean respiratory care charges (A $868, B $1,124, C $1,054, P < .001).
More recently, a study performed at the University of Pittsburg Medical Center evaluated a before-and-after initiation of an RT-driven protocol in neurosurgery and trauma step-down units, and trauma/surgery general wards.8 The application of this strategy resulted in an increased number of respiratory treatments, despite the fact that most patients included in this study were deemed to have low risk of pulmonary complications. This finding has not been seen in prior trials, and is notable because hospital stay was reduced after the implementation of the RT-driven protocol.
Based on the aforementioned evidence, and in order to evaluate and improve our local routine care, we committed to a QI project to change the way respiratory care is delivered in our hospital. After a training phase, which consisted of following physician-ordered treatments and simultaneous documentation of bronchodilator therapy frequencies that would have resulted with the application of a protocol, we assessed economic outcomes, frequency of bronchodilator delivery, and concordance of treatments. Direct costs, composed of RT labor, hand-held nebulizers, aero-chambers, and medication costs, would have been lower with bronchodilator treatments delivered according to protocol guidance. Furthermore, the frequency of bronchodilator treatments would have been reduced with the application of this strategy. These results are in concordance with those reported in the previously mentioned studies, which consistently revealed that stratification of patient severity permits better allocation of resources and higher concordance with standards of care. Strikingly, we found discordance between physician-ordered and protocol-driven treatments in 86.4% of bronchodilator orders. Specifically, physician-ordered treatments were most frequently prescribed on an every-4-hour basis (63.6% of the cases), despite the fact that only 10 (21%) of the subjects were admitted with an exacerbation of obstructive lung disease (asthma or COPD). Therefore, the application of RT-driven bronchodilator protocols may not only improve resource allocation, but also translate to a better understanding of indications (or lack of indications) for bronchodilator therapy in specific pulmonary conditions.
Despite the previously described positive findings, our study presents several important limitations. First, we do not know whether clinical outcomes would have been the same, better, or worse with the utilization of RT-driven protocols. Based on prior studies, it is unlikely that clinical outcomes would have been worse. Nevertheless, this remains a speculative assumption, and comparison of clinical outcomes before and after the implementation of our QI project will be needed. Second, treatments ordered on an “as needed” basis were not included in the cost analysis. Predicting potential “as needed” bronchodilator treatments in the RT-driven protocol group was not feasible, due to the study methodology. However, we recognize that the number of potential “as needed” treatments in the RT-driven protocol group could completely alter our cost assessment. Third, the evaluation period was only 2 weeks, leading to a relatively small number of subjects and assessments. A larger number of subjects could increase or decrease our calculated costs, as well as the percentage of discrepancies between strategies. Last, due to our study design, the study compares physician practices with an arbitrary RT algorithm regarding bronchodilator frequency. A likely bias is compounded by the RTs' knowing the frequency of physician-ordered bronchodilator use and their awareness that a study was being performed, introducing a Hawthorne effect that would further bias RTs to conservative assessments. Furthermore, if the RTs were observing subjects and developing their care plans some time after the physicians' orders were implemented, the RTs would be observing the subjects' stability on the physician-ordered frequency, which would naturally drive them to favor less frequent subsequent bronchodilator use.
Conclusions
In summary, the first phase of our QI project revealed that the application of an RT-driven bronchodilator protocol might hypothetically reduce costs, as well as frequency of treatments, compared with a physician-ordered treatment strategy. Further analysis of economic and clinical outcomes utilizing a before-and-after QI project implementation will be accomplished in the near future.
Footnotes
- Correspondence: Ariel Modrykamien MD, Pulmonary, Sleep, and Critical Care Medicine Division, Creighton University School of Medicine, 601 North 30th Street, Suite 3820, Omaha NE 68131. E-mail: arielmodrykamien{at}creighton.edu.
The authors have disclosed no conflicts of interest.
See the Related Editorial on Page 546
- Copyright © 2013 by Daedalus Enterprises









{kind=link}
{kind=link}