

Abstract
BACKGROUND: The introduction of reduced respiratory care may lead to worse long-term outcomes for patients undergoing prolonged mechanical ventilation (PMV) for more than 21 days. The objective of this study was to determine the survival for an integrated system of reduced intensive respiratory care (ISRIRC) by the Taiwan Bureau of National Health Insurance, in patients requiring PMV.
METHODS: A 10-year retrospective study was performed in a 1,000-bed teaching hospital in Taiwan. A total of 633 consecutive PMV patients transferred from the hospital between 1998 and 2007 were enrolled. Medical records were reviewed to collect the clinical data, which were linked to the National Death Certification Database to ascertain subject survival. Kaplan-Meier estimates were performed, and a Cox proportional hazards model was constructed. We further conducted a corroboration study and retrieved a systematically randomized nationwide sample of PMV subjects with combined septicemia and shock, and compared the survival functions of those who were treated before and after the integrated system, including 228 and 2,677 subjects, respectively.
RESULTS: The survival rates at 3 months, 6 months, and 1 year were 60.0%, 44.0%, and 30.0%, respectively. The 1-year survival rates of the subjects before and after ISRIRC were 21.0% and 37.2%, respectively (P = .04). The factors associated with better survival were younger age, absence of cirrhosis, and establishment of the ISRIRC. A comparison of the 4-year survival in the larger random sample of PMV subjects with combined septicemia and shock before and after ISRIRC also showed a significant improvement.
CONCLUSIONS: With the improvement of PMV technology in the early 2000s, the establishment of ISRIRC seems to be associated with an improved survival rate for subjects under PMV.
- survival
- respiratory care
- health services
- healthcare delivery
- long-term acute care
- prolonged mechanical ventilation
- elderly patients
Introduction
Advances in acute critical care supporting and treating patients in ICUs have resulted in the emergence of patients requiring prolonged mechanical ventilation (PMV). The continued intensive service to PMV patients is a specialized area of critical care medicine.1,2 PMV has been defined as the need for mechanical ventilation in excess of 21 days and for 6 or more hours per day.3,4 The number of ICU patients requiring PMV ranges from 3% to 10%, with these patients accounting for an estimated 37–40% of ICU resources.5–7 The number of patients requiring PMV has increased and is projected to increase further. Previous studies reported that the 1-year survival rates for patients on PMV were poor, as they were between 18.0% and 38.0%.8–13 Several prognostic factors among these PMV patients were identified, including comorbidity with diabetes, renal replacement therapy, laboratory variables of hypoalbuminemia and low mean hematocrit, facilities, and the cost of care.14,15
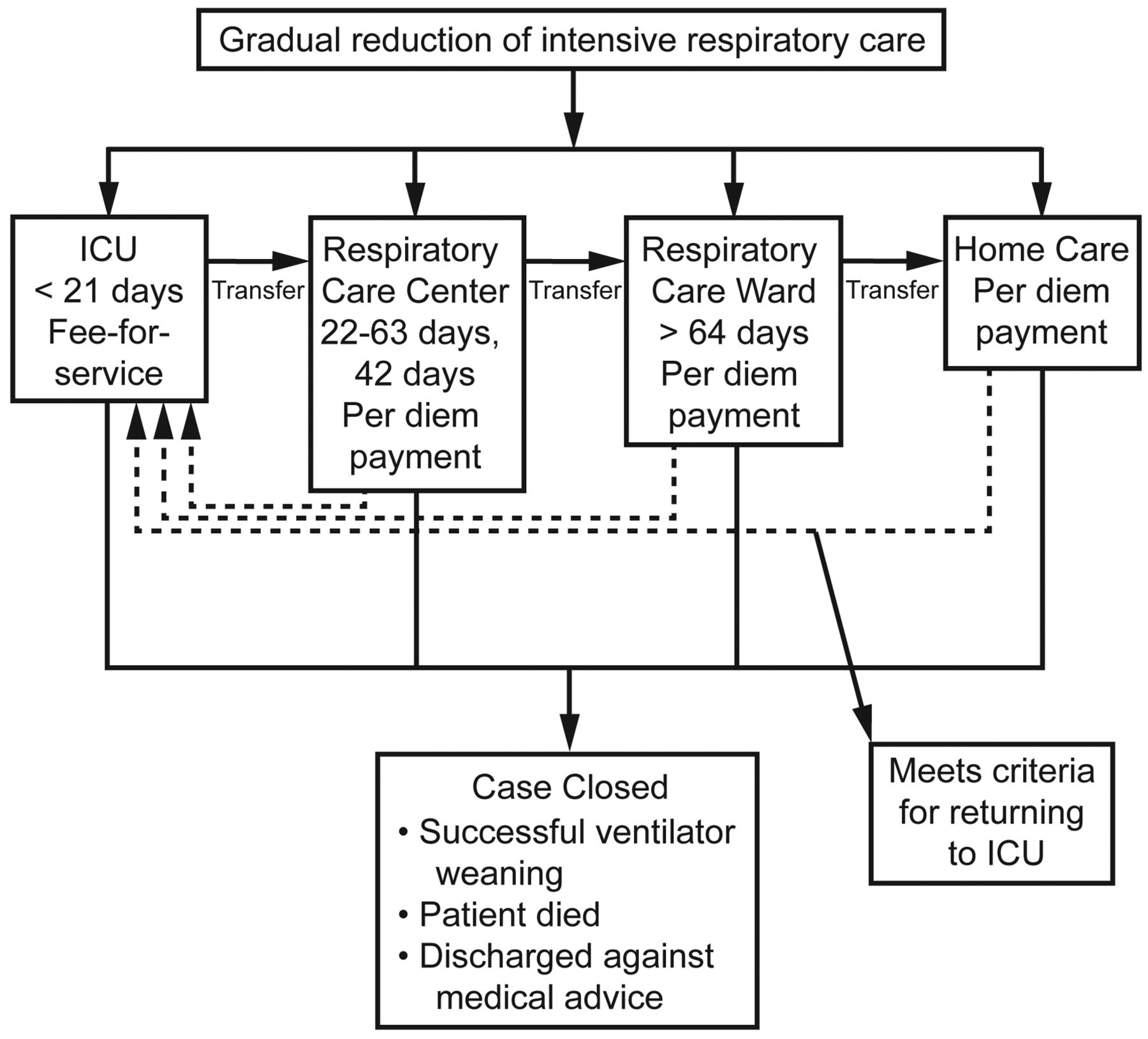
The National Health Insurance in Taiwan covers more than 96–99% of Taiwanese individuals and their medical services and is a single-payer system with global budgeting. Because patients with PMV were considered to be suffering catastrophic illnesses, co-payment was waived (ie, all PMV patients were treated in the ICU). By the end of the twentieth century, this care pattern caused a severe shortage of ICU capacity because of the ever-increasing numbers of PMV patients congesting the ICU settings. To help ameliorate this congestion, the Bureau of National Health Insurance started an integrated system of reduced intensive respiratory care (ISRIRC) in 2000. This program introduced respiratory care centers (RCCs) and respiratory care wards (RCWs) to provide both a gradual reduction of intensive respiratory care to patients with PMV and careful monitoring of the quality of care (Fig. 1). In brief, adult patients (> 17 years old) in the ICU receiving mechanical ventilation for more than 14 days are enrolled in the ISRIRC system, which guarantees the care resources in an ICU for the first 21 days, followed by transfer to an RCC for a maximum of 42 days of specialized respiratory care with weaning training, and further transfer to an RCW and/or home care services. To secure the quality of care, RCCs/RCWs must be staffed by multidisciplinary integrated teams of chest and critical care physicians, nurses, respiratory therapists, dietitians, and social workers (Table 1). Such a design can manage PMV patients at a reduced per diem while simultaneously saving many ICU wards for other acute care services.16
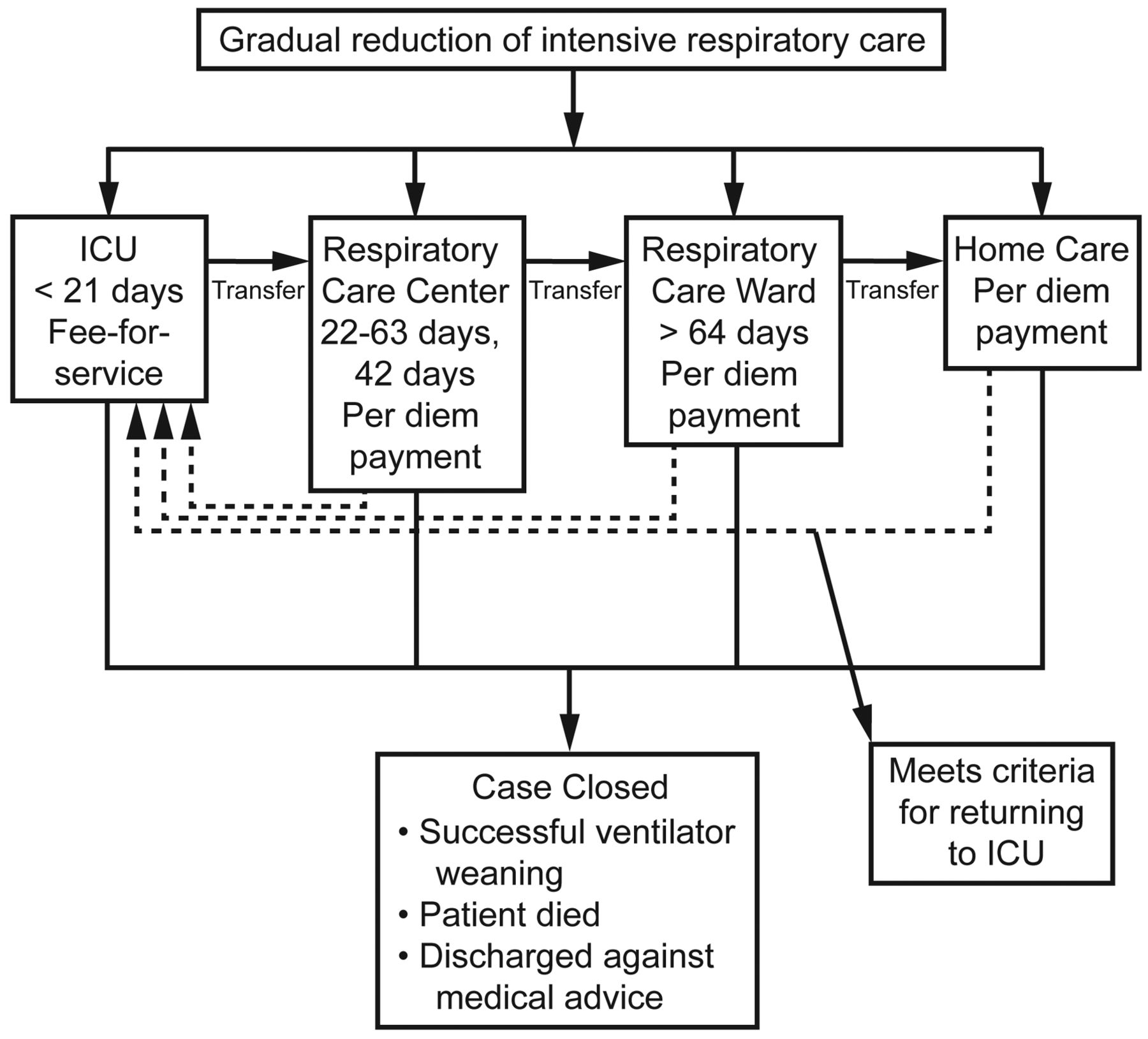
Integrated system of reduced intensive respiratory care developed by the Taiwan Bureau of National Health Insurance in 2000.
Personnel and Facilities Requirements for Respiratory Care Wards in an Integrated System of Reduced Intensive Respiratory Care
Although the ISRIRC has been regularly under careful auditing for the process of care, evaluating the final outcome to ensure the real quality of care is important. Thus, we hypothesized that the introduction of ISRIRC led to worse long-term outcomes for PMV patients. Although 2 studies evaluated the determinants of weaning for PMV patients hospitalized in RCCs, the objective of this study was to report our experience over a 10-year period with regard to final outcomes or survival for patients under the care of ISRIRC.17,18
QUICK LOOK
Current knowledge
Prolonged mechanical ventilation (PMV) is defined as a requirement for mechanical ventilation for > 6 hours a day for > 21 days. The number of post-ICU PMV patients has grown substantially over the last decade and is predicted to increase further. One challenge is placing the PMV patient in an appropriate facility.
What this paper contributes to our knowledge
In Taiwan, establishment of facilities for multidisciplinary management of PMV patients improved survival at 3, 6, and 12 months, compared to a historical control group. Survival was associated with younger age, absence of liver cirrhosis, and the establishment of the PMV facilities.
Methods
Study Populations and Data Collection
We recruited all of the PMV patients in both the pre- and post-ISRIRC eras to determine the system's potential effect on survival. From 1998 to 2007 a total of 633 consecutive PMV patients transferred from the ICU of Chia-Yi Christian Hospital in southern Taiwan (an approximately 1,000 bed teaching hospital) were enrolled after approval by the Chia-Yi Christian Hospital institutional review board (no. 098061). The study included only those PMV patients who had not been weaned.
Chia-Yi Christian Hospital is a regional teaching hospital in southwestern Taiwan with 1,000 beds and is responsible for secondary and tertiary care. There are a total of 8 adult ICU units, including 1 for coronary care, 4 for medical intensive care, 1 for burn patients, and 2 for surgical intensive care; each unit consists of 10–12 beds. Annual ICU admissions were approximately 5,500, and 30% of patients needed mechanical ventilation therapy. Among them, 5% of mechanically ventilated patients developed PMV. Chia-Yi Christian Hospital did not establish an RCC before 2009. Before the ISRIRC the PMV patients were transferred from the Chia-Yi Christian Hospital ICU to other community or local hospitals (30%), nursing homes (68%), or home care (2%). After the establishment of ISRIRC (2001–2007), the PMV patients were all directly transferred to RCWs of the regional and local hospitals because there were no RCC wards in the nearby community (Tables 2 and 3).
Demographic and Clinical Data of Prolonged Mechanical Ventilation Patients Before and After the Taiwan Integrated System of Reduced Intensive Respiratory Care
Crude and Adjusted Hazard Ratios for Prognostic Factors (n = 633)
Medical records were reviewed to abstract the clinical data at the time when the PMV subjects were transferred from the ICU of Chia-Yi Christian Hospital (meaning the time point subjects were transferred to the local hospital/nursing home before ISRIRC, and to the RCC/RCW after ISRIRC). The demographic and clinical variables of each subject were collected at the time of transfer, including age, sex, education level, smoking status, disease severity using the Acute Physiology and Chronic Health Evaluation II (APACHE II) score, Glasgow coma scale score, duration of ICU stay, comorbidity diagnoses, complete blood counts and biochemistry values, arterial blood gas analyses, tracheostomy, and mechanical ventilator setting variables. All diagnoses (including comorbidities), using the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) codes recorded by the chest physicians at transfer, were also collected. The reasons for mechanical ventilation were classified into 4 major categories: cardiopulmonary resuscitation, ventilation failure, oxygenation failure, and miscellaneous causes (eg, post-operation, trauma) at the time point of intubation recorded by the chest physicians and respiratory therapists in the ISRIRC registration system. In addition, we separated “year of transfer” into 2 groups: before the year 2000 (1998–2000), and after 2001 (2001–2007), based on the implementation of the ISRIRC.
Mortality Data of PMV Subjects
The National Death Certification Database of Taiwan was used to ascertain the dates of death for subjects who had died. We obtained the personal identification numbers of the PMV subjects and linked them to the database on January 2008 to determine mortality dates and survival functions for each subject.
Statistical Analysis
The data were collected through a coding form in a spreadsheet (Excel, Microsoft, Redmond, Washington), and were converted into data sets in statistics software (SAS 8.0, SAS Institute, Cary, North Carolina). All results are summarized into appropriate descriptive statistics. Binary and categorical variables are summarized using frequency counts and percentages. Continuous variables are presented as the means if they were normally distributed and as medians if they showed skewness. The Kaplan-Meier method was used for survival analysis. A log-rank test was used to compare differences between 2 groups (pre- and post-ISRIRC). A Cox proportional hazards model was constructed based on various subject characteristics, including age, sex, education, smoking status, laboratory values, arterial blood gas analyses, tracheostomy, mechanical ventilator setting variables, comorbidities, reasons for mechanical ventilation, and whether the care was provided before or after the establishment of the ISRIRC system.
Corroboration Study
We further conducted a corroboration study and retrieved a systematically randomized nationwide sample (1:3.4) of PMV subjects with combined septicemia and shock, and compared the survival functions of those who were treated before and after the ISRIRC system, including 228 and 2,677 subjects, respectively. The corroborative study was based in part on data from the National Health Insurance Research Database provided by the Bureau of National Health Insurance, Department of Health, and managed by the National Health Research Institutes (registered numbers 97163 and 98353). The details of how we retrieved the data were described in our previous study19 and are briefly summarized below.
The reimbursement data file obtained from the National Health Insurance of Taiwan was transformed into a research database by the National Health Research Institutes of Taiwan. These files contained detailed demographic data, and they also included information regarding the healthcare services provided for each subject, including hospitalizations, diagnoses, and intervention procedures. The data for each in-patient hospitalization included up to 5 diagnoses, which were coded according to the ICD-9. Because the government has established guidelines to restrict < 10% of all data to be drawn for research, we applied a random sample to this population with a 3.4:1 ratio and enrolled 50,481 subjects with PMV from 1998–2007. The PMV subjects with combined septicemia and shock before and after the ISRIRC system were compared for their survival functions using a Kaplan-Meier estimation and a log-rank test.
Results
More than half of the PMV subjects hospitalized in the Chia-Yi Christian Hospital were males, and more than three fourths (78.2%) were elderly (over the age of 70). Table 2 summarizes the demographic and clinical data of these subjects stratified by the year of beginning ISRIRC for comparison, indicating that the APACHE II scores and the prevalences of comorbidities of the subjects admitted after 2000 were generally higher than those admitted before that year.
Survival of PMV Subjects
Figure 2 shows the survival curves stratified by the establishment of the ISRIRC system. The survival rates of the subjects at 3 months, 6 months, and 1 year after the ISRIRC was established were slightly better than those before the ISRIRC system. However, the 2 survival curves seemed to become closer and closer after the 5th year. The 1-year survival rates of the subjects before and after the ISRIRC system were 21.0% and 37.2%, respectively (P = .04).
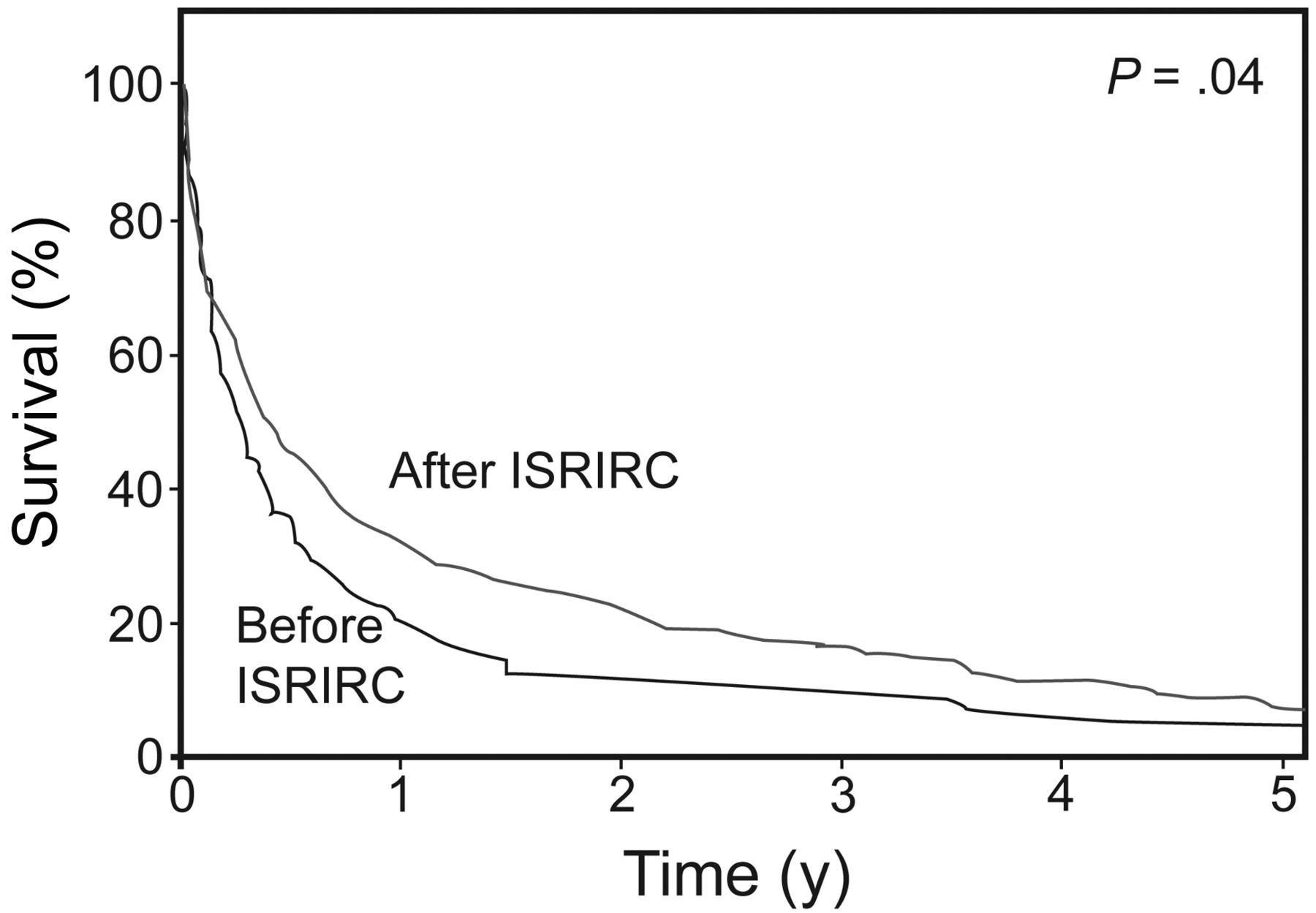
Survival curve of prolonged mechanical ventilation subjects stratified by the establishment of the integrated system of reduced intensive respiratory care (ISRIRC) in Taiwan in 2000.
Predictors of PMV Subjects
Table 3 summarizes the crude and adjusted hazard ratios with 95% CIs for the prognostic factors. Old age, hospitalization before the ISRIRC, comorbidity with liver cirrhosis, low platelet counts, and abnormal Paco2 levels were significant predictors after adjustment for all potential confounding factors. The adjusted hazard ratio for PMV subjects with liver cirrhosis was 2.39 (95% CI 1.43–4.00); for PMV subjects transferred after the year of 2000 (or ISRIRC) the hazard ratio was 0.70 (95% CI 0.53–0.93), indicating a significant reduction of mortality, compared with that before the ISRIRC. Although the crude hazard ratio for an APACHE II score of > 21 appears to increase, it did not exhibit a consistent elevation after adjustment with other risk factors. Other comorbidities, including cancer (n = 6), were not significantly associated with long-term mortality in this analysis, apparently because of small sample sizes.
Corroboration Study
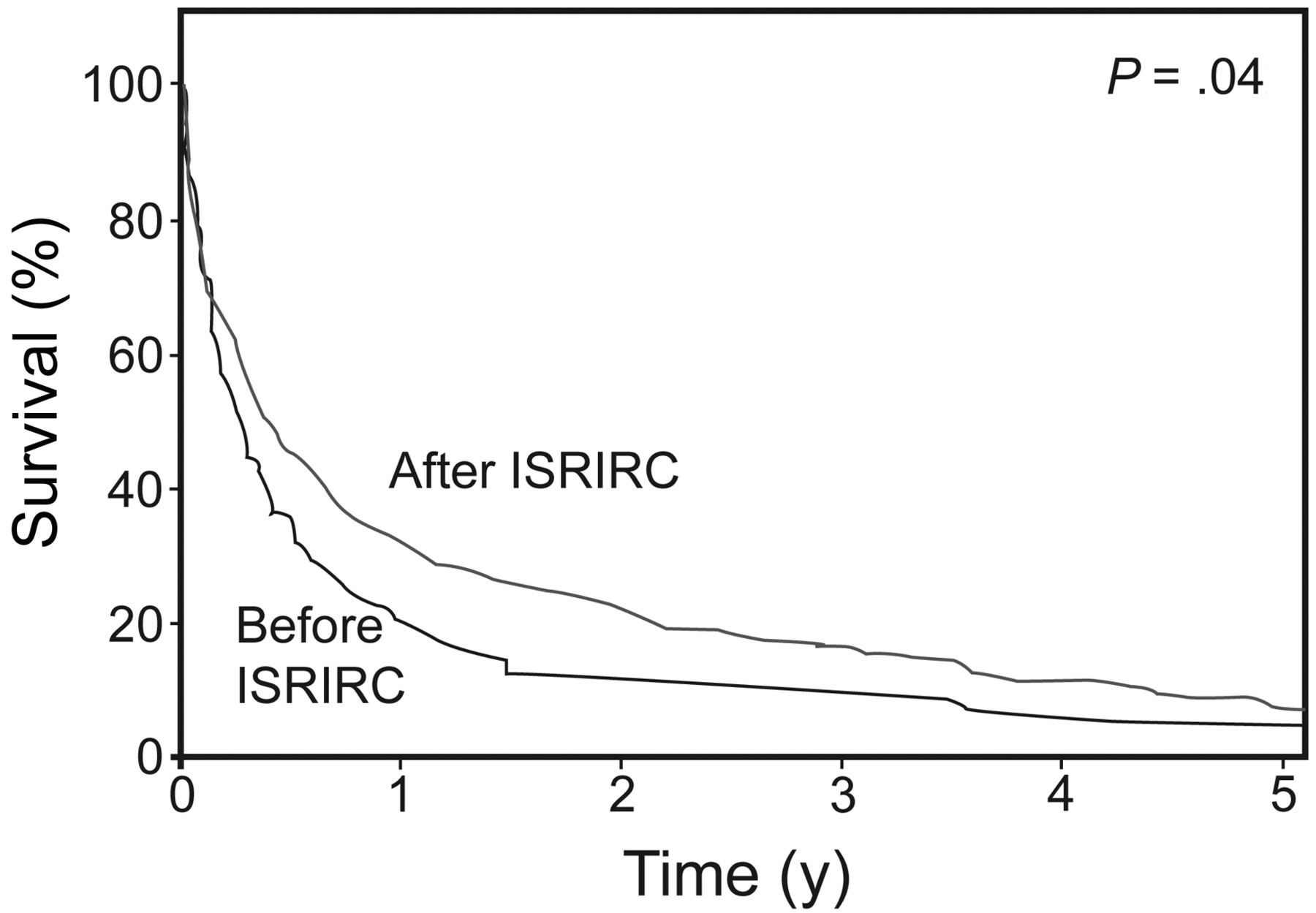
Figure 3 shows the analysis comparing the 4 year survival rates of the PMV subjects with septicemia and shock who were treated before and after the ISRIRC, including 228 and 2,677 subjects, respectively. There was a significant improvement for the subjects treated after the ISRIRC establishment compared with subjects who had been previously treated (P = .04).

Four-year survival of subjects with prolonged mechanical ventilation and septicemia and shock before (n = 228) and after (n = 2,677) the implementation of the integrated system of reduced intensive respiratory care (ISRIRC). The data were obtained from a corroboration study and from a systematically randomized nationwide sample of prolonged mechanical ventilation subjects.
Discussion
In this study we hypothesized that the introduction of the ISRIRC led to worse long-term outcomes for PMV patients. This study, which summarized the survival data for a 10-year follow-up of PMV patients in the Chia-Yi Christian Hospital and Taiwan, revealed that the ISRIRC system did not seem to increase long-term mortality. However, because association does not necessarily indicate causality, we must examine more details before making any inferences. First, there was no significant difference in the distributions of the APACHE II scores between the PMV subjects admitted before and after the year 2000, and there were increased proportions of subjects with other comorbidities, including liver cirrhosis, diabetes, hypertension, stroke, coronary artery disease, COPD, and end-stage renal disease, after the ISRIRC (see Table 2). These findings indicate that subjects hospitalized after the ISRIRC did not appear to be less severely affected than those admitted before. Second, all major risk factors were adjusted for because they were included in the construction of the Cox proportional hazard model (see Table 3). Third, our final model found that being elderly and having low platelet counts and abnormal Paco2 were major prognostic factors, corroborating the results of other previously published studies; this could be regarded as a partial validation of the results of this study.20,21
We further conducted a corroboration study and retrieved a systematically randomized nationwide sample (1:3.4)19 of the PMV subjects with combined septicemia and shock, and then compared the survival functions of those who were treated before and after the ISRIRC, which included 228 and 2,677 subjects, respectively. Figure 3 depicts the 4-year survival curves for the 2 comparison groups, and the survival of the PMV subjects seems significantly better after the ISRIRC.
In fact, the Taiwan Bureau of National Health Insurance has published a series of clinical guidelines to facilitate coordination and communication between the ICUs and RCCs/RCUs (see Fig. 1), and a continuous auditing system has been implemented to monitor such multidisciplinary care, which might help maintain a consistent quality of care. Our results corroborate the principles of a care system such as that proposed by Kim and colleagues.22 Initially, individuals (especially the family members of the PMV patients) were concerned that the transfer of a PMV patient to a less intensive care facility for chronic critical illness might affect the patient's health. For example, the 1-year trajectories of care for patients receiving PMV revealed multiple transitions of care and persistent and profound disability.23,24 Because the ISRIRC guarantees the direct backflow of PMV patients from RCCs to RCWs to home care (see Fig. 1), this regimen seemed more acceptable to the patients and their families. Our finding describes a systematic long-term care plan for PMV patients and a possible alternative to the direct transfer of such patients into a long-term acute care hospital without a suitable interdisciplinary team for continued respiratory care.
Although more than three fourths of our PMV subjects were over 70 years of age, those in reports from the United States were usually < 70 years old. Living in a Confucian culture, people in Taiwan do not give up on elderly family members, and the regulation of end-of-life care remains at a developing stage. The improvement of the 1-year survival from 21% to 37% associated with the implementation of the ISRIRC was likely still saddled with functional dependencies. The trade-off in terms of economic and social costs to achieve what may be a small improvement in survival, along with the socio-cultural factors and ethical issues, should be investigated in future studies.
Our study indicated that liver cirrhosis was a significant predictor of PMV patients, which corroborates the results reported by others.25 A possible explanation was that we recruited our subjects from a region with high prevalences of hepatitis, liver cirrhosis, and hepatocellular carcinoma.26 The Cox model assumes a multiplicative interaction among different risk factors, which implies that liver failure most likely interacts with multi-organ failure synergistically to affect mortality.27,28
There are several limitations to our study. First, because of the retrospective, single-center, and pre-post design of the study over a 10-year period, the results might not be directly generalized to other countries. Many innovations have occurred over the last decade that could improve mortality in PMV patients. As a pre-post retrospective study, there are other limitations in assessing causation, including a Hawthorne effect and regression to the mean. In addition, long-term survival may depend on the case mix. Randomized controlled trials are needed to corroborate any positive effects of the ISRIRC. Second, the data were collected only once, at the time of transfer to an RCC/RCW. Because PMV patients were generally at risk for various complications and had substantial comorbidities, future studies with repeated measurements of the risk factors may be indicated for direct tests of the hypothesis of the improved quality of respiratory care after implementation of the ISRIRC. Third, although the data on subjects' quality of life after the ISRIRC implementation were collected in another study, we were unable to retrospectively collect any such data before 2000 for comparison.29 Thus, we were unable to make any inference on this issue and the related cost-effectiveness for the ISRIRC. Simulation studies may be indicated to explore the question.
Conclusions
In conclusion, we have demonstrated that the ISRIRC, or a well coordinated, gradually reduced intensive respiratory care regimen, was associated with a slight but significant improvement in the survival rate of PMV subjects. Because the ISRIRC system actually relieves the congestion of the ICU ward, it is a viable alternative to ICU care for subjects on PMV. Future large-scale, prospective, multicenter studies may be needed to corroborate our findings.
Footnotes
- Correspondence: Cheng-Ren Chen MD, Division of Chest Medicine, Department of Internal Medicine, Chia-Yi Christian Hospital, 539 Jhongsiao Road, Chiayi City, Taiwan. E-mail: 01994{at}cych.org.tw.
This work was supported by research grant NSC-98-2314-B-705-001 from the Taiwan National Science Council, and by research grants R97-9 and R98-3 from Chia-Yi Christian Hospital. The interpretations and conclusions reported in this paper do not represent those of the Taiwan Bureau of National Health Insurance, Department of Health, or National Health Research Institutes. The authors have disclosed no conflicts of interest.
- Copyright © 2013 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}