

Abstract
BACKGROUND: Some investigations have revealed an association between depression and physical measurements of COPD patients in North America and Europe, but few related studies have been performed in Asia.
METHODS: In this cross-sectional study, 84 consecutive, stable out-patients with COPD (mean ± SD age 72.0 ± 9.0 y, percent-of-predicted FEV1 46 ± 15%, 15 [17.9%] female) in a Japanese community hospital were recruited. “Probable depression” was defined as a score of ≥ 6 on the short-form Geriatric Depression Scale (SF-GDS). Relationships among commonly used physical measurements, SF-GDS raw score, and probable depression were evaluated with the Spearman rank correlation test, multiple linear regression analysis, logistic regression analysis, and receiver operating characteristic curves.
RESULTS: Thirty-two subjects (38.1%) had probable depression. Body mass index, obstruction, dyspnea, exercise capacity index, percent-of-predicted FEV1, Modified Medical Research Council dyspnea score, 6-min walk distance, and SpO2 had: simple correlations (r 0.42–0.60, P < .001 for all) with the SF-GDS raw score; partial correlations (r 0.25–0.51, P < .05 for all) with the SF-GDS raw score after adjusting for demographic and social factors; association with probable depression in the logistic regression analysis after adjusting for demographic and social factors (P < .05 for all); and areas under the receiver operating characteristic curve of 0.72−0.84 (P < .001 for any) for probable depression.
CONCLUSIONS: Physical parameters were associated with depression in our Japanese COPD out-patients.
Introduction
COPD, defined as not fully reversible air-flow obstruction,1 is now the fourth leading cause of death in the world.2 Among the many aspects of COPD, depression is a serious concern, because it is generally associated with longer hospitalization, poor survival rate, and impaired physical and social functioning.3 Patients with depression also characteristically make fewer attempts to improve their health.4–6 Therefore, examining symptoms of depression is an important part of comprehensive COPD treatment.
The prevalence and incidence of depression among COPD patients are high, but the depression is often under-diagnosed and undertreated in these patients.7–11 Inadequate treatment for depression leads to insufficient care, poor quality of life, and premature death.12 Several risk factors are well known to predict depression in COPD patients: female,7,13 current smoking,7,12,14 poor quality of life,9,12–14 long-term oxygen therapy (LTOT),15 living alone,16 and low social status.7 Studies in North America and Europe have evaluated the association between depression and physical factors such as percent-of-predicted FEV1, 6-min walk distance (6MWD), and Modified Medical Research Council (MMRC) dyspnea score,3,13,14,16–30 but few studies have focused on the association between depression and COPD in Asians. Compared to whites, Asians generally exhibited elevated levels of depression.31,32 A study recently published in Japan reported that the prevalence of depression among COPD elderly in-patients (mean age of 72.7 y) was as high as 48.6%.33
Thus, investigations of depression in Asian out-patients with COPD are warranted. If the link between depression and commonly used physical measurements becomes clear, physicians could respond by screening such patients for depression. This would increase the rate of diagnosis and adequate treatment of depression.
This cross-sectional study evaluated the prevalence of depression and the association between depression and physical measurements such as percent-of-predicted FEV1, MMRC dyspnea score, and 6MWD, in Japanese COPD out-patients.
QUICK LOOK
Current knowledge
Depression is a common comorbidity in patients with COPD, and is associated with longer hospitalization, poor survival, and impaired physical and social functioning. Depression is under-diagnosed in COPD patients, and the research has mainly been in Europe and North America.
What this paper contributes to our knowledge
In Japanese patients with COPD, the prevalence and severity of depression were associated with the severity of lung impairment. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) COPD stage, BODE (body mass index, air-flow obstruction, dyspnea, and exercise capacity) index, percent-of-predicted FEV1, 6-min walk distance, and SpO2 were all worse in patients with depression.
Methods
The study was performed in the Department of Allergy and Respiratory Medicine, Fraternity Memorial Hospital, Tokyo, Japan, and in the Department of Internal Medicine and Clinical Immunology, Yokohama City University Graduate School of Medicine, Yokohama, Japan.
Procedure
All patients who visited the Fraternity Memorial Hospital from November 2010 to February 2011 for treatment of COPD were considered as possible study subjects. First, the investigators screened patients by reviewing their charts. Then investigators met all of the candidates and evaluated them for the inclusion criteria. Patients who satisfied the criteria and agreed to participate were then surveyed.
Study Population
The inclusion criteria were:
COPD diagnosis as defined by the Global Initiative for Chronic Obstructive Lung Disease (GOLD)1 (spirometry was newly performed at this time)
Stable medical condition, without exacerbation or infection in the preceding 2 weeks
No orthopedic problem interfering with the 6-min walk test
SpO2 ≥ 90% on ambient air
Able to safely complete the 6-min walk test
Not currently taking an antidepressant (the degree of depression may be affected by antidepressant; depressed patients not taking antidepressants were not excluded)
Absence of severe disease such as active malignancy or human immunodeficiency virus, which may influence the degree of depression.
We approached 191 patients for recruitment, of whom 107 were excluded, for the following reasons: 25 refused to participate, 23 missed appointments, 32 did not meet COPD diagnostic criteria (FEV1/FEV > 70% [n = 15]; > 12% reversibility after inhaled salbutamol [n = 15]; CT image not compatible [n = 2]), 3 had had recent exacerbations, 6 had orthopedic problems, 4 had SpO2 < 90% on ambient air, 1 was taking an antidepressant, and 3 had human immunodeficiency virus or malignancy. Some patients had 2 or more reasons for exclusion. Finally, 84 COPD patients were included in the study. We obtained written informed consent from all subjects. No subjects were on respiratory rehabilitation, as our facility does not provide that for out-patients. This study was approved by the institutional review boards at Yokohama City University Hospital and Fraternity Memorial Hospital.
Short Form of the Geriatric Depression Scale
The short form of the Geriatric Depression Scale (SF-GDS), consisting of 15 yes-or-no questions, was originally designed as a depression screening tool. A total score ≥ 6 indicates probable depression.22,34 While the SF-GDS was primarily used as a screening tool, Giordano showed that SF-GDS score correlates with the Beck depression inventory score, one of the most widely used instruments for measuring the severity of depression (r = 0.78, P < .001).35 This scale was originally developed for geriatrics but was later validated for younger adults as well.34
Measurement of Other Clinical Parameters
We selected the following clinical measurements: physical measurements of COPD, GOLD stage,1 BODE (body mass index, obstruction, dyspnea, and exercise capacity) index36 and its components, SpO2; and known demographic and social risk factors for depression among COPD patients, including age (depression is more prevalent in younger patients), sex (depression is more prevalent in females), smoking history (in pack-years), current smoking, low economic status, use of LTOT, living alone, and marital status (widowed or divorced).37
GOLD stage1 is primarily based on percent-of-predicted FEV1, and ranges from I (mild) to IV (very severe). The BODE index36 is a comprehensive prognostic index with 4 components, and the total score ranges from 0 to 10. The score of 10 indicates the poorest prognosis. The MMRC dyspnea scale score ranges from 0 to 4, with 4 indicating the severest dyspnea. Trained medical technicians performed spirometry (Autospiro AS-407, Minato, Osaka, Japan). 6MWD was obtained by standardized method38 on a 108 meter rounded track, without oxygen supplementation. The subject inhaled 1.5 mg of salbutamol via nebulizer for 20 min, and then FEV1 was measured. SpO2 was recorded with a portable pulse oximeter (Pulsox-M, Minolta, Osaka, Japan) after a 5-min resting period in a sitting position. Predicted spirogram values were based on a formula designed for Japanese subjects.39 Low economic status was defined as receiving supplemental security income from the Japanese government. This supplemental income is offered to approximately 1.5% of Japanese families.
Statistical Analysis
Data were analyzed using the unpaired Student t test, the Fisher exact test, multiple linear regression analysis, logistic regression analysis, receiver operating characteristic curve, and Cochran-Armitage test. Rank correlation was evaluated with Spearman rank correlation test, whereby r < 0.2 indicated meaningless correlation, 0.2 ≤ r < 0.4 indicated weak correlation, 0.4 ≤ r < 0.6 indicated moderate correlation, 0.6 ≤ r < 0.8 indicated strong correlation, and 0.8 ≤ r indicated very strong correlation. The ± sign always indicates standard deviation, not standard error. P values < .05 were considered statistically significant. Statistical analyses were performed with statistics software (Excel Toukei, SSRI, Tokyo, Japan, and Prism 5, GraphPad Software, San Diego, California).
Results
Eighty-four subjects met the criteria for this study; 69 were male, and 15 were female. The average age was 72.0 ± 9.0 y. Percent-of-predicted FEV1 was 45.9 ± 14.7%. Results from the SF-GDS indicated that 32 (38.1%) subjects had probable depression, while 52 (61.9%) did not. Demographic, social, and physical measurements among all subjects, subjects with probable depression (SF-GDS ≥ 6), and subjects without probable depression (SF-GDS < 6) are summarized in Table 1.40 Subjects with and without probable depression had statistically significant (P < .05) differences in economic status, LTOT use, GOLD stage, BODE index, percent-of-predicted FEV1, MMRC dyspnea score, 6MWD, and SpO2.
Subject Characteristics and Correlation With SF-GDS Depression Score
GOLD stage, BODE index, percent-of-predicted FEV1, MMRC dyspnea score, 6MWD, and SpO2 each had a significant rank correlation of r > 0.4 with raw SF-GDS score. Scatter plots for SF-GDS and 6 physical measurements are shown in Figure 1. These 6 physical measurements except for GOLD stage, which is not a continuous variable, had significant associations with raw SF-GDS score, even after adjusting for 8 demographic and social factors such as use of LTOT (Table 2).

Scatter plots of scores on the short-form of the Geriatric Depression Scale (SF-GDS) versus Global Initiative for Chronic Obstructive Lung Disease (GOLD) stage, BODE (body mass index, obstruction, dyspnea, and exercise capacity) index, percent-of-predicted FEV1, Modified Medical Research Council (MMRC) dyspnea score, 6-min walk distance (6MWD), and SpO2 in subjects with COPD. Each dot represents one subject.
Multiple Linear Regression Analysis* for the Short Form of the Geriatric Depression Scale
Probable depression significantly increased as BODE index, percent-of-predicted FEV1, MMRC dyspnea score, 6MWD, and SpO2 decreased in models adjusting for 8 demographic and social factors such as use of LTOT (Table 3).
Multiple Logistic Regression Analysis* for Probable Depression (SG-GDS Score ≥ 6)
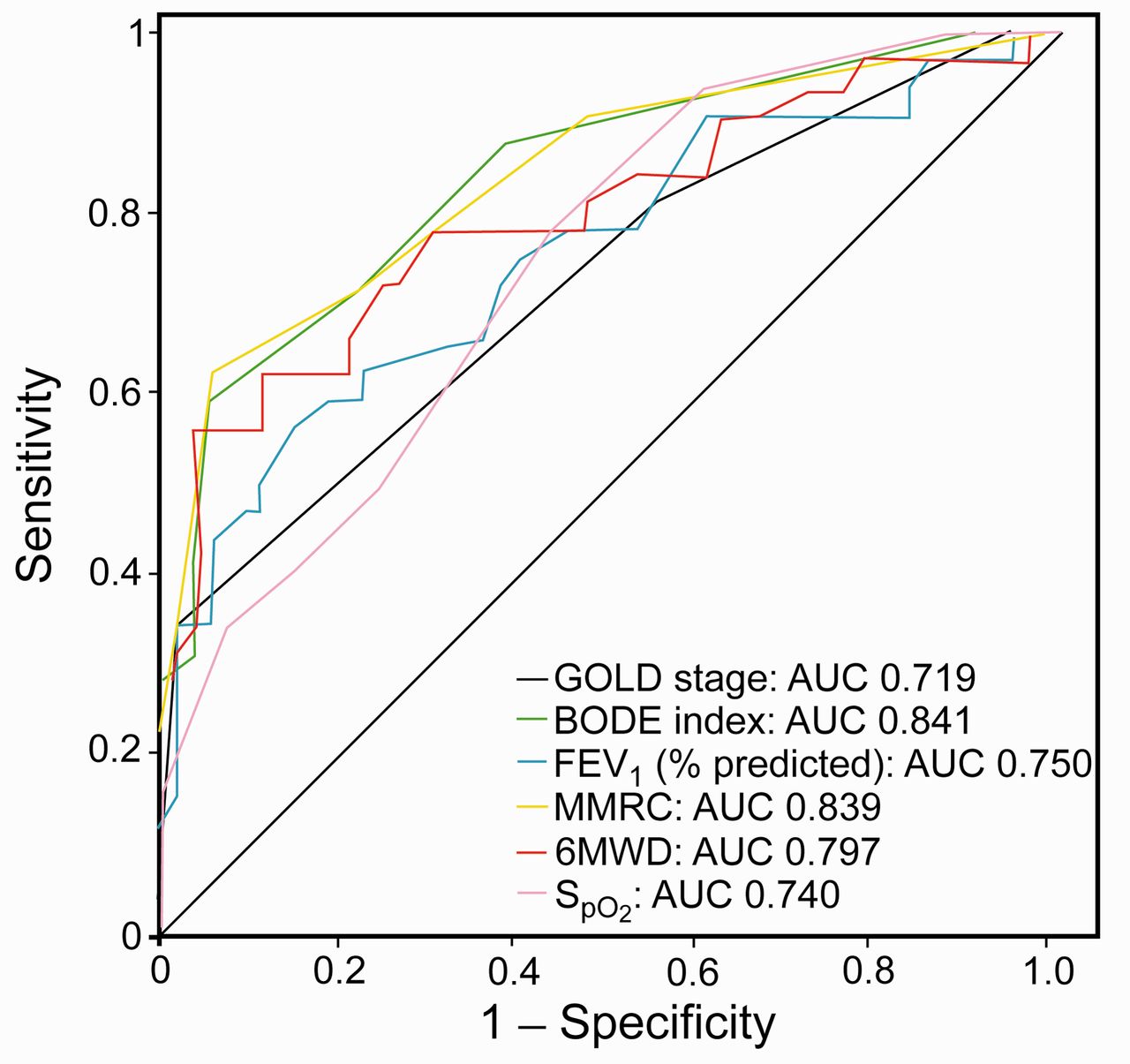
Receiver operating characteristic curves to predict probable depression by each physical factor are shown in Figure 2. The range for area under the curve was 0.719–0.841 for the 6 parameters (P < .001 for all). Receiver operating characteristic curves were allocated near the Y-axis, especially when sensitivity was < 0.3, meaning each parameter had good specificity rather than sensitivity. The 3 factors with the highest area under the curve were BODE index, MMRC dyspnea score, and 6MWD.
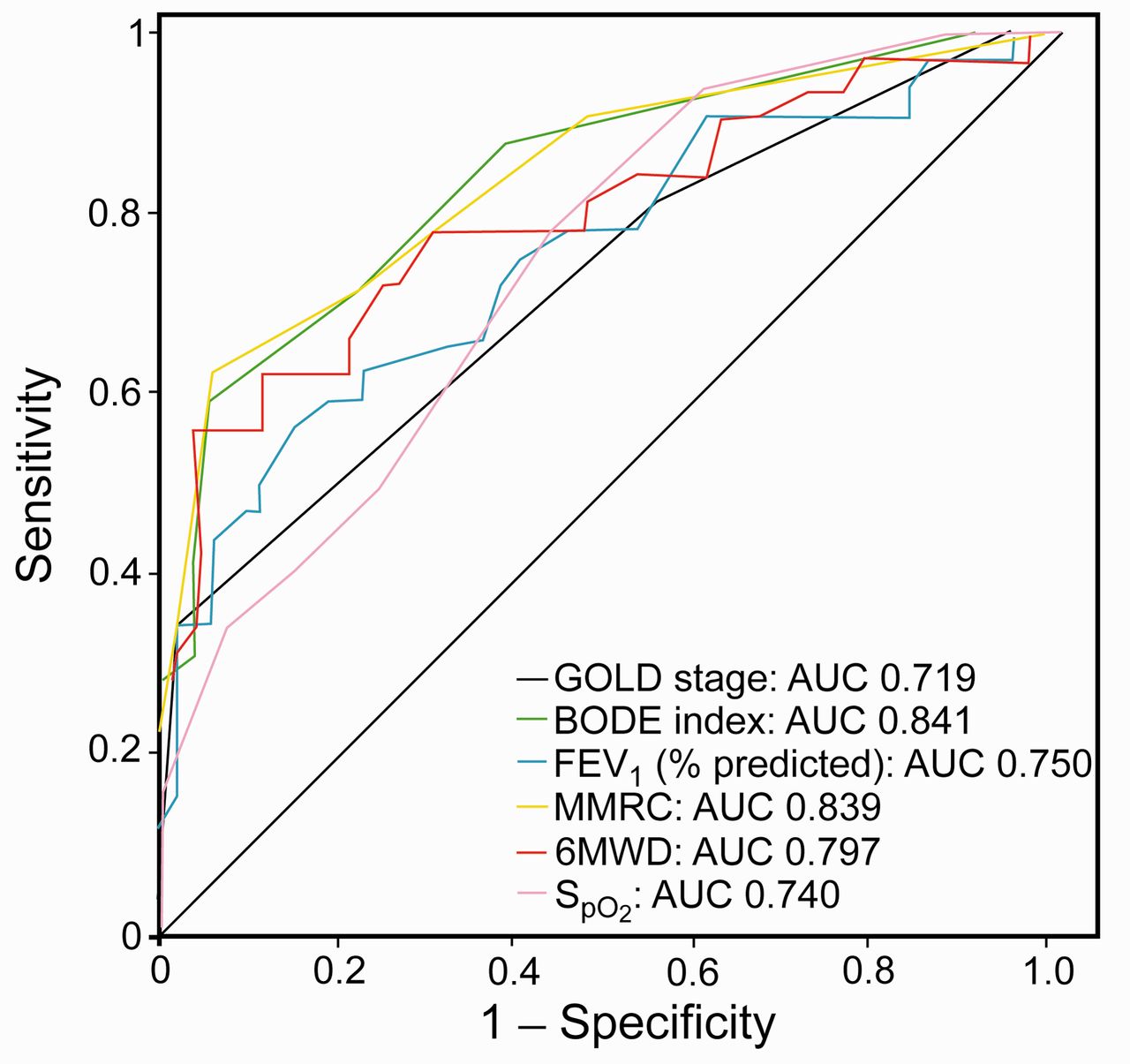
Receiver operating characteristic curves for depression versus Global Initiative for Chronic Obstructive Lung Disease (GOLD) stage, BODE (body mass index, obstruction, dyspnea, and exercise capacity) index, percent-of-predicted FEV1, Modified Medical Research Council (MMRC) dyspnea score, 6-min walk distance (6MWD), and SpO2 in subjects with COPD. AUC = area under the receiver operating characteristic curve.
The positive predictive values for probable depression were 0.73 for MMRC dyspnea score of 2.5, and 0.86 for 6MWD of 250 m.
Discussion
In the current study, the severity and prevalence of depression were associated with COPD severity measured by GOLD stage, BODE index, percent-of-predicted FEV1, MMRC dyspnea score, 6MWD, and SpO2. Previous studies evaluating the association between physical factors and depression are summarized in Table 4. The first was conducted by Light in 1985.17 Until 2007, most studies denied an association between depression and physical measurements of COPD. In contrast, most studies since 2008 have affirmed a positive association between depression and physical measurements of COPD. That lack of concordance might be owing to the wide variation in nationality, measurement tools, study design, and diagnostic criteria.41 The homogenous severity of COPD makes it especially difficult to detect a relationship. For example, most studies found a significant relationship between dyspnea and depression; however, some studies conducted with subjects who had relatively mild obstruction did not find an association.21,25 Similarly, a study of subjects who had relatively severe disease found no association between depression and physical parameters.17
Summary of Studies Evaluating the Relationship Between Physical Factors and Depression
Even though MMRC dyspnea score and 6MWD are simple parameters of COPD, their links with depression are strong. The positive predictive values in this study were 0.73 for MMRC dyspnea score of 2.5, and 0.86 for 6MWD of 250 m. If patients have worse dyspnea or limited exercise capacity, they should be screened for depression.
The associations between depression and some physical parameters are indisputable, but the interpretation is difficult. The simplest explanation is that depression is caused by COPD symptoms or limited quality of life. Another explanation is that depression makes physical signs and symptoms worse. The following evidence supports this hypothesis: subjective sensation of dyspnea increased with depression, even with normal lung function,42 and 6MWD depends on both physical and psychological factors.43,44 The other explanation is that systemic inflammation lowers both physical and mental status. There is a recent accumulation of evidence that somatic factors such as inflammation cytokines are also related to depression in COPD patients.45,46 Further research is expected to clarify the interaction between physical factors and depression.
Some possible demographic and social risk factors did not prove to be related to depression in this study. This may be because this study was not designed to investigate such relationships. Our cohort did not include enough subjects with these risk factors to research the association.
MMRC dyspnea score and 6MWD had stronger associations with depression than did percent-of-predicted FEV1 in our study. The severity of COPD has traditionally been assessed via percent-of-predicted FEV1.1 However, whether the current percent-of-predicted FEV1 grading scale is an ideal single parameter for severity of COPD has long been discussed. The importance of dyspnea and exercise tolerance has recently been emphasized, because percent-of-predicted FEV1 underestimates the importance of the extra-pulmonary manifestations of COPD.36,47,48 Our study confirmed the superiority of MMRC dyspnea score and 6MWD over percent-of-predicted FEV1.
We also measured the prevalence of depression in our Japanese out-patient cohort (38.1%). Iguchi's recent study of Japanese COPD in-patients reported a prevalence of 49%.33 It is difficult to compare prevalence in studies that vary with respect to patient background, COPD severity, depression scales, and cutoff values for depression. The prevalence of depression in Japanese patients, both our cohort and that studied by Iguchi, was greater than in patients in most other countries (see Table 4). In 1996, Mishima reported that the prevalence of depression was as low as 19%23; however, the cutoff value (10 points on the Hospital Anxiety and Depression scale) is higher than the usually used cutoff of 8 points.20 Among European countries the prevalence of depression is especially high in the United Kingdom (see Table 4).
Limitations
This study had some limitations. First, the cohort size is not large enough to warrant a solid conclusion. Second, our study design had possible selection bias, because:
More than 90% of COPD patients in Japan have emphysema. In Western countries, emphysema type is less common.
In the recruiting process, 25 patients refused to participate, and 23 were excluded because they missed their appointments in the recruitment process. This may also have caused selection bias, because depressed patients are usually less motivated to participate in this kind of study.
One patient (0.5%) was excluded because of antidepressant use.
The majority of subjects were male.
There were several confounders, such as socio-economic status.
Conclusions
In conclusion, COPD parameters including GOLD stage, BODE index, percent-of-predicted FEV1, MMRC dyspnea score, 6MWD, and SpO2 were generally associated with depression in our Japanese cohort. Dyspnea and exercise tolerance were especially important factors estimating depression.
Acknowledgments
We thank Mr Masaya Narisada and Mrs Rikako Narisada for their advice on statistics, and Mrs Yoriko Inoue for her editorial assistance.
Footnotes
- Correspondence: Takeshi Kaneko MD PhD, Respiratory Disease Center, Yokohama City University Medical Center, 4–57 Urafune, Minami-ku, Yokohama City, 232-0024, Japan. E-mail: takeshi{at}med.yokohama-cu.ac.jp.
The authors have disclosed no conflicts of interest.
Supplementary material related to this paper is available at http://www.rcjournal.com.
- Copyright © 2013 by Daedalus Enterprises









{kind=link}
{kind=link}