

Abstract
BACKGROUND: Patterns of pulmonary function tests (PFTs) and flow-volume loops among patients with clinically important tracheobronchomalacia (TBM) are not well described. Small studies suggest 4 main flow-volume loop morphologies: low maximum forced expiratory flow, biphasic expiratory curve, flow oscillations, and notching. We studied common PFT and flow-volume loop patterns among the largest prospective series of patients to date, undergoing clinical evaluation for symptomatic moderate to severe TBM.
METHODS: We conducted a retrospective analysis of prospectively collected data from patients who were referred to our Chest Disease Center from January 2002 to December 2008, with respiratory symptoms that were attributed primarily to TBM. The PFT results of 90 subjects with symptomatic moderate to severe TBM were evaluated.
RESULTS: By PFTs, 40 (44.4%) subjects had an obstructive ventilatory defect, 16 (17.8%) had a definite or highly likely restrictive ventilatory defect, 15 (16.7%) had a mixed defect, and 19 (21.1%) were within normal limits. Among 76 subjects with available flow-volume loops, the most frequent finding was low maximum forced expiratory flow, in 62 (81.6%) subjects, followed by biphasic morphology (15, 19.7%), notched expiratory loop (7, 9.2%), and expiratory oscillations (2, 2.6%). The balance of 13 subjects (17.1%) had no distinctive flow-volume loop abnormality.
CONCLUSION: PFTs and flow-volume loops are normal in a substantial number of patients with moderate to severe TBM, and should not be used to decide whether TBM is present or clinically important.
Introduction
Tracheobronchomalacia (TBM) is an increasingly recognized condition, associated with hypercompliant central airways.1–3 While the pathogenesis of diffuse TBM is often not known, it frequently occurs in patients with chronic airway inflammation.1,2 TBM has been identified in 1–4.5% of all patients undergoing bronchoscopy, 23% of patients with chronic bronchitis undergoing bronchoscopy, and 14.1% of patients with chronic cough.4–7 The most frequent presenting signs and symptoms include dyspnea on exertion, intractable cough, orthopnea, mucostasis, and recurrent infections.2,4,8,9
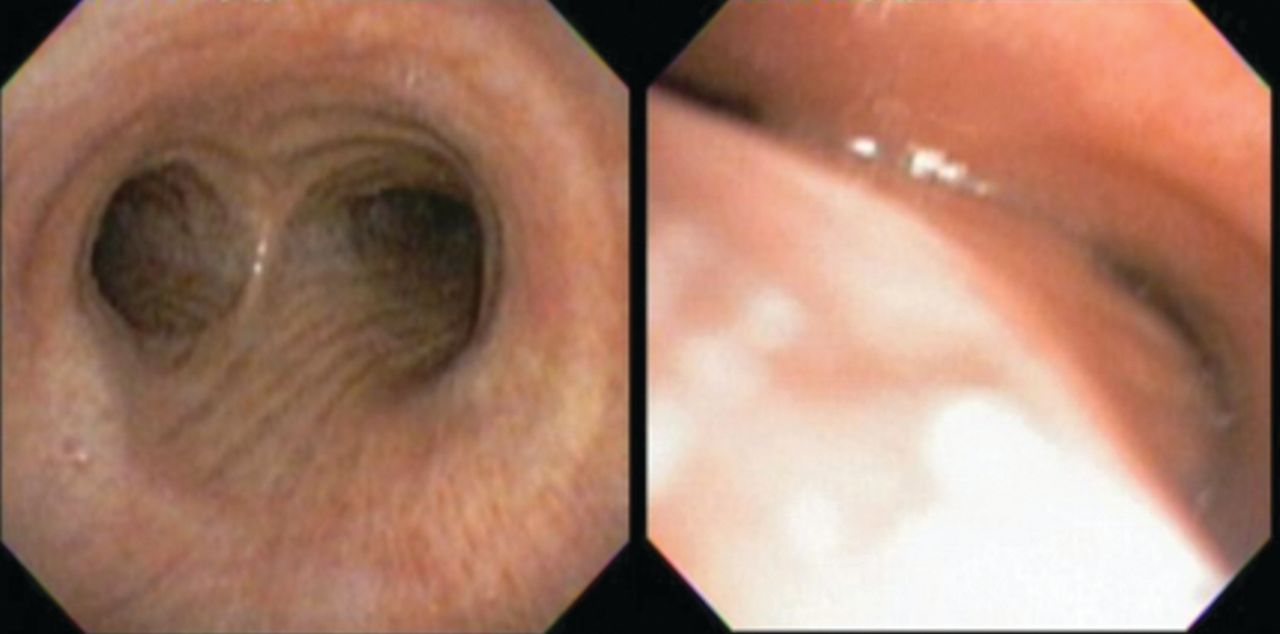
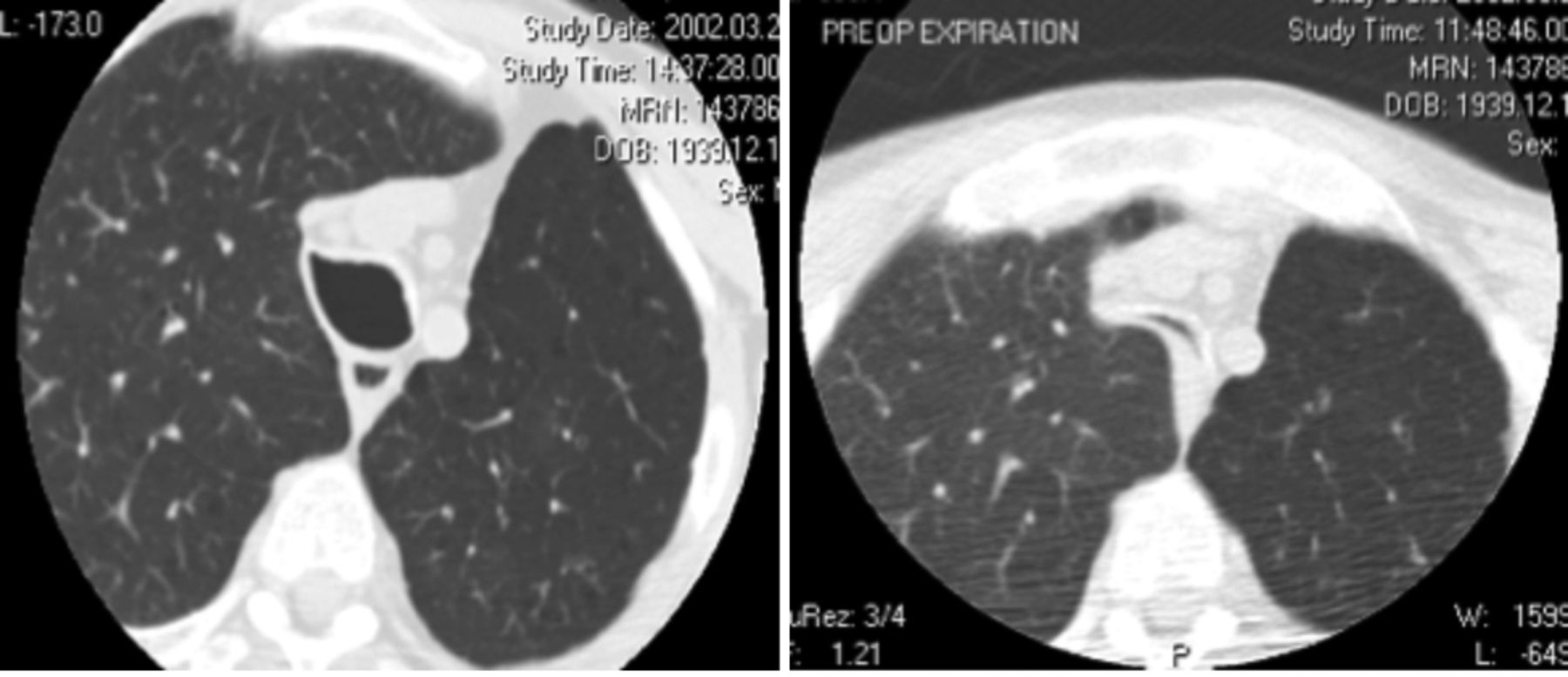
The diagnosis of TBM may be challenging, as patients often have other chronic pulmonary conditions such as asthma or COPD that may explain their symptoms. Formal diagnosis can be made with dynamic flexible bronchoscopy (Fig. 1) and dynamic airway computed tomography (Fig. 2).2,3 However, most patients will have pulmonary function tests (PFTs) as part of the initial workup for their presenting symptoms. While some characteristic PFT and flow-volume loop patterns have been described in patients with TBM, the prevalence and diagnostic utility of these patterns have not been determined in a large, well defined, cohort of patients.2–4

Dynamic flexible bronchoscopy. Left: During forced inhalation. Right: At exhalation.
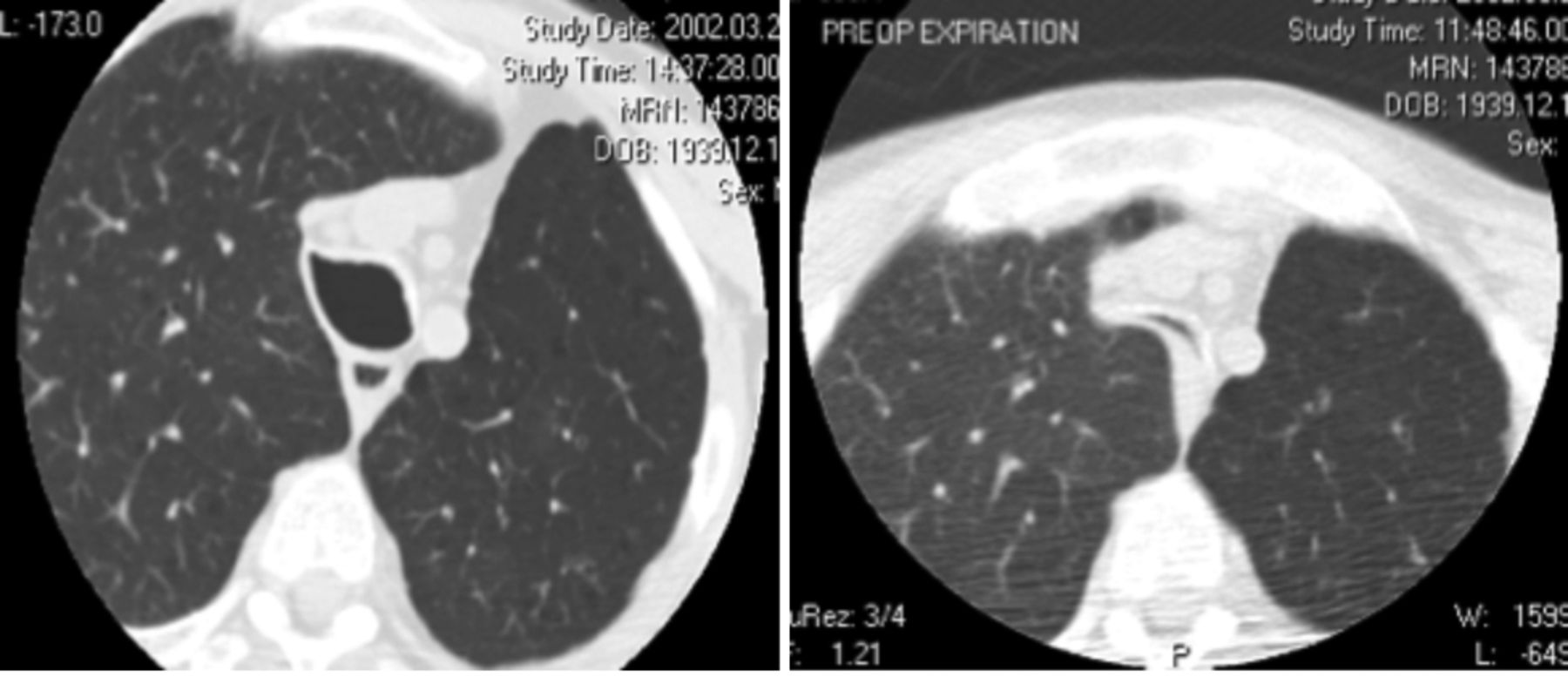
Dynamic computed tomography. Left: During forced inhalation. Right: At exhalation.
With increased awareness of TBM as an independent cause of clinical symptoms and functional impairment, the need for a standard diagnostic workup becomes more important. This is especially true in light of effective available therapies such as airway stenting, tracheoplastic surgery, and CPAP.8–10 Therefore, the role of PFTs in the initial evaluation of TBM needs to be better defined. Our objective was to describe the most common PFT and flow-volume loop patterns in a large series of patients undergoing evaluation for symptomatic moderate to severe diffuse TBM.
QUICK LOOK
Current knowledge
Flow-volume loop patterns in patients with clinically important tracheobronchomalacia have not been well described, but typically show low maximum forced expiratory flow, biphasic expiratory curve, flow oscillations, and notching.
What this paper contributes to our knowledge
The flow-volume loop patterns were normal in about 17% of subjects with moderate to severe tracheobronchomalacia, so the flow-volume loop pattern should not be used to decide whether tracheobronchomalacia is present or clinically important.
Methods
This study was performed at Beth Israel Deaconess Medical Center, Boston, Massachusetts. The protocol was approved by the institutional review board, Committee on Clinical Investigation at Beth Israel Deaconess Medical Center (research protocol 2005P-000112), and all patients undergoing evaluation for symptomatic TBM were asked to provide informed consent to become a part of the TBM database for future publications. We conducted a retrospective analysis of prospectively collected data from patients who were referred to the Chest Disease Center from January 2002 to December 2008, with respiratory symptoms that were attributed primarily to TBM. These patients are referred to our center by primary care physicians, pulmonologists, and thoracic surgeons from around the country, for further evaluation and treatment of suspected TBM. All patients with baseline PFTs prior to any airway intervention were included. Exclusion criteria were a prior airway intervention and mild or no TBM.
Moderate to severe TBM was defined as a > 75% collapse of the airway lumen anywhere along the trachea, main bronchi, or bronchus intermedius during forced expiration during dynamic flexible bronchoscopy. Age, sex, comorbidities, and respiratory symptoms were also recorded.
Dynamic flexible bronchoscopies were performed under light sedation and topical anesthesia.2,8,9 The bronchoscope was advanced into the proximal trachea, and the subject was instructed to forcefully inhale and exhale. This sequence was repeated at the mid-trachea, distal trachea, and proximal to the ostium of both main bronchi and the bronchus intermedius. The procedure was video recorded in order to generate airway images for subsequent quantitative analysis.
The PFTs were all performed with equipment (CPL, nSpire Health, Longmont, Colorado) that meets the American Thoracic Society standards. The equipment was calibrated daily. All maneuvers were done ensuring proper patient effort and reproducibility. Spirometry, lung volumes, and diffusing capacity of the lung for carbon monoxide (DLCO) were performed following the American Thoracic Society guidelines.11–14 All results were interpreted by a board-certified pulmonologist.
Statistical Analysis
This study is descriptive, and the results are expressed as frequencies, proportions, medians, and means ± SD, as appropriate. Statistical analyses were conducted with spreadsheet software (Excel 2007, Microsoft, Redmond, Washington) by one of the study authors (AFS).
Results
At the time of data collection, 172 patients had been referred for evaluation of symptomatic TBM. Ninety patients had both confirmed moderate to severe TBM and baseline PFTs performed prior to any airway intervention. Flow-volume loops were available for 76 (84.4%) of those patients (Fig. 3). Fifty-eight (33.7%) had moderate or severe TBM but were excluded due to prior airway interventions (ie, T-tube, tracheotomy, stents). Twenty-one patients (12.2%) who had mild TBM and 3 (1.7%) who did not have TBM were also excluded.

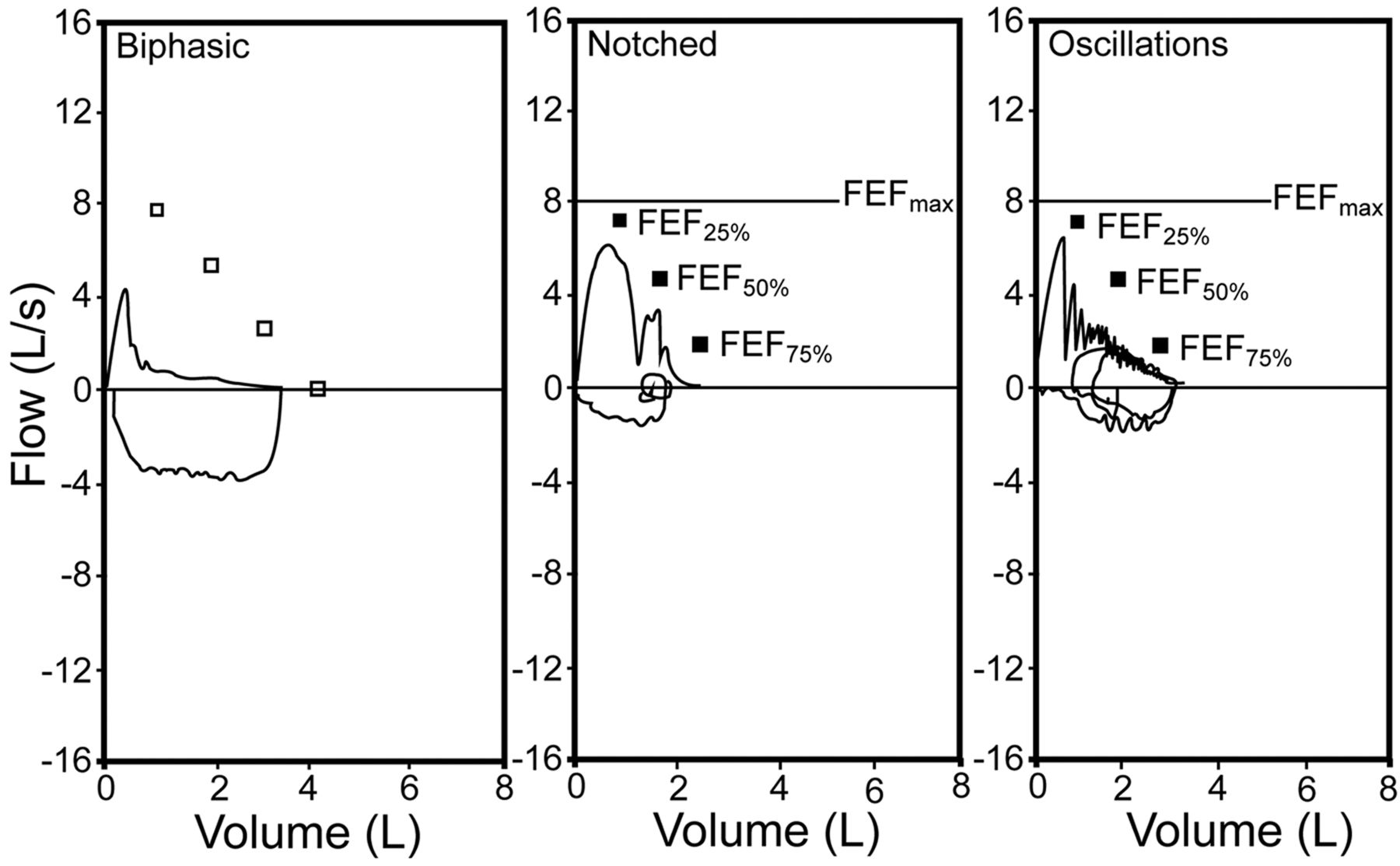
Flow-volume loop morphology. FEF25% = forced expiratory flow at 25% of the FVC maneuver.
The median age of the subjects was 65 years (31–95 y), 40 (44%) subjects were men, and mean body mass index was 30 ± 6 (Table 1). Forty-three (47.8%) had been diagnosed with COPD, and 21 (23%) had been diagnosed with asthma (Table 2). The most common presenting symptoms (Table 3) were dyspnea on exertion (71, 78.9%), severe chronic cough (63, 70%), and recurrent respiratory infections (48, 53.3%).
Subject Demographics and Pulmonary Function Test Results
Comorbidities in Subjects With Moderate to Severe Diffuse Tracheobronchomalacia
Presenting Symptoms and History in Subjects With Moderate to Severe Diffuse Tracheobronchomalacia
By PFTs, 40 of the 90 subjects (44.4%) had air-flow obstruction (defined as FEV1 < 80% of predicted and FEV1/FVC < 70% of predicted); 16 (17.8%) had definite or highly likely restriction (defined, respectively, as total lung capacity < 80% of predicted or, in the absence of total lung capacity measurement, reduced FVC with a normal FEV1/FVC). Fifteen (16.7%) had a mixed defect, and 19 (21.1%) were within normal limits (see Table 1).
Among subjects with flow-volume loops available, the most frequent finding was a below-predicted maximum forced expiratory flow (in 62, 81.6%), followed by biphasic morphology (15, 19.7%) (Table 4). This pattern shows a rapid peak and decline in expiratory flow, followed by a prolonged plateau extending throughout most of the expiratory maneuver (see Fig. 3). Notched expiratory loop (seen in 7 [9.2%] subjects) shows a rapid mid-expiratory dip and return of flow, without other indications of cough, and is reproducible in several maneuvers (see Fig. 3). Expiratory oscillations (seen in 2 [2.6%] subjects), are characterized by reproducible large-amplitude, high-frequency oscillations over much of the expiratory loop (see Fig. 3). The balance of subjects (13, 17.1%) had no distinctive abnormal flow-volume loop characteristics. These findings were not mutually exclusive, and a below normal maximum forced expiratory flow was also present in the other 3 patterns.
Flow-Volume Loop Morphology in Subjects With Moderate to Severe Diffuse Tracheobronchomalacia
Lung volumes and DLCO were obtained in 63 subjects. The mean percent-of-predicted values were: total lung capacity 86.8 ± 17.7%, residual volume 105 ± 35.5, ratio of residual volume to total lung capacity 119 ± 32.7), DLCO 70.4 ± 28.3 mL/min/mm Hg. The spirometric values from the groups with and without lung volumes did not differ significantly.
Discussion
In this large series of subjects with symptomatic moderate to severe diffuse TBM we found that PFT results demonstrated no characteristic and/or common pattern that would help to screen patients during initial diagnostic workup. Although many subjects (81.6%) were unable to achieve the predicted maximum forced expiratory flow, this index does not seem reliable, especially in light of the fact that almost 20% of the subjects showed normal values.
The biphasic flow-volume loop morphology is also characterized by a low maximum forced expiratory flow, which is followed by a rapid fall in flow, resulting in a plateau of very low flow for the remainder of exhalation. This pattern was described in 8 of 11 subjects with TBM in an observational study by Campbell and Faulks.15 Gandevia16 also described in 10 subjects with emphysema and TBM an initial phase of rapidly exhaled gas, followed by a linear phase of constant, slow flow.
Nuutinen5 and Koblet and Wyss17 described a notch in the expiratory limb of the flow-volume loop as typical of TBM. The notch was thought to be due to sudden decrease of flow with airway collapse. Their findings contrast with those of the current study, where only 7 (9.2%) subjects showed this particular finding. Campbell and Faulks thought that this finding was likely an artifact caused by the water-filled spirometer.15 Reinert and Steurich were unable to correlate this pattern with central bronchial collapse.18 The finding of reproducible notching in only 7 subjects in our study suggests that this is not a particularly reliable indicator of TBM.
Rapid flow oscillations have been defined by Vincken and Cosio as a “reproducible sequence of alternating accelerations and decelerations of flow, creating a saw-tooth pattern superimposed on the general contour of the flow-volume loop produced by the awake subject.”19 This pattern can be explained by the fact that rapid changes in either driving pressure or airway resistance can occur during inspiration and expiration, and have a characteristic frequency of 4–60 Hz. These oscillations have been described in different structural and functional disorders of the upper airways, including obstructive sleep apnea and neuromuscular disorders (ie, essential tremor, Parkinson's disease, Shy-Drager syndrome).19 Garcia-Pachon described oscillations in a patient with TBM.20 However, in the present study, oscillations were noted in the expiratory curve of only 2 (2.6%) subjects. Although the observed frequency is roughly almost twice that described in the general population, it is still quite infrequent.19
Interestingly, 17.1% of subjects in our series had a normal flow-volume loop. This suggests that compression of the central airways due to TBM is not necessarily the cause of air-flow obstruction, and that expiratory flow limitation occurs in more peripheral airways. This finding is supported by Loring et al, who described airway pressure-area characteristics by relating airway narrowing to the pressure differences measured across the central airway wall during graded expiratory efforts.21 They concluded that central airway collapse did not correlate with the degree of obstruction assessed by FEV1, and could be seen irrespective of the degree of expiratory flow limitation. Samad et al found no correlation between degree of air-flow obstruction and tracheobronchial collapse during cough.22 Reinert and Steurich also found no strong correlations between central airway collapse and lung function parameters in 30 unselected male patients.18 Consistent with this observation, previous studies have shown that clinical improvement after central airway stabilization is not always associated with an increase in FEV1.8,9
The low mean DLCO seen in our study is likely explained by the high prevalence of parenchymal lung disease in this patient population. It is possible that patients with emphysema may also have a greater tendency for expiratory central airway collapse, due to loss of elastic recoil, with reduced airway tethering. It is conceivable that sequelae from copious airway secretions, mucus plugging, and recurrent infections, as seen in TBM, may lower the DLCO in the absence of primary parenchymal lung disease. We did not find other studies that explored the relationship between DLCO and TBM.
An important limitation in the present study is the absence of a control group: all the subjects had moderate to severe TBM. We therefore cannot assess the specificity of various PFT abnormalities that may predict the presence of TBM. However, 19 (21.1%) subjects had normal PFTs. Since this finding alone allows some speculation to suggest poor sensitivity, one could make an argument that PFTs are not a precise screening tool for the presence of moderate to severe TBM.
It is also important to mention that many healthy subjects have a forced expiratory collapse of > 75%, so the finding of TBM may not have been pathologic in part of our sample population.23
Conclusions
PFTs are often used in the evaluation of patients with symptomatic TBM. Although some characteristic patterns in the expiratory limb of the flow-volume loop have been described, these seem unreliable for the diagnosis of TBM. Of particular interest, a substantial percentage of these patients have normal PFTs, which suggests that a diagnosis of TBM should not be ruled out in the setting of persistent symptoms with normal PFTs. At the same time, it is important to keep in mind that forced expiratory collapse exceeding what is currently viewed as normal may not be a pathologic finding.23,24 Based on our findings, the workup of TBM should rely on dynamic airway computed tomograms or bronchoscopy, and normal PFTs should not drive one away from pursuing this diagnosis.
Acknowledgments
We thank Rabih Bechara MD, Arthur Sung MD, Jed Gorden MD, Chakravarty Reddy MD, Saleh Alazemi MD, David Berkowitz MD, Dilip Nataraj MD, Samaan Rafeq MD, and Archan Shah MD for help in gathering the data.
Footnotes
- Correspondence: Adnan Majid MD, Chest Disease Center, Beth Israel Deaconess Medial Center, 185 Pilgrim Road, Deaconess 201, Boston MA 02215. E-mail: amajid{at}bidmc.harvard.edu.
The authors have disclosed no conflicts of interest.
- Copyright © 2013 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}