

Abstract
BACKGROUND: The diffusion capacity of the lung for carbon monoxide (DLCO) is a good marker of disease severity in patients with idiopathic interstitial pneumonia, and is associated with oxygen saturation; however, little is known about DLCO in systemic sclerosis patients with interstitial lung disease. We studied potential predictors of exercise-induced oxygen desaturation in patients with systemic sclerosis.
METHODS: Data were collected prospectively from 80 of 110 consecutive systemic sclerosis patients with normal oxygen saturation (> 95%) at rest, who could perform the 6-min walk test without physical discomfort, including leg pain. Pulmonary function tests and echocardiography were collected from all subjects.
RESULTS: Thirty subjects showed a ≥ 4% decline in oxygen saturation during the 6-min walk test (desaturation group). The other subjects were assigned to the normoxic group. The percent-of-predicted values for FVC, FEV1, total lung capacity, DLCO, and DLCO/alveolar volume were lower, and FEV1/FVC was higher, in the desaturation group. Logistic regression analysis showed the percent-of-predicted DLCO as a highly accurate predictor of exercise-induced oxygen desaturation: the area under the receiver operating characteristic curve was 0.92 (cutoff point 56.3%, sensitivity 0.83, specificity 0.86). Five subjects over the cutoff point of the percent-of-predicted DLCO in the desaturation group could not be distinguished from the normoxic subjects with the lung-volume measurements or right-ventricular systolic pressure.
CONCLUSIONS: The factor underlying exercise-induced oxygen desaturation appeared to be reduced percent-of-predicted DLCO, which was useful as a predictor in over 80% of the subjects.
- systemic sclerosis
- interstitial lung disease
- oxygen saturation
- pulmonary function
- pulmonary arterial hypertension
- 6-min walk test
Introduction
Exercise-induced oxygen desaturation in patients with interstitial lung disease may be one of the crucial factors in exercise limitation. An SpO2 decrease to ≤ 88% during the 6-min walk test (6MWT) predicts high mortality risk in patients with idiopathic interstitial pneumonia.1 Oxygen desaturation during 6MWT correlates with the diffusion capacity of the lung for carbon monoxide (DLCO).2,3 Impaired DLCO and pulmonary arterial hypertension are also found in patients with systemic sclerosis,4,5 and low DLCO (≤ 50%) was one of the predictors of death.6 However, SpO2 decrease of ≥ 4% during 6MWT correlates with age, dyspnea index, positive anti-Scl-70 autoantibody, and FVC, but DLCO has not been examined in relation to oxygen saturation in patients with systemic sclerosis.7
Identifying predictors of exercise-induced oxygen desaturation would help to select patients who might benefit from additional monitoring using oximetry during 6MWT when oxygen saturation is normal at rest. Moreover, the suggestion of cutoff points for these predictors would help alert patients to avoid hypoxic risk.8 In the present study we used 6MWT as a submaximal exercise to prospectively identify predictors of exercise-induced oxygen desaturation in patients with systemic sclerosis and interstitial lung disease.
QUICK LOOK
Current knowledge
The diffusion capacity of the lung for carbon monoxide (DLCO) is a good marker of disease severity in patients with idiopathic interstitial pneumonia, and is directly associated with a diminished oxygen saturation. The role of DLCO in characterizing interstitial lung disease in patients with systemic sclerosis is not known.
What this paper contributes to our knowledge
Reduced DLCO and percent-of-predicted lung volumes affected oxygen saturation during the 6-min walk test in patients with systemic sclerosis and interstitial lung disease. Percent-of-predicted DLCO was a sensitive and specific predictor of exercise-induced oxygen desaturation.
Methods
The study was approved by the ethics committee of Kanazawa University Hospital, Kanazawa, Japan, and all subjects gave written informed consent. Between 2008 and 2012, 110 consecutive adult patients with systemic sclerosis and interstitial lung disease were referred to the Division of Rehabilitation Medicine, Kanazawa University Hospital. Interstitial lung disease was diagnosed via pulmonary function tests, high-resolution computed tomography, and/or open lung biopsy. The main reasons for the patients' visits were for the evaluation and rehabilitation treatment of digit ulcers, joint contracture, and exercise intolerance.
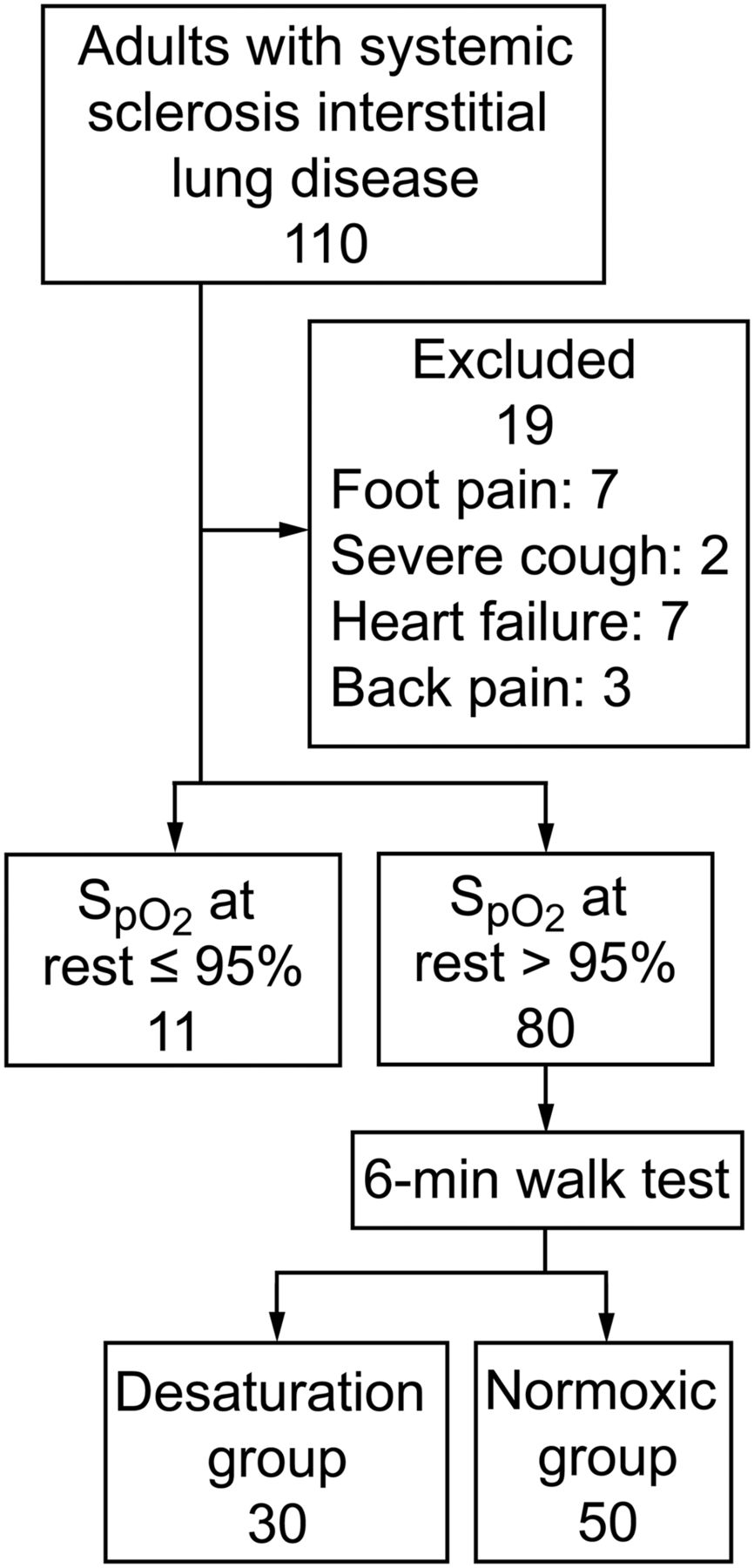
6MWT was conducted if SpO2 was > 95% at rest on room air. The exclusion criteria were pain in or ulcers on the foot, severe cough, heart failure, or back pain. We enrolled 80 subjects (66 female, 14 male), with a mean age of 57.4 years (Fig. 1). During the 6MWT SpO2 was monitored with a handheld pulse oximeter, with a reflectance sensor on the forehead, and was also measured at rest and at the end of the walk, without interfering with the 6MWT. We did not use a fingertip oximetry sensor because digit circulation is often deteriorated in patients with systemic sclerosis, which makes fingertip SpO2 readings inaccurate.9

Flow chart.
We measured percent-of-predicted FVC, FEV1, FEV1/FVC, total lung capacity (TLC), peak expiratory flow (PEF), residual volume/TLC (RV/TLC), DLCO, and DLCO/alveolar volume (DLCO/VA) (Chestac-9800, Chest Medical Instruments, Tokyo, Japan). Each predicted value was calculated with sex, age, and height10 (per the Baldwin formula). Single-breath DLCO was adjusted by hemoglobin concentration, according to the Cotes equation.2
Transthoracic echocardiography (iE33, Philips Healthcare, Best, Netherlands) was performed with the subject in the left-lateral decubitus position. Left-ventricular end-diastolic and end-systolic diameters were determined with M-mode echocardiography, and left-ventricular ejection fraction was calculated with the modified Simpson formula. Right-ventricular systolic pressure (RVSP), reflecting systolic pulmonary artery pressure, was estimated from the tricuspid regurgitating velocity, following the Bernoulli principle, via tissue Doppler echocardiography.11,12
Statistics
Subjects whose SpO2 decreased ≥ 4% during 6MWT were assigned to the desaturation group, because exercise desaturation of ≥ 4% predicts mortality1 and is an adverse prognostic sign13 in patients with idiopathic pulmonary fibrosis. The remaining subjects constituted the normoxic group. Differences between the 2 groups were calculated with the 2-tailed t test. The chi-square test was used to compare sex distribution and skin-involvement subsets (diffuse versus limited type). Logistic regression was used for parameters regarding exercise-induced oxygen desaturation; then, for parameters with high accuracy (indicated by the area under the receiver operating characteristic curve), sensitivity and specificity were obtained from critical points on the receiver operating characteristic curve. Moreover, all subjects were divided by degree of impairment in percent-of-predicted DLCO, and lung volumes and RVSP were compared between the 2 DLCO groups with the 2-tailed t test. Statistical analyses were performed with statistics software (JMP8.0, SAS Institute, Cary, North Carolina), except for the 95% CI for the area under the receiver operating characteristic curve, which was calculated with SPSS 17.0 (SPSS, Chicago, Illinois). In all analyses, P < .05 was taken to indicate significance.
Results
The Table describes the subjects. There were no differences in sex distribution, age, skin-involvement subset, duration of disease after the onset of Raynaud phenomenon, percent-of-predicted RV/TLC, percent-of-predicted PEF, left-ventricular ejection fraction, RVSP, or 6MWT distance between the desaturation and normoxic groups. The desaturation group had significantly lower percent-of-predicted FVC, FEV1, TLC, DLCO, percent-of-predicted DLCO, DLCO/VA, and percent-of-predicted DLCO/VA, and significantly higher FEV1/FVC.
Subjects
In the logistic regression analysis, percent-of-predicted DLCO was the most accurate predictor: area under the receiver operating characteristic curve 0.92 (Fig. 2). At the critical point on the receiver operating characteristic curve, the percent-of-predicted DLCO was 56.3% (sensitivity 0.83, specificity 0.86). When the cutoff point for percent-of-predicted DLCO was set at 56.3% for exercise-induced oxygen desaturation, 5 subjects in the desaturation group had percent-of-predicted DLCO > 56.3%, defined as the false negative subjects.
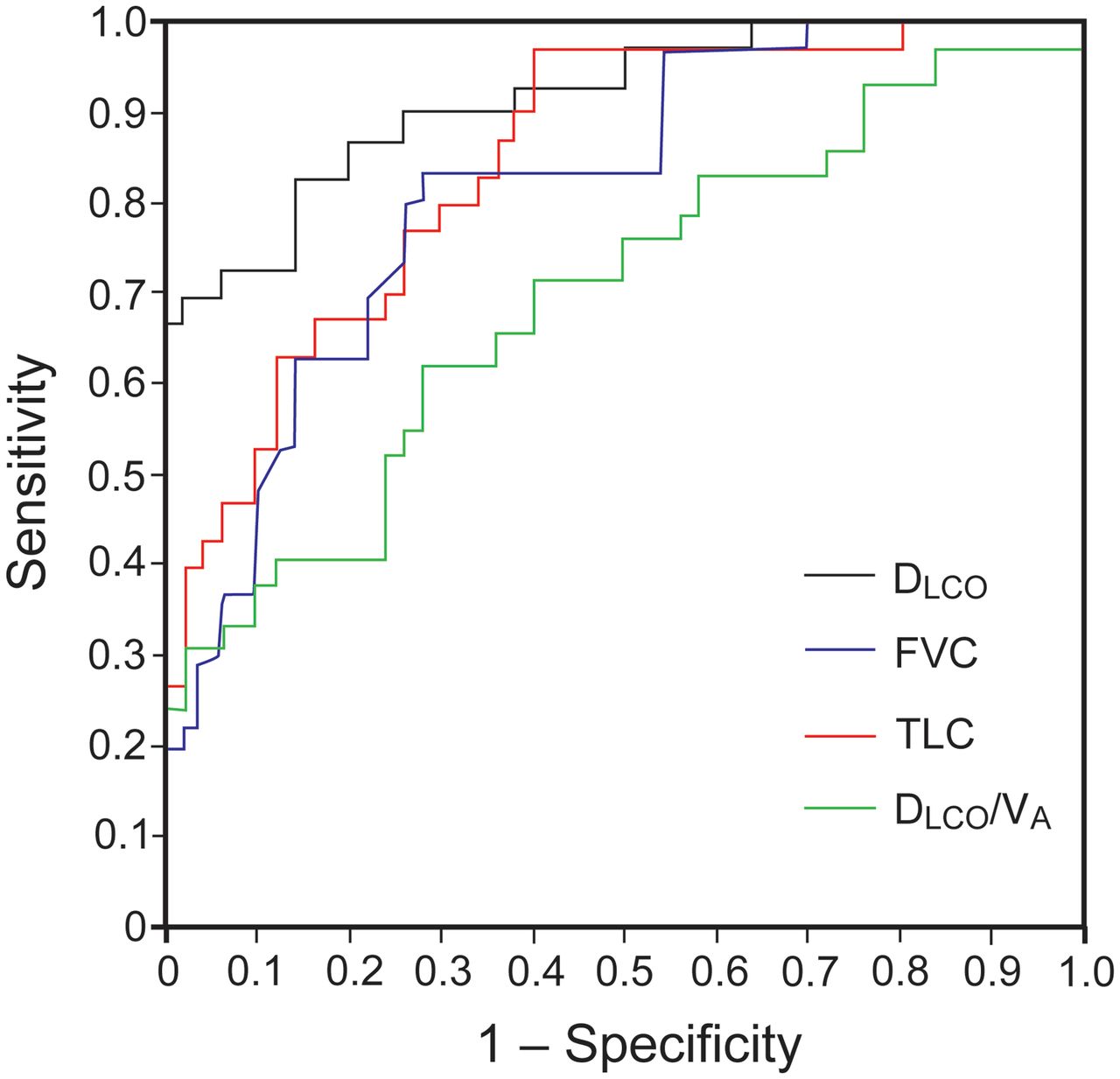
Receiver operating characteristic curves for parameters affecting oxygen saturation during 6-min walk test. DLCO = diffusion capacity of the lung for carbon monoxide. TLC = total lung capacity. VA = alveolar volume. The area under the receiver operating characteristic curves were 0.92 (95% CI 0.85–0.98) for percent-of-predicted DLCO, 0.82 (95% CI 0.73–0.91) for percent-of-predicted FVC, 0.84 (95% CI 0.76–0.93) for percent-of-predicted TLC, and 0.70 (0.57–0.82) for percent-of-predicted DLCO/VA.
All subjects were classified per the percent-of-predicted DLCO cutoff point, and then the percent-of-predicted FVC, FEV1, TLC, and RVSP values of the 2 groups were compared (Fig. 3). The percent-of-predicted FVC, FEV1, and TLC values in the desaturation group over the cutoff point were significantly lower than those in the normoxic group. There was no significant difference in RVSP between the 2 groups. However, 5 false negative subjects showed low values for 3 lung volume parameters, and the range of values of false negative subjects overlapped with that of subjects in the normoxic group. Therefore, it was difficult to predictively distinguish them from subjects in the normoxic group using lung volume parameters, even after classification for percent-of-predicted DLCO impairment.

Percent-of-predicted FVC, percent-of-predicted FEV1, percent-of-predicted total lung capacity (TLC), and right-ventricular systolic pressure in 80 subjects classified according to degree of impairment in diffusion capacity of the lung for carbon monoxide (DLCO), and according to desaturation (SpO2 decrease of ≥ 4%) or normoxia during the 6-min walk test.
Discussion
Significantly impaired DLCO, FVC, FEV1, and TLC were found in the desaturation group. Little information has been obtained on the correlation between lung parameters and exercise-induced oxygen desaturation in systemic sclerosis, though FVC previously showed a significant association with induced oxygen desaturation during 6MWT.7 Percent-of-predicted DLCO has been reported to be a predictor of 6MWT distance in patients with systemic sclerosis and interstitial lung disease.4 Exercise-induced oxygen desaturation in patients with idiopathic interstitial pneumonia correlates with walk velocity, percent-of-predicted DLCO and arterial oxygen pressure,14 percent-of-predicted DLCO and pulmonary capillary blood volume,3 and DLCO.2 In support of those studies, associations have been suggested between lung volume parameters and DLCO with exercise-induced oxygen desaturation in patients with systemic sclerosis and interstitial lung disease.
Impaired lung volumes, especially TLC, in the desaturation group indicated restrictive abnormalities, confirmed by the higher FEV1/FVC than in the normoxic group, and the similar PEF to the normoxic group. Moreover, RV/TLC did not differ between the 2 groups, and the mean values were not higher than normal. These results imply no significant obstructive abnormalities in these subjects. Generally, interstitial lung disease shows restrictive abnormalities, including lung volume reduction and the involvement of alveolar-capillary membranes, which reduces the 6MWT distance and lowest SpO2 during 6MWT, due to a disturbance in gas exchange.15
The reduced percent-of-predicted DLCO in the desaturation group was most severe, at 45.8% on average, among the lung function parameters. The percent-of-predicted DLCO/VA was also low, whereas the area under the receiver operating characteristic curve of the percent-of-predicted DLCO was larger than that of DLCO/VA. It has been suggested that the reduced DLCO was much greater than the loss of lung volume, because of parenchymal abnormalities.10 Moreover, low DLCO without reduced FVC is the earliest and most sensitive pulmonary functional abnormality in systemic sclerosis.16 DLCO/VA is also reduced in many patients, but it usually does not improve the sensitivity for detecting lung disease. The gas transfer reduction is not purely attributable to a loss of lung volume, but might also be secondary to alveolar-capillary membrane thickening and pulmonary vascular disease. In this study, since DLCO was adjusted according to the concentration of hemoglobin, it may be the preferable parameter to reflect alveolar-capillary membrane conductivity and/or pulmonary vasculopathy.6,17
The highest percent-of-predicted DLCO value in the desaturation group was 78.0% (results not shown), and the cutoff point for exercise-induced oxygen desaturation was 56.3%. With that criterion, 83% of subjects were correctly predicted regarding oxygen desaturation after 6MWT, and 5 subjects were false negatives. We attempted to detect parameters to identify false negatives to reduce the risk of unexpected exercise-induced oxygen desaturation, and found that lung volume parameters and RVSP were insufficient for that purpose. There might be some other factors that affect oxygen saturation during exercise.
Limitations
We did not evaluate pulmonary arterial hypertension during and after exercise. Patients with interstitial lung disease are prone to pulmonary arterial hypertension at rest and after exercise,5,18,19 and primary pulmonary hypertension or exercise-induced pulmonary arterial hypertension reduce SpO220 and percent-of-predicted DLCO.21 Those observations suggest that a high RVSP during exercise may induce oxygen desaturation. RVSP is an estimated value based on pulmonary arterial pressure measured via tissue Doppler echocardiography at rest, without catheterization, and > 40 mm Hg was the criterion for pulmonary arterial hypertension. Although the 5 false negative subjects did not show pulmonary arterial hypertension at rest, there is a possibility that exercise-induced pulmonary arterial hypertension or other pathogenesis may have affected these subjects. Complications associated with systemic sclerosis are multiple,22 so the number and severity of affected organs differ between individual patients. Further studies of exercise-induced desaturation are required.
Conclusions
Reduced percent-of-predicted lung volumes and of DLCO affected oxygen saturation during 6MWT in patients with systemic sclerosis and interstitial lung disease. Percent-of-predicted DLCO is a good candidate for a sensitive and specific predictor of exercise-induced oxygen desaturation in such patients.
Footnotes
- Correspondence: Fujiko Someya MD, School of Health Sciences, Kanazawa University, Kodatsuno 5-11-80, Kanazawa 920-0942, Japan. E-mail: fujiko{at}mhs.mp.kanazawa-u.ac.jp.
The authors have disclosed no conflict of interest.
- Copyright © 2014 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}