

Abstract
BACKGROUND: Anxiety and depression are prevalent comorbidities in patients with COPD. Breathing techniques can improve anxiety and depression in patients hospitalized for COPD exacerbation.
METHODS: We conducted a randomized clinical study with 46 male subjects, 67–86 years old, hospitalized with acute COPD exacerbation. Subjects were randomly and equally divided into a control group and a controlled breathing intervention group. We measured baseline and post-intervention dyspnea, anxiety and depression, quality of life (with the St George's Respiratory Questionnaire and the European Quality of Life questionnaire), maximum inspiratory and expiratory pressure, hand-grip strength, and sleep quality. The cohort had high dyspnea and low overall quality of life.
RESULTS: Controlled breathing techniques significantly improved dyspnea, anxiety, and mobility. All the measured variables improved in the intervention group. The control group had poorer values in all the variables after the hospitalization period.
CONCLUSIONS: Controlled breathing exercises improve anxiety and depression in patients hospitalized for COPD exacerbation. (ClinicalTrials.gov NCT01826682)
Introduction
COPD is a major and increasing cause of disability and death worldwide.1,2 COPD is associated with intermittent hospitalizations due to exacerbations characterized by acute deterioration in the symptoms of chronic dyspnea, cough, and sputum production. Hospitalizations due to COPD exacerbation are common (up to 60%)3 and an important part of the care of patients with COPD.
Anxiety and depression are the most prevalent psychological comorbidities in COPD patients, and decrease quality of life. They are associated with greater disability4 and impaired functional status5 in the areas of general health, physical roles, emotional roles, social functioning, bodily pain, mental health function, and vitality.6 Even after statistically controlling for the effects of overall health status, including additional medical diseases, COPD severity, and dyspnea, anxiety and depression remain significantly associated with decreased functional status.5,7 Anxiety is also related to the disease characteristics of COPD, including FVC,7 chest symptoms,8 and dyspnea.9
Breathing frequency is increased by physiological arousal, and in COPD patients the hyperventilation that results from anxiety markedly worsens shortness of breath by causing bronchoconstriction and lung hyperinflation.10–12 Hyperinflation increases the work and effort of breathing and reduces inspiratory reserve capacity.12,13
Finally, anxiety is a significant predictor of the frequency of hospital admission for COPD exacerbation,13 mortality risk,14,15 relapse risk,16 and hospital readmission.17 Few studies have assessed anti-anxiety programs in patients with COPD exacerbation. Numerous studies have explored the anxiety that develops in the hospitalization process.14,17 To our knowledge, however, few studies18 have explored the effects of a breathing program on anxiety.
Previous studies have found controlled breathing to be an effective treatment for different pulmonary symptoms.19 We hypothesized that controlled deep breathing would reduce negative affect level, as it has been found to do with smoking withdrawal.
The term “controlled breathing” encompasses exercises such as active expiration, slow and deep breathing, pursed-lips breathing, relaxation therapy, specific body positions, inspiratory muscle training, and diaphragmatic breathing.20 In COPD patients, controlled breathing relieves dyspnea by reducing dynamic hyperinflation, improving gas exchange, increasing strength and endurance of the respiratory muscles, and optimizing the pattern of thoraco-abdominal motion.21 In addition, psychological effects, such as controlling respiration, may also contribute to the effectiveness of controlled breathing. However, these effects are not discussed in the present study.
We studied the feasibility of implementing controlled breathing techniques in patients hospitalized for COPD exacerbation, and the efficacy of these techniques in improving dyspnea, sleep disturbance, anxiety, depression, and quality of life.
QUICK LOOK
Current knowledge
Anxiety and depression are common comorbidities in patients with chronic lung disease, and affect quality of life and long-term outcomes.
What this paper contributes to our knowledge
In hospitalized patients with chronic lung disease, controlled breathing techniques improved mobility and reduced dyspnea, anxiety, and depression scores.
Methods
This randomized pilot study was approved by our university and hospital ethics committees, and all subjects gave written consent.
Study Design
We compared the effects of a 10-day controlled breathing program to a standard care control intervention in subjects hospitalized for COPD exacerbation at San Cecilio University Hospital in Granada, Spain. Subjects in the standard care group received the standard medical treatment. Primary and secondary outcomes were measured at hospital admission and discharge.
Sample Size Calculation
Our sample size calculation was based on the primary outcomes: anxiety and depression symptoms scores. An increase in anxiety and depression symptoms (2 ± 3.3 points on the Hospital Anxiety and Depression questionnaire score) was expected in the control group, as reported in other studies,22 and a small positive effect (−5 points on the Hospital Anxiety and Depression questionnaire score) was anticipated in the treatment group. Hence, to have 80% power using a 2-sided α = .05, and a hypothetical dropout rate of 20%, we needed 23 subjects in each group to show statistically significant differences in anxiety and depression between the 2 groups.
Randomization Procedure
An independent nurse assigned subjects to the treatment or control group according to a computer-generated randomization list. The nurse informed the physiotherapist after the subject had given consent and been included in the study.
Subjects
Forty-six subjects were recruited during a 6-month period, from patients admitted to the hospital's pulmonary care unit and diagnosed with a non-infectious exacerbation of COPD (Figure). The diagnosis of COPD was made according to the criteria of the American Thoracic Society.23 All subjects had been free from exacerbation for at least 10 days (range 10–12 d). Patients with other organ failure, cancer, or inability to cooperate were excluded. During the exacerbation, all subjects were treated with standard medical therapy, including systemic steroids (76%), inhaled bronchodilators (100%), and oxygen.24
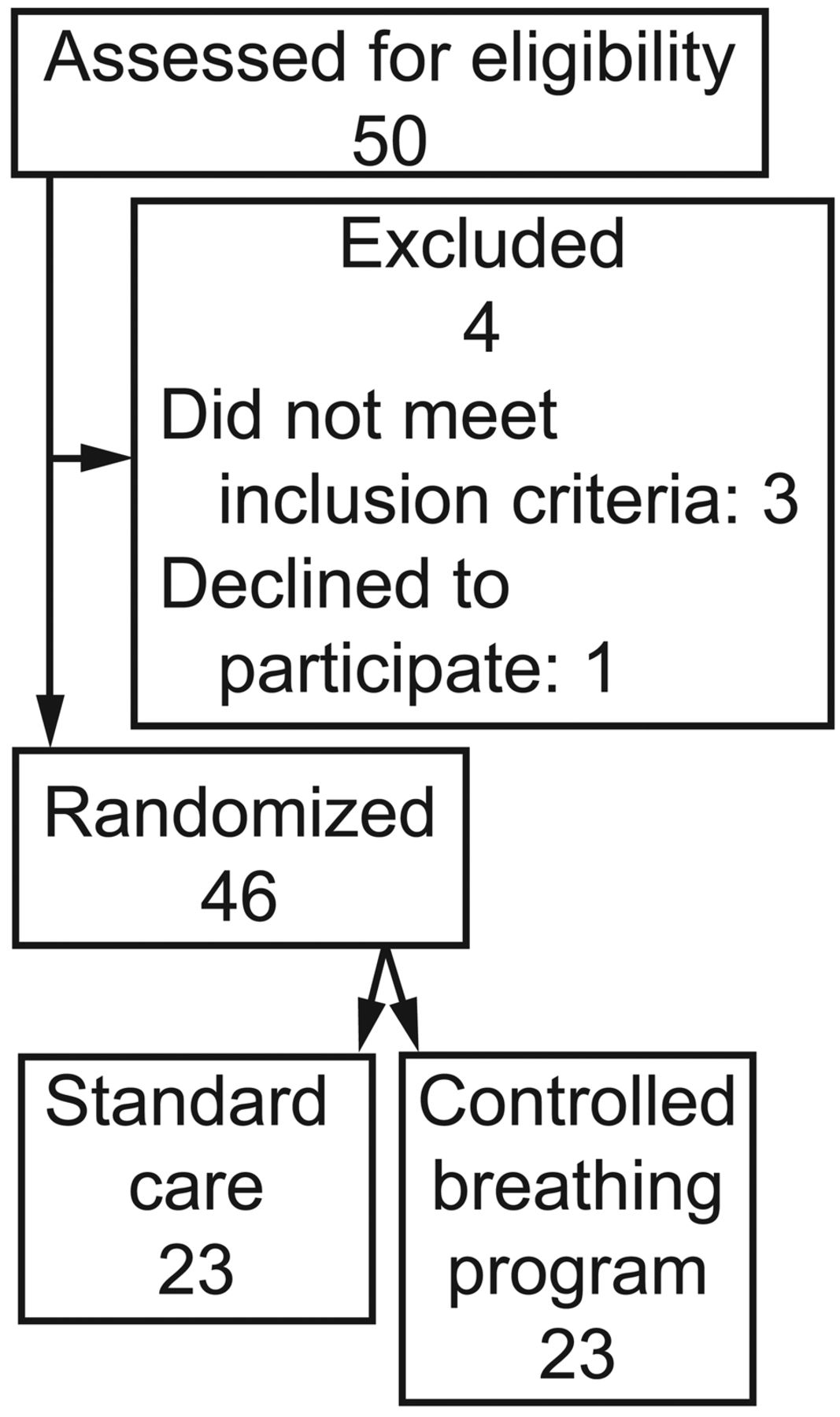
Flow chart.
Controlled Breathing Program
The controlled breathing program was delivered by a trained physiotherapist twice a day during hospitalization. The physiotherapy session duration was 30 min, and the subjects were instructed to take a break of 3 min when necessary. The controlled breathing program included relaxation exercises, pursed-lips breathing, and active expiration, as follows.
Relaxation Exercises.
Studies on relaxation exercises are based on the observation that hyperinflation is a partially reversible airway obstruction that is at least partly caused by an increased activity of inspiratory muscles during expiration.25 This increased activity may continue even after recovery from an acute episode of airway obstruction, and hence contributes to dynamic hyperinflation. Relaxation is also meant to reduce the breathing frequency and increase the tidal volume, thus improving breathing efficiency.26
Pursed-Lips Breathing.
Pursed-lips breathing improves expiration by requiring active and prolonged expiration and by preventing airway collapse. The subject performs a moderately active expiration through pursed lips, inducing an expiratory pressure of about 5 cm H2O.27 Compared to spontaneous breathing, pursed-lips breathing reduces breathing frequency, dyspnea, and PaCO2, and improves tidal volume and oxygen saturation at rest.28 Symptom-benefit patients have a more marked increase of tidal volume and decrease of breathing frequency.29
Active Expiration.
Contraction of abdominal muscles increases abdominal pressure during active expiration, which lengthens the diaphragm and contributes to operating the diaphragm close to its optimal length. Indeed, diaphragm displacement and its contribution to tidal volume during resting breathing has not been found to be different between COPD patients and healthy subjects.30,31 In addition, active expiration increases the elastic recoil pressure of the diaphragm and the rib cage, the release of which after relaxation of the expiratory muscles assists the next inspiration.
In summary, active expiration is a normal response to increased ventilatory requirements. In COPD patients, depending on the severity of airway obstruction, spontaneous activity of abdominal muscles is often already present at rest. Although active expiration improves diaphragm function,32 its effect on dyspnea remains unclear.
Outcome Measures
Hospital Anxiety and Depression Scale.
The Hospital Anxiety and Depression scale is a 14-item self-report questionnaire designed to detect psychological morbidity in medically ill patients.33 It contains depression and anxiety subscales, each with scores ranging from 0 to 21. A score above 8 on either subscale indicates possible depression and anxiety, and a score above 11 indicates probable depression and anxiety.34 A score of < 8 on the depression scale is considered normal, 8–10 indicates mild depression, 11–14 indicates moderate depression, and ≥ 15 represents severe depression.34 The Hospital Anxiety and Depression scale is a valid measure of depression and anxiety, with Cronbach alpha values of 0.83 for anxiety and 0.82 for depression.34
St George's Respiratory Questionnaire.
The St George's Respiratory Questionnaire is a standardized, self-administered questionnaire for measuring impaired health and perceived health-related quality of life in patients with airway disease.35 It includes 50 items, divided into 3 domains: symptoms, activity, and impacts. A score is calculated for each domain, and the total score includes all the domains. A low score indicates better health-related quality of life.
Modified Medical Research Council Dyspnea Scale.
Dyspnea was assessed with the modified Medical Research Council chronic dyspnea self-administered questionnaire, which consists of 6 questions about perceived breathlessness36: category 0 represents no dyspnea; category 1 represents slight dyspnea (troubled by shortness of breath when hurrying on the level or walking up a slight hill); category 2 represents moderate dyspnea (walks slower than people of the same age on the level, because of breathlessness); category 3 represents moderately severe dyspnea (has to stop because of breathlessness when walking at own pace on the level); category 4 represents severe dyspnea (stops for breath after walking about 100 m or after a few minutes on the level); and category 5 represents very severe dyspnea (too breathless to leave the house or breathless when dressing or undressing).
European Quality of Life Questionnaire.
The generic European Quality of Life questionnaire37,38 consists of the EQ-5D visual analog scale and the EQ-5D index. The visual analog scale has a rating scale of 0 to 10 points, taken as 0–100% (0% = death/worst possible health, and 100% = best possible health). The questionnaire has 5 domains: mobility, self-care, usual activity, pain/discomfort, and anxiety/depression. For each item the subject selects one of 3 descriptive health states (from good to poor) and the number/percentage of subjects selecting each state is recorded.
Hand-Grip Strength.
We measured hand-grip strength with a dynamometer (TEC-60, Technical Products, Clifton, New Jersey) individually adjusted for the size of the subject's hand-grip. Three measurements were made on each hand and the peak force was recorded.39 This test has been used for measuring muscle strength in people with COPD.40
Respiratory Muscle Strength.
We measured maximum inspiratory and expiratory pressures (Micro-RPM, SensorMedics/CareFusion, San Diego, California) in each subject 4 times, at 2-min intervals, and normalized the readings to predicted values.41 All respiratory tests were performed by cardiopulmonary physiotherapists, with the subject in sitting position.
Statistical Analyses
Baseline characteristics were compared using the Mann-Whitney U test for continuous variables, and the chi-square test for categorical variables. Results are shown as number and percentage or mean ± SD. Inter-group and intra-group differences were analyzed with 2-way repeated-measures analysis of variance. We also used the paired-sample Student t test for intra-group comparisons. An intention-to-treat analysis was carried out assuming that subjects who could not continue the program had the same change as the average improvement in the intervention group. A 2-tailed P value < .05 was considered significant. All statistical analyses were performed with statistics software (SPSS 20.0, SPSS, Chicago, Illinois).
Results
Table 1 shows the baseline characteristics. All the subjects were male. The mean age was 76 ± 5.5 y in the intervention group and 74.43 ± 6.7 y in the control group. There were no significant differences in the percentages of subjects who used alcohol and tobacco. Both the intervention and control groups had 2 hospitalizations per year. The St George's Respiratory Questionnaire subscales showed significant differences between the groups in the activity domain and the total score, with higher scores in the control group, meaning a worse quality of life.
Baseline Characteristics
Table 2 shows the baseline values and the changes in dyspnea, anxiety and depression, and quality of life scores. No significant differences were found in any of the baseline values. The dyspnea scores significantly improved in the intervention group (P = .004), whereas the control group's dyspnea score increased between baseline and discharge. The anxiety and depression subscores of the Hospital Anxiety and Depression scale showed better improvement after the controlled breathing intervention. Higher mean change values were found in the depression score (10.56 ± 0.465). All the European Quality of Life subscales showed better improvement at discharge in the intervention group, with greater improvements in the mobility score and the anxiety/depression score.
Baseline Versus Discharge Dyspnea, Anxiety and Depression, and Quality of Life Scores
Discussion
The objective of this study was to assess the effects of a controlled breathing program on anxiety and depression in subjects hospitalized for COPD exacerbation. Although numerous studies have recognized the physical and psychological effect of hospitalization,42,43 no studies have explored these effects in acute COPD.
Previous studies found a poor physiological status, a moderately impaired quality of life, and higher levels of anxiety and depression than other pathologies in COPD.44,45 Additionally, individuals with COPD reported that episodes of heightened and intractable dyspnea were inextricably associated with anxiety.46 Anxiety and/or depression is an important risk factor for re-hospitalization within a 12-month period in COPD patients with poor health-related quality of life.47
Various studies have evaluated therapies for anxiety, depression, quality of life, and function in subjects hospitalized for COPD exacerbation, and the results have been contradictory. In one trial, incentive spirometry significantly improved St George's Respiratory Questionnaire scores, compared with standard care,48 while another trial found a mean increase in the Barthel score, favoring the use of a gutter frame over a rollator.49 No significant improvements were found in daily weight, eating, sleeping, and exercise scores when the incentive spirometry group was compared with the standard care group.50 To our knowledge, no previous studies have assessed the effectiveness of a therapeutic program in subjects with COPD exacerbation, considering the variables included in the present study. Several studies have shown that COPD exacerbation harms health-related quality of life,51 pulmonary function,52 and survival53 of COPD patients.
The present study found a significant improvement in functional and psychological variables in the intervention group and significant deterioration in the control group, due to the hospitalization effect. This suggests that the patient's inactivity54 during hospitalization is a factor in functional and psychological impairment during COPD exacerbation.
Pulmonary rehabilitation programs can reduce anxiety in COPD patients.55,56 Emery et al57 found that an exercise training program combined with education that included stress management techniques significantly reduced anxiety. Curiously, stress management sessions without exercise training did not improve anxiety. This is in line with our results, suggesting that an additional value of exercise in its different modalities (breathing or global training) can improve psychological status in patients with COPD.
The present study had 2 important limitations. First, the sample size was small and included only males. Second, we did not obtain follow-up data after discharge.
Conclusions
Our study addresses an important rehabilitation option in COPD patients, and is novel as few studies have investigated the effect of breathing techniques during the early post-exacerbation period.43
Footnotes
- Correspondence: Marie Carmen Valenza PT PhD, Physical Therapy Department, Faculty of Health Sciences, University of Granada, Avenida de Madrid s/n 18071, Granada, Spain. E-mail: cvalenza{at}ugr.es.
The authors have disclosed no conflicts of interest.
- Copyright © 2014 by Daedalus Enterprises









{kind=link}