

Abstract
BACKGROUND: Intrathoracic pressure in patients undergoing laparoscopic surgery may be affected by intra-abdominal pressure during surgery. We investigated the relationship between intra-abdominal pressure (Pabd) and esophageal pressure (Pes) in mechanically ventilated patients undergoing laparoscopic surgery.
METHODS: We prospectively studied 43 consenting patients over 18 y of age who were scheduled for elective laparoscopic surgery with plans for intra-operative intubation and paralysis. After establishing a good level of inter-observer agreement on Pes measurements, Pes was measured by one observer for each patient using an esophageal catheter. Pabd and Pes were recorded before and after abdominal insufflation. We used regression analysis to model the relationship between Pabd and Pes.
RESULTS: Patients' ages varied from 22 to 78 y, with a mean of 53.2 ± 14.6 y. Body mass index (BMI) varied from 13.7 to 60.5 kg/m2, with a mean of 33.7 ± 10.5. PEEP was 5–7 cm H2O for 19 patients and 0 cm H2O for the remainder. Most patients underwent gastric bypass surgery (n = 11); others underwent hernia repair (n = 9), colon resection (n = 7), cholecystectomy (n = 6), and various other surgeries (n = 10). Using univariate analyses, baseline Pabd was significantly correlated with baseline Pes (estimate of model coefficient [95% CI]: 0.79 [0.36–1.21], R2 = 0.24, P = .001), as was BMI (0.29 [0.19–0.40], R2 = 0.41, P < .001). However, a multivariable analysis showed no significant correlation with baseline Pabd (0.10 [−0.46 to 0.65], P = .73), whereas BMI remained highly significant (0.27 [0.11–00.43], P = .001) with R2 = 0.40. Due to unexpected uniformity of abdominal inflation pressures (generally 20.4 cm H2O) during surgery, data were not amenable to assessment of correlation between changes in abdominal and esophageal pressures after inflation.
CONCLUSION: There was a limited correlation between baseline Pes and Pabd in patients undergoing elective laparoscopic surgery, suggesting a limited value of Pabd measurements in the management of mechanically ventilated patients.
Introduction
Transpulmonary pressure during positive-pressure ventilation refers to the summation of positive forces that inflate the lungs (airway inflation pressure) and negative forces that prevent the lungs from collapsing (pleural pressure). In healthy subjects with normal lungs, transpulmonary pressure is slightly positive, which serves to maintain a functional residual capacity. For critically ill patients with ARDS, maintaining an “open lung” is important to minimize end-expiratory atelectasis, which might otherwise contribute to ventilator-induced lung injury and possibly the risk of death.1–5 Esophageal pressure manometry is a method to estimate pleural pressure and thus derive the transpulmonary pressure.3,6–9
Investigations of a role for esophageal manometry in guiding mechanical ventilation show promise. The application of PEEP to the airways, as guided by the measurement of esophageal pressure to estimate transpulmonary pressure, has demonstrated improved respiratory system compliance and improved oxygenation in critically ill adults with ARDS.5,6 Despite these reported successes, clinical uptake has been limited. This may be related, in part, to lack of familiarity with the technology and the invasive nature of esophageal probe insertion.3–10 The availability of accurate and familiar surrogate measurements for esophageal pressure could, in theory, help to overcome these deterrents. One potential surrogate is abdominal pressure (Pabd), which can be measured at the bedside as bladder pressure. However, a previous study has shown a significant but limited correlation between gastric pressure (Pga) and esophageal pressure (Pes) in patients with acute respiratory failure (R2 = 0.354, P < .0001).3
The main objective of this study was to explore the correlation between Pabd (as measured via an abdominal insufflator) and Pes (as measured via esophageal pressure manometry) in surgical patients undergoing laparoscopic surgery. Establishing a correlation between Pabd and Pes may stimulate researchers to look at the use of bedside abdominal pressure measurements (bladder pressure) rather than esophageal pressure to optimize the application of PEEP in the ICU.
QUICK LOOK
Current knowledge
Esophageal manometry estimates pleural pressure and can be used to derive transpulmonary pressure. Abdominal pressure as determined by bladder pressure has also been used to determine transpulmonary pressure. Laparoscopic abdominal surgery uses carbon dioxide insufflation to optimize the surgical field, increasing intra-abdominal pressure.
What this paper contributes to our knowledge
In a group of patients without respiratory disease undergoing laparoscopic surgery, there was a significant but limited relationship between esophageal and abdominal pressures. Intra-abdominal pressure cannot predict esophageal pressure but can provide complementary information useful in setting mechanical ventilation.
Methods
Study Design
We conducted a prospective single-cohort observational study at St. Joseph's Healthcare Hamilton (SJHH) in Ontario, Canada. The study underwent full review and received approval by the SJHH Research Ethics Board.
Patients
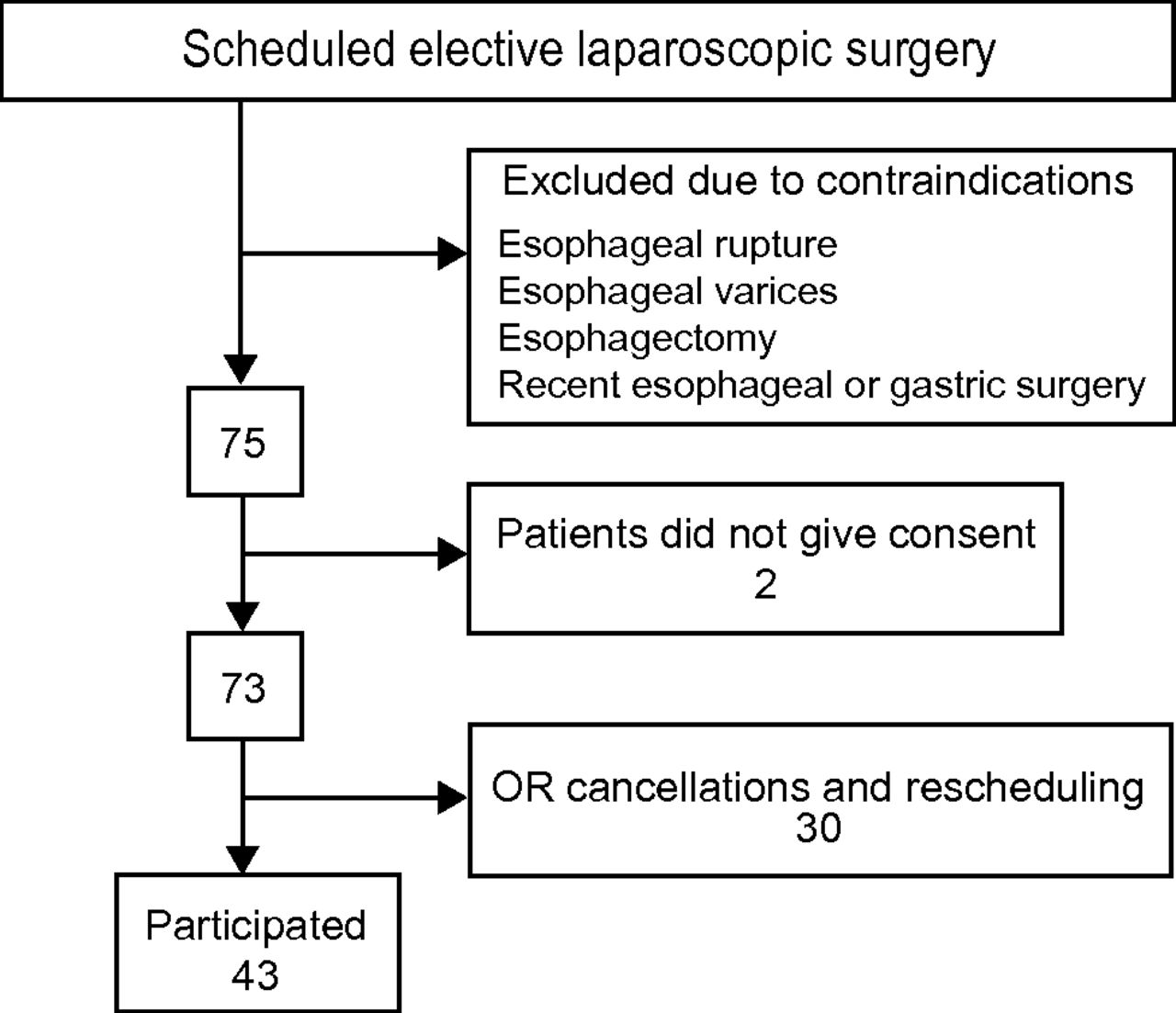
Patient recruitment began in January 2011 and stopped at the end of March 2011. We screened patients in the adult pre-operative clinic for the following inclusion criteria: scheduled elective laparoscopic surgery, age >18 y, and a plan for intra-operative intubation and paralysis. We excluded patients with any contraindication to esophageal manometry, including esophageal rupture, esophageal varices, esophagectomy, or recent esophageal or gastric surgery. Measurements in the operating room were obtained in parallel with patients' recruitment in the pre-operative clinic during these 3 months depending on the surgery time and date.
Measurements
In the operating room, study patients were sedated, paralyzed, and mechanically ventilated, in accordance with both routine surgical care and the study protocol. All patients were positioned supine. We reviewed 3 distinct protocols for esophageal catheter insertion3,5,7–9 and chose the technique used recently by Talmor et al3,5 in their management of critically ill adults with ARDS. A study investigator inserted the esophageal catheter (adult esophageal balloon catheter set, CooperSurgical, Trumbull, Connecticut). The catheter was inserted to 60 cm and connected to a pressure transducer, and pressure waveforms and measurements were displayed on an associated monitor. Placement in the stomach is usually confirmed in passively breathing patients by the absence of cardiac oscillations, a rise in pressure during a positive-pressure breath delivered by the ventilator, and a transient increase in pressure during a gentle compression of the abdomen, and there should be no resistance (due to coiling) when removing the catheter stylet. To avoid contaminating the surgical field, gentle compression of the abdomen was omitted. The catheter was then withdrawn to 40 cm and assumed to be placed in the lower third of the esophagus only if cardiac oscillations were noted. Two investigators (AS and TP) obtained Pes measurements independently for the first 5 patients to assess inter-rate agreement. Inter-rate agreement was 0.44 (moderate agreement) using Cohen's kappa statistics method,11 and the investigators further unified their procedures accordingly. A study by Pelosi et al12 showed that pleural pressure could be estimated by measuring esophageal pressure directly at mid-lung height, which we did in our study. However, their study was conducted in animal models. In humans, the effect of mediastinal weight on Pes measured in healthy volunteers in the supine position was ∼3 cm H2O.13 For this reason, we subtracted 3 cm H2O from our measured Pes values.
After the attending surgeon inserted an abdominal insufflator (PneumoSure 45L insufflator, Stryker, Kalamazoo, Michigan), a study investigator recorded the baseline esophageal pressure at end of expiration, as identified from the waveform display. Next, the surgeon insufflated the abdomen to achieve adequate visualization in accordance with routine surgical management, and a post-insufflation esophageal pressure measurement was recorded, again at end of expiration. Foley catheter insertion was uncommon; therefore, abdominal pressures were directly recorded for all patients from the insufflator screen by a study investigator.
Data Collection and Statistical Analysis
Study data for each patient include demographics, primary diagnosis, comorbidities, and pressure data before and after abdominal insufflation. Data were entered into a password-protected database.
The sample size for this study was determined based upon the following statistical considerations. We needed a sample size that would allow us to fit a regression with 3 predictor variables of interest: body mass index (BMI), PEEP, and baseline pressures. Our original plan was to study 50 patients over 4–6 months; however, with delays related to equipment availability and cancelled surgeries, we terminated the study after including 43 patients over 3 months.
Baseline and study data are summarized using descriptive summary measures, expressed as mean ± SD for continuous variables and count frequencies (percentages) for categorical variables. We conducted univariate and multiple linear regression analyses using insufflation Pes measurement as the outcome with baseline Pes, Pabd, and BMI as independent variables. We were unable to investigate the correlation between changes in Pes with change in Pabd due to an unexpected lack of variability in insufflation pressures. Specifically, in contrast to prior experience, surgeons routinely inflated the abdomen to ∼15 mm Hg (20.4 cm H2O). We assessed for collinearity (correlations among predictors) using a scatter plot and variance inflation factor (VIF), and considered variables with VIF > 10 as collinear.14 Model assumptions and goodness of fit were evaluated using the residual plot and R2, respectively. Results from the regression analysis are reported as an estimate of the coefficient and the corresponding 95% CI values and associated P values. All analyses were performed using statistics software (Stata 10, StataCorp, College Station, Texas).
Results
Seventy-three patients consented to participate in the trial, and 43 were included (Fig. 1). Thirty patients were not included as a result of surgical cancellations, with or without rescheduling within the allotted time frame of the study. Tables 1 and 2 summarize baseline patient characteristics. Patients' ages varied from 22 to 78 y, with a mean of 53.2 ± 14.6 y. BMI varied from 13.7 to 60.5 kg/m2, with a mean of 33.7 ± 10.5 kg/m2. Fifty-one percent of the patients were classified as obese. All patients were ventilated using either pressure or volume control mode. Nineteen patients were on PEEP during surgery; levels varied between 5 and 7 cm H2O. Most patients underwent gastric bypass surgery (11/43). Mean baseline Pes and Pabd were 9.5 ± 4.7 and 7.8 ± 3.0 cm H2O, respectively.

Trial enrollment. OR = operating room.
Baseline Clinical Statistics
Ventilatory Settings
Using univariate analyses, we found that baseline Pabd is significantly correlated with baseline Pes (estimate of model coefficient [95% CI]: 0.79 [0.36–1.21], R2 = 0.24, P = .001), as was BMI (0.29 [0.19–0.40], R2 = 0.41, P < .001) (Fig. 2). However, a multivariable analysis showed no significant correlation with baseline Pabd (0.10 [−0.46 to 0.65], P = .731), whereas BMI remained highly significant (0.27 [0.11–0.43], P = .001) with R2 = 0.40 (Table 3). However, the correlation between post-insufflation pressures and changes in abdominal and esophageal pressures could not be calculated as a result of an insufficient range of values in post-insufflation abdominal pressures and change in abdominal pressures.

Esophageal and intra-abdominal pressures at baseline related to body mass index (BMI). Pes = esophageal pressure.
Linear Regression With Internal Model Validation
Discussion
In this prospective observational study, we found a significant but limited correlation between baseline Pes and Pabd in patients undergoing laparoscopic surgery (see Table 3). This correlation was not statistically significant after adjusting for BMI.
To our knowledge, there are no studies that have previously addressed this question in the same population. However, a relevant study3 reported a significant correlation between Pga as an indirect method for measuring intra-abdominal pressure and Pes in patients with acute respiratory failure in the ICU (R2 = 0.354, P < .0001). Their results were similar to ours even though their recorded Pga (16.6 ± 6.8 cm H2O) and Pes (17.5 ± 5.7 cm H2O) were different from our recorded Pabd (7.8 ± 3 cm H2O) and Pes (9.5 ± 4.7 cm H2O). The Pes measurements in their study were done at the end of exhalation, as was done in our study. However, their mean PEEP level was 14.2 cm H2O, and ours was only 2.7 cm H2O. It is uncertain whether the Pes levels recorded in their study are a result of the application of airway pressure or are due to secondary causes related to lung injury. In the same study, however, Pes was not correlated with obesity as assessed by BMI at end of expiration (R2 = 0.051, P = .069), which is in contrast to what we found (95% CI 0.29 [0.19–0.40], R2 = 0.41, P < .001). This is likely due to the significant difference between our recorded Pes (9.5 ± 4.7 cm H2O) and their recorded Pes (17.5 ± 5.7 cm H2O), which raises the possibility that this correlation between Pes and BMI may not exist at higher levels of Pes.
Does this mean that intra-abdominal pressure measurements have a minimal role in the assessment of mechanically ventilated patients? It has previously been shown that intra-abdominal pressures > 12 cm H2O increase chest-wall elastance in two thirds of patients.15 However, chest-wall elastance does not correlate well with Pes at end of expiration (R2 = 0.011, P = .05).3 Therefore, although Pabd may not be valuable in predicting Pes, it may still provide complementary information that may be useful in the management of patients receiving mechanical ventilation.
Favorable conditions were present in this study to investigate these relationships: Patient positioning and measurement techniques were consistent, Pabd was measured directly rather than estimated through gastric or bladder measurements, and all subjects received neuromuscular blockade to eliminate the effect of diaphragmatic tone. However, our study has some noteworthy limitations. We had hoped to include correlation data after abdominal insufflation. Unfortunately, post-insufflation Pabd measurements were far more uniform than anticipated. The lack of variability in post-insufflation Pabd pressures made the correlation between post-insufflation Pes and Pabd or the changes in Pes and Pabd statistically challenging and unreliable. The generalizability of our findings to other settings is also limited. Although there was a difference in the ventilation modes used (pressure or volume), the mode would not impact baseline end-expiratory values of Pes. However, some patients had low levels of PEEP applied and others did not, and this may have affected baseline levels of Pes. Unfortunately, plateau airway pressures were not documented because we were interested in end-expiratory values. If we had measured inspiratory plateau airway and esophageal pressures, we could have included much more valuable data related to lung and chest-wall mechanics.
In a recent landmark ARDS trial,5 esophageal balloon manometry was used to select PEEP levels to minimize end-expiratory atelectasis. It was hypothesized that maintaining a positive end-expiratory transpulmonary pressure would result in better lung recruitment and less atelectrauma. This novel approach resulted in greater PEEP levels than reported for the control strategy16 and better oxygenation, and it appeared to improve survival, although the mortality analyses were limited by a very small number of deaths.17 The goal of determining a correlation between Pabd and Pes is to provide a surrogate method of estimating transpulmonary pressure.
Conclusions
In conclusion, we found a significant but limited correlation between baseline Pes and Pabd in patients undergoing laparoscopic surgery. Further investigations to elucidate the relationships between abdominal and pleural pressure measurements in critical illness may serve to refine mechanical ventilation protocols.
Acknowledgments
We thank Toni Tidy and Dr Marc de Somer for their kind contribution to this project.
Footnotes
- Correspondence: Anees Sindi MBChB, Department of Anesthesia and Critical Care, King Abdulaziz University, Jeddah 22254, Saudi Arabia. E-mail: ansindi{at}me.com.
Dr Sindi and Mr Piraino are co-first authors.
This research was supported by the Father Sean O'Sullivan Research Centre and the Firestone Institute for Respiratory Health, St. Joseph's Healthcare Hamilton. The authors have disclosed no conflicts of interest.
- Copyright © 2014 by Daedalus Enterprises









{kind=link}
{kind=link}