

Abstract
BACKGROUND: Circadian rhythm regulates many physiologic and immunologic processes. Disruption of these processes has been demonstrated in acutely ill, mechanically ventilated patients in the ICU setting. Light has not been studied as an entraining stimulus in the chronically mechanically ventilated patient. The purpose of this study was to determine the association of naturally occurring ambient light levels in a long-term acute care (LTAC) hospital with circadian rhythm in patients recovering from critical illness and requiring prolonged mechanical ventilation (PMV).
METHODS: We performed a prospective observational study of 15 adult patients who were recovering from critical illness and receiving PMV and who were admitted to the ventilator weaning unit at an LTAC hospital. Demographic data were obtained from chart review. Light stimuli in each patient room were assessed using a photometer device placed at eye level. Circadian rhythm was assessed by wrist actigraphy. Cumulative data were obtained from each device for a 48-h period, averaged into 4-h intervals, and analyzed.
RESULTS: Patients receiving PMV were obese (mean body mass index of 32.7 ± 10.3 kg/m2) and predominantly female (73%) and had an average age of 63.1 ± 14.3 y. Light exposure to this cohort maintained diurnal variation (P < .001) and was significantly different across time periods. Circadian rhythm, as represented by actigraphy, also maintained diurnal variation (P < .001) and was in phase with light. Linear regression of movement and time demonstrated a moderate relationship between light and actigraphy (R2 = 0.56).
CONCLUSIONS: Despite requiring continued high-level care and a prolonged stay in a medical facility, patients recovering from critical illness and actively weaning from PMV maintain their circadian rhythm in phase with normal diurnal variations of light.
Introduction
The ICU is disruptive to maintenance of circadian rhythm and sleep-wake cycle.1–3 Many physiologic and immunologic functions are governed by sleep and circadian rhythm; thus, it is not surprising that the maintenance of these homeostatic mechanisms has become a subject of intense research in the critically ill population.4–6 Circulating immune cells, cytokines, and components of the coagulation system have been shown to have a diurnal variation in levels. In addition, lung mechanics and gas exchange show a circadian pattern. Therefore, we can surmise that the maintenance of circadian rhythm is of great importance in the recovery from critical illness of patients requiring prolonged mechanical ventilation (PMV).7–9
Prior studies have demonstrated that there is loss of circadian rhythm in patients during critical illness with subsequent restoration of diurnal patterns with recovery and discharge from the ICU.7,8 Poor sleep quality and quantity in critically ill patients can be attributed to several possible mechanisms, including critical illness itself, mechanical ventilation, medication effects, patient care activities, and unscheduled noise and light levels.10–13 Alterations in sleep structure result in anxiety and fatigue and perpetuate circadian rhythm disruption in hospitalized patients.1,3,14–16
Although restoration of circadian rhythm has been demonstrated in patients treated in non-ICU settings, these findings have not been consistent, and the exact mechanisms responsible for precipitating and perpetuating proper circadian rhythm are unclear.17–22 Several studies have quantified the prevalence and negative effects of sleep deprivation in critically ill patients. However, there are no studies that describe circadian rhythm and sleep patterns in patients who are recovering from critical illness and requiring PMV and who are discharged from ICUs to long-term acute care (LTAC) hospitals.1–6,9–13 The aims of this study are (1) to determine the patterns of naturally occurring ambient light levels in an LTAC environment, (2) to evaluate circadian rhythm in patients recovering from critical illness and requiring PMV, and (3) to evaluate the relationship between circadian rhythm in these patients and exposure to hospital light levels. Our hypothesis is that circadian rhythm is maintained in this unique patient population and is in phase with the diurnal variation in naturally occurring ambient light levels.
QUICK LOOK
Current knowledge
Circadian rhythm regulates a number of physiologic and immunologic processes. Disruption of circadian rhythm has been demonstrated in acutely ill, mechanically ventilated patients in the ICU.
What this paper contributes to our knowledge
Patients recovering from critical illness and actively weaning from prolonged mechanical ventilation maintain their circadian rhythm in phase with normal diurnal variations of light.
Methods
This study was approved by the Institutional Review Board of the University of Maryland, Baltimore. Informed consent was obtained from all patients.
Study Design and Setting
This was a prospective observational study of patients who were recovering from critical illness and receiving PMV and who were admitted to the Comprehensive Pulmonary Rehabilitation Unit (CPRU) of the University Specialty Hospital (USH). USH is a 180-bed LTAC hospital affiliated with the University of Maryland Medical Center. The CPRU is a 14-bed, high-intensity ventilator weaning unit that emphasizes mobility and pulmonary rehabilitation. All patients participate in 1–2 h of physical and occupational therapy daily as tolerated for a minimum of 5 d/week. Care was provided by registered nurses at a 1:4 nurse-patient ratio and by respiratory therapists at a 1:7 therapist-patient ratio. Hospitalists supervised general medical care, and pulmonologists served as consultants for all patients. To preserve naturally occurring environmental cues, no specific instructions were provided for environmental regulation with respect to light, noise, and patient-staff interaction. No additional artificial lighting was provided, and patients were observed in their assigned hospital room located in the CPRU. The patients did not receive any devices (earplugs, eyeshades, bright lights, etc) to alter their natural exposure to environmental stimuli.
Patient Selection
Eligible patients were older than 18 y and were receiving PMV as defined by the National Association for Medical Direction of Respiratory Care (NAMDRC).23 Patients were eligible for the study if they were admitted to an ICU and required mechanical ventilation for > 6 h in a 24-h period for ≥ 21 d, had a tracheostomy in place, were able to interact, and were able to give verbal or written consent in English. Patients had to be actively participating in physical and occupational therapy and be able to move all four limbs spontaneously. In addition, patients were actively weaned using the facility's ventilator weaning protocol. To maximize patients' efforts at weaning, sedatives and hypnotics are typically avoided in the CPRU. None of the patients enrolled in the study were receiving any sedative or hypnotic medications. Per protocol, patients were rested at night with either increased pressure support or continuous mandatory ventilation according to their specific needs. Nursing protocol required patients to be turned every 2 h unless they were ambulatory. Tracheal suctioning was performed every 4 h or more frequently if needed. Patients were excluded from the study if they were blind, were pregnant, had a known circadian rhythm disturbance or phase shift disorder, had a brain tumor involving the pineal gland or hypothalamus, or were mentally incompetent. Severity of illness was assessed in all patients using the Charlson comorbidity index. The Charlson comorbidity index is a score that predicts the risk of mortality in 10 y. The index includes 19 possible comorbid conditions that are weighted 1–6 with a total score from 1–37. Higher Charlson comorbidity index values represent greater comorbidity and higher probability of death within 10 y.24
Data Collection
Patients were enrolled between January 2011 and February 2012. Patients were studied for a median of 6 d after admission to the LTAC hospital. Demographic information and clinical covariates, including body mass index (BMI), medications, tracheostomy days, and comorbidities, were collected. Light levels in each subject's room were measured in 30-s epochs over a 48-h period using an actigraph/luxmeter (ActiTrac, IM Systems, Baltimore, Maryland) mounted on the wall directly adjacent to the patient in a central location at eye level. The luxmeter was mounted away from patient care equipment and devices to avoid any obstruction of its light sensor. An actigraph wristwatch (MicroMini Motionlogger, Ambulatory Monitoring, Ardsley, New York) was placed on each patient's non-dominant wrist, and measurements were recorded using zero crossing mode. Motion was detected in 1-min epochs continuously over the 48-h study period for each patient.
Data Analysis
Light levels and actigraphy data were collected continuously over 30-s epochs. Although light levels were collected via the luxmeter over 30-s epochs, only the 1-min epoch data were used for analysis to maintain consistency with the actigraphic data collected over 1-min epochs. Light levels and actigraphy data from 1-min epochs were then averaged into 4-h periods. Data were grouped into six time periods: 2 pm to 6 pm, 6 pm to 10 pm, 10 pm to 2 am, 2 am to 6 am, 6 am to 10 am, and 10 am to 2 pm. Four-hour periods were chosen, as prior investigation has demonstrated accuracy and resolution when monitoring circadian rhythms using urinary melatonin level.10 In addition, 4-h time periods were thought to be adequate to determine any significant changes in activity levels and light levels throughout the day. Light levels were processed with ActiTrac 8.54 software. Actigraphy data were processed with Action 4 software. Mean light levels and actigraphy data were compared at 4-h time periods and in between the two 24-h periods using two-way analysis of variance for repeated measures, with time and day as independent variables. If a significant result was found, a post hoc analysis (Holm-Sidak) was performed to determine the significant comparisons. Data were collated and expressed as mean ± SD unless noted otherwise. Linear regression was performed comparing total activity level as measured by actigraphy (dependent variable) and light (independent variable). R2 was calculated to determine the proportion of variance in activity explained by changes in light levels. Statistical analysis was conducted using statistical software (SigmaPlot 11.0, Systat Software, San Jose, California). The null hypothesis was rejected at the 5% level.
Results
Twenty patients were assessed for inclusion into the study. After exclusion of 5 patients, 15 patients remained for analysis (Fig. 1). Table 1 shows demographic and clinical data. Patients were studied various times during the first 3 months of admission to the CPRU. Mean BMI was 32.7 ± 10.3 kg/m2. Eight patients were obese (BMI ≥ 30 kg/m2), and 4 patients were morbidly obese (BMI ≥ 40 kg/m2). Patients had multiple comorbidities as shown in Table 2, with congestive heart failure being the most prevalent (73%). Comorbidity burden, as measured by the Charlson comorbidity index, was 5.5 ± 2.6. During the 48-h observation period, 10 patients were on pressure support weaning trials, 3 patients were able to tolerate tracheostomy collar trials, and 2 patients required continuous ventilator support during that period because of an inability to wean.

Patient enrollment.
Demographics and Characteristics of 15 Patients Admitted for Weaning From Prolonged Mechanical Ventilation
Major Comorbidities Present on Admission to Long-Term Acute Care Hospital
A total of 2880 light measurements were obtained using an actigraph/luxmeter. Light levels remained low over the course of the 48-h monitoring period, with an average maximum level of 145.3 ± 156.4 lx/min, yet maintained diurnal variation (Fig. 2). A total of 2880 movement measurements were obtained via actigraphy. Light and movement data were grouped into the previously mentioned 6 time periods. All patients demonstrated light and activity that maintained diurnal variation and that were highest during daytime hours and lowest during nighttime (Fig. 3). Linear regression of movement as a function of light demonstrated a moderately strong relationship (R2 = 0.56) (Fig. 4).

Light levels during the 48 hour study period. The minimum and maximum horizontal bars represent the 10th and 90th percentiles, respectively. The shaded areas show the 25th to 75th percentiles, with the horizontal bars in the shaded areas representing the median value. The circles indicate the minimum and maximum values recorded.
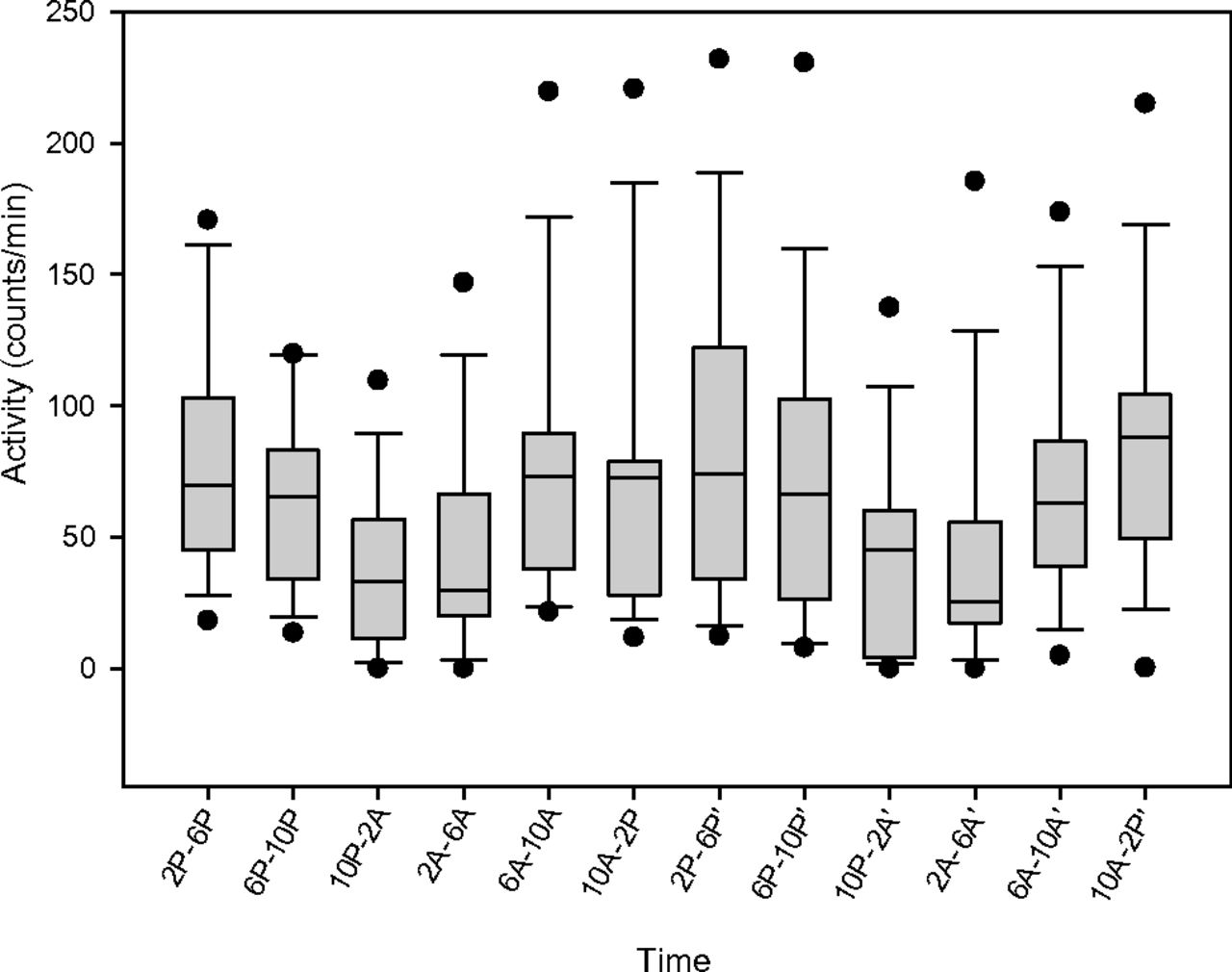
Movement during the 48 hour study period. The minimum and maximum horizontal bars represent the 10th and 90th percentiles, respectively. The shaded areas show the 25th to 75th percentiles, with the horizontal bars in the shaded areas representing the median value. The circles indicate the minimum and maximum values recorded.
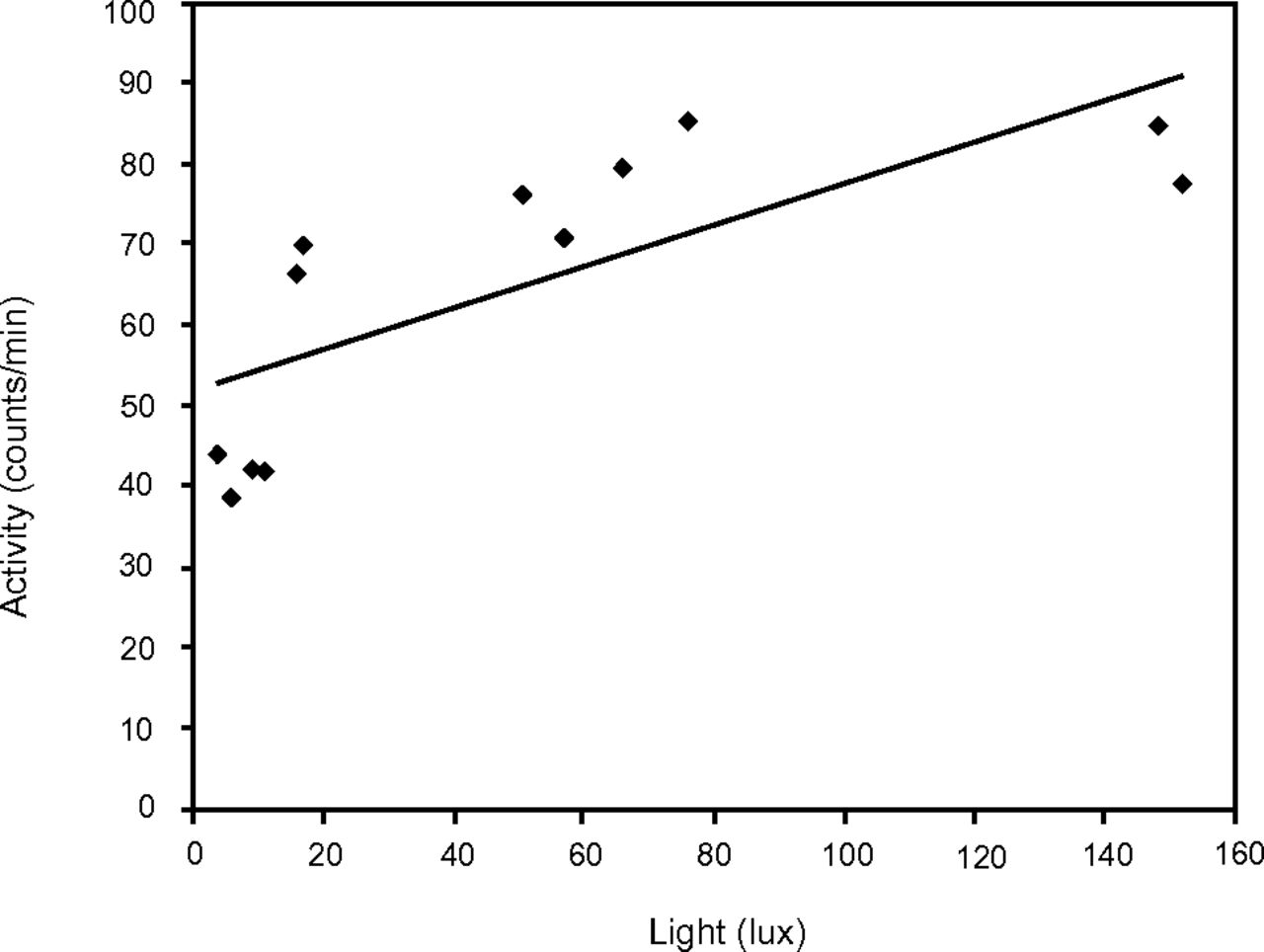
Average movement according to light level data. Linear regression curve R2 = 0.56.
Two-way analysis of variance for repeated measures using day and time as independent variables and light (see Fig. 2) and actigraphy (see Fig. 3) as dependent variables revealed significant differences in both light and actigraphy levels across time (P < .001). No significant difference in light or actigraphy was noted between the 2 d when matched for times. For light levels (see Fig. 2), the values during midday (10 am to 2 pm) were significantly greater (P < .001, Tukey honest significance test) than levels at all other times, except for the 6 am to 10 am period. Activity levels (see Fig. 3) were significantly greater during the daylight hours (6 am to 10 am, 10 am to 2 pm, and 2 pm to 6 pm) compared with the nighttime hours (6 pm to 10 pm, 10 pm to 2 pm, and 2 am to 6 am) (P < .001, Tukey honest significance test). Activity levels during the daylight hours were not significantly different from each other. Similarly, activity levels during the nighttime hours were not significantly different from each other. Thus, light and activity were found to be in phase and maintained diurnal variation, being highest in the daytime and lowest during nighttime.
Discussion
We found that LTAC patients recovering from critical illness and receiving PMV maintained circadian rhythm as represented by actigraphy. In addition, naturally occurring ambient light levels, although low, maintained a diurnal periodicity in patient care rooms. Finally, it was found that circadian rhythm was in phase with environmental cues, as peak light levels coincided with peak movement levels and demonstrated a significant difference between peak and nadir light levels. This suggests that although light levels were low, they were still present in sufficient intensity to entrain circadian rhythm in this population.
To the best of our knowledge, our study is the first study to demonstrate that LTAC patients who are recovering from critical illness and who are actively weaning from mechanical ventilation maintain their circadian rhythm by exhibiting uniformly occurring peak and trough levels of activity within a 24-h period. Our conclusions in this population are different from previous findings in acutely critically ill patients, using melatonin levels to determine circadian rhythmicity.10,11,15–17,25 In these studies, circadian rhythm was consistently impaired in the setting of critical illness and mechanical ventilation. Because our study focused on less acutely ill, post-ICU patients, it is possible that the maintenance of circadian rhythm reflects our study population's improved physiology. It has been demonstrated that recovery from critical illness is associated with decreased catecholamine and inflammatory mediator release, both of which perpetuate sleep disturbances.5,25
A second explanation of these patients' maintained circadian rhythm may be attributed to their improved response to environmental and social cues. At sufficient levels (150–180 lx), light has been shown to be the primary stimulus for entraining circadian rhythm.26,27 We demonstrated that the light levels in our LTAC unit were present in cycles appropriate to normal sleep-wake cycles, although they lacked intensity. Because we chose to study the circadian response to variations in naturally occurring light levels within the LTAC weaning unit, we did not need to adjust for seasonal variation over the study period. Linear regression further demonstrated the positive relationship between light and circadian rhythm, as represented by actigraphy. The exposure to proper diurnal variation in light levels in our patient population likely contributed to entrainment and maintenance of their circadian rhythm. Additionally, all patients were actively participating in pulmonary rehabilitation and were conscious and socially interactive. Although the majority of the patients (one of 15) were fed via gastrostomy tube, oral intake at regular mealtimes was encouraged in all patients. The presence of these zeitgebers is unique to our study compared with previous studies in the ICU setting, in which important environmental stimuli may be lacking.
Ventilator mode may have contributed to our finding of increased daytime activity with actigraphic representative sleep at night. Several studies have shown that mechanical ventilation disrupts sleep and circadian rhythm in acutely critically ill patients.13,16,28–32 Some studies have shown that a higher percentage of sleep occurs during daytime compared with nighttime in mechanically ventilated patients.13,32 Other studies have looked extensively into the mode of ventilation as a contributor to sleep arousals and have noted continuous mandatory ventilation and, more recently, Neurally Adjusted Ventilatory Assist ventilation as conducive to maintaining high sleep quality in mechanically ventilated patients.31,32
Despite all patients receiving pressure support ventilation at some point during the observation period, all maintained their circadian rhythm. This contrasts with previous studies that have shown that pressure support ventilation is associated with increased arousals during sleep.31,32 The fact that most of the patients were able to breath spontaneously at least some of the time during the study may have contributed to their maintenance of circadian rhythm.
The mean age of our cohort was slightly younger than previous work focusing on LTAC patients weaning from prolonged mechanical ventilation.33 This may have been the result of our inclusion criteria, which required that all patients were functional, with all four limbs capable of spontaneous and purposeful movement. In addition, all patients were cognitively intact and able to participate in high-level physical therapy. Thus, our study may not be generalizable to all LTAC populations but rather applies to higher functioning patients who are actively weaning.
We analyzed light levels in the LTAC unit and associated them with circadian rhythm as represented by actigraphy. In contrast to the ICU setting, we found appropriate diurnal variation in light levels in our LTAC unit. Studies based in ICUs caring for acutely ill patients frequently show poor diurnal variation in light, which may also contribute to loss of circadian rhythmicity in the acute care setting.7,18–20,34 Exposure to short periods of high-intensity light and darkness did not stimulate melatonin secretion in a small cohort, which may indicate that the physiologic and psychologic changes associated with critical illness and the lack of environmental zeitgebers play a large role in loss of circadian rhythm in critical illness.28 Additionally, our group has shown that despite exposure to a diurnal variation in light levels, circadian rhythm is not entrained in ICU patients. The difference in light levels between an LTAC facility and acute care units is likely multifactorial and related to differences in unit design, incorporation and orientation of windows, nursing and institutional practices, and patient preferences.1,3,11,14
Although actigraphy is a validated noninvasive tool for monitoring the sleep-wake cycle, it may overestimate sleep in inpatients because of increased sedentary time.35–37 However, in critically ill patients, measurement of limb movement via wrist actigraphy has been shown to correlate with activity levels and sedation levels in critically ill patients.38,39 Given the principles of using actigraphy as a surrogate for sleep and circadian rhythm (activity representing wake time, and lack of movement representing sleep) our findings of the presence of increased motion during daytime hours and the lack of motion during nighttime hours are consistent with appropriate circadian rhythm despite the possibility that the actigraphy may have missed some subtle movements. Thus, we believe that the use of actigraphy is an appropriate marker for activity and circadian rhythm in this population. Light data collection may vary depending on weather changes, season of the year, latitude, room location, and individual nursing practices on the data collection days. Nevertheless, as we did not institute any changes in environmental or nursing care practices, the levels recorded are typical of patient exposure in our hospital. Finally, a biomarker of circadian rhythm, such as melatonin or cortisol, was not obtained. Prior studies have demonstrated an association between poor sleep and circadian rhythm with increased mortality, prolonged ICU stay, and delirium in critical illness. The use of serum or urinary melatonin levels to determine maintenance of circadian rhythm and its correlation with outcomes in patients receiving PMV may deserve further attention. However, movement as detected by actigraphy is a validated modality of quantifying circadian rhythm and thus is an appropriate metric.35–37
Conclusions
LTAC patients who are actively weaning from prolonged mechanical ventilation after recovering from critical illness maintain their circadian rhythm. We demonstrated an association between diurnal variation of light levels and movement measured using actigraphy. Further studies may improve our knowledge about optimizing circadian rhythmicity and its effects on improving patient outcomes.
Footnotes
- Correspondence: Avelino C Verceles MD, Division of Pulmonary and Critical Care Medicine, University of Maryland School of Medicine, 110 South Paca Street, Baltimore, MD 21201. E-mail: avercele{at}medicine.umaryland.edu.
Dr Verceles was supported by National Institute on Aging grant P30 AG028747. The authors have disclosed no conflicts of interest.
- Copyright © 2014 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}
{kind=link}