

Abstract
BACKGROUND: The study objective was to determine differences in the proportion of supranormal pulmonary function tests (PFTs) between active duty (AD) military personnel and a similar non-active duty (non-AD) population. Given the emphasis on cardiovascular fitness in the military, it has been hypothesized that regular exercise in this cohort leads to an increased proportion of supranormal PFTs. We hypothesized that a comparison of PFTs would identify no differences in the ratio of supranormal to normal PFTs between the AD and non-AD populations.
METHODS: A retrospective chart review was conducted of all PFT studies at the Brooke Army Medical Center from 2006 to 2011. Studies were included with either an FVC or FEV1 > 110% of predicted, with both values > 100% of predicted. A comparative analysis was performed for patients between 18 and 50 years of age based on AD status. Further analysis was performed on all ages to determine the distribution of supranormal findings in the entire study population.
RESULTS: A total of 16,600 interpreted PFTs were queried. Of those, 4,303 (31.6%) were AD patients, and 9,306 (68.4%) were non-AD patients. From all of the PFTs reviewed, a total of 912 (6.7%) were identified as supranormal. When further analyzed, 381 (9.4%) of AD patients 18–50 years old were supranormal, 175 (12.4%) of non-AD patients 18–50 years old were supranormal, and 356 (4.7%) of non-AD patients older than 50 years were supranormal.
CONCLUSIONS: This study revealed no significant difference in the proportion of supranormal-to-normal PFTs in an AD versus non-AD duty population of the same age range. Based on these findings, no assumption should be made that supranormal PFTs are more common in military personnel. Interpretation of normal PFTs in AD personnel undergoing evaluation should not differ from that in any typical patient.
Introduction
Dyspnea is a frequently evaluated complaint among the active duty (AD) population of the United States military. In part, military personnel may be referred for clinical evaluation due to their inability to meet the physical requirements of military service and specifically the standards for a timed physical fitness run. Although asthma and exercise-induced bronchospasm are often the cause of exertional symptoms, many initial clinical evaluations based on pulmonary function testing (PFT) and chest imaging are negative. Twenty-five percent of AD military personnel with complaints of exertional dyspnea had a negative comprehensive evaluation.1 Given the recent emphasis on post-deployment respiratory symptoms and the possible relationship with environmental exposures such as sand storms and burn pits, many military personnel being evaluated for respiratory symptoms are found to have normal baseline PFTs.2,3 Some clinicians have theorized that the AD military population, with a high level of emphasis on regular physical fitness compared with their non-AD counterparts, has a larger proportion of supranormal PFT values. This has lead to a supposition that a “normal” spirometry in an AD service member presenting with dyspnea actually reflects a decrement in function and underlying lung disease.3 Although spirometry reference equations such as National Health and Nutrition Examination Survey (NHANES) III establish both an upper and lower limit for normal, the upper limit of normal is not routinely calculated on spirometry reports. How does a clinician interpret spirometry either in those patients referred for a baseline study due to military occupational exposures or in those symptomatic individuals presenting with cough, dyspnea, or other respiratory complaints other than with established population guidelines?
Intense aerobic training does have a direct impact on overall cardiovascular function, muscle strength and endurance, and hematologic indices.4 However, data are inconclusive regarding the change in lung function in high-level aerobic performers. Studies comparing athletes and individuals in high-performance professions with untrained control groups provide little evidence that high demand of lung function changes the underlying PFT values.5 The results of these studies led many investigators to question whether the minor increases in lung function found in conditioned versus non-conditioned subjects were induced by training or present prior to training. Conversely, several studies of elite athletes for the diagnosis of exercise-induced bronchospasm have noted elevated baseline values in this population.6,7 Given the current lack of evidence supporting the correlation between increased levels of fitness and supranormal PFTs in elite athletes, the suggestion that the military population would comprise more supranormal PFT values than the general population has not been investigated. Although many members of the military achieve and maintain a high level of physical fitness, the average military member is not a highly conditioned elite athlete. We hypothesized that a comparison of PFT data from both AD military and non-AD beneficiaries would not demonstrate an increase in supranormal values.
QUICK LOOK
Current knowledge
Dyspnea is a frequent complaint among the active duty population of the United States military. Military personnel may be referred for clinical evaluation due to their inability to meet the physical requirements of military service, specifically the standards for a timed physical fitness run.
What this paper contributes to our knowledge
The physical requirements of military service do not alter the normal distribution of pulmonary function results. There was no difference in pulmonary function test results between active duty military personnel and a similar cohort of civilians.
Methods
This study was conducted as a retrospective review of Department of Defense electronic medical records after obtaining written approval from the local institutional review board. The electronic database repository for all PFT studies conducted at the Brooke Army Medical Center was queried from 2006 to 2011. All studies were performed on a spirometer (SensorMedics Vmax-22, CareFusion, San Diego, California), which was calibrated on a daily basis following the manufacturer's recommendations. Individual spirometry examinations were reviewed, and those with an elevated FVC or FEV1 > 110% of predicted (based on NHANES III reference values) were identified.8 To qualify for inclusion in this study, both the FEV1 and FVC were required to be > 100% of predicted. Spirometry reports from our laboratory do not calculate the upper limit of normal based on CI, and the percent of predicted was used as a surrogate to compare populations. Studies that did not meet American Thoracic Society guidelines for acceptability and repeatability were excluded from further analysis. Specific note was also made for patients with either FEV1 or FVC > 120% of predicted. The percentage of percent-of-predicted values (110% and 120%) that were above the calculated 95% CI based on the NHANES III upper limit of normal for FEV1 and FVC was also determined for the included studies. From these studies, the following information was obtained: (1) patient demographics (age, gender, ethnicity, and height); (2) patient military status (AD, retired, or military dependent); (3) spirometry results (actual, predicted, and % of predicted) to include FEV1, FVC, and FEV1/FVC; and (4) if performed, total lung capacity (TLC), residual volume (RV), and diffusing capacity for carbon monoxide (DLCO).
Results were divided into 3 groups of patients for analysis: (1) AD military 18–50 years old, (2) non-AD patients 18–50 years old, and (3) military retirees or dependents 51–90 years old. The percentage of studies meeting the inclusion criteria was calculated from the overall number of studies performed based on diagnostic procedure codes obtained for the pulmonary clinic during the study years. Values were calculated for AD and non-AD patients by groups and age ranges.
Statistical analysis was performed using commercially available software (SPSS 16 and SAS 9.3, SPSS, Chicago, Illinois). Statistical comparison of the three groups was done with a one-way analysis of variance for the following variables: FVC (% predicted), FEV1 (% predicted), and FEV1/FVC (actual). Post hoc analysis was performed if the primary analysis failed to reach significance. Additional analysis included differences between groups based on RV (% predicted), TLC (% predicted), and DLCO (% predicted) values. Direct comparison of the 18–50 AD and non-AD groups was performed using a paired t test assuming equal variance. A final analysis was also performed to evaluate for any differences in PFT values based on gender or ethnicity. To compare the actual FEV1 and FVC for AD and non-AD across ages 18–50 y, a Z score was calculated for all patients. The Z score was calculated by taking each patient's absolute FEV1 and FVC measures, subtracting the mean, and dividing by the SD, with respect to their gender and age group (18–20, 21–30, 31–40, and 41–50 y). The Z scores for AD and non-AD were then compared using a t test for both the FEV1 and FVC measures.
Results
A total of 16,600 PFTs performed at the Brooke Army Medical Center between 2006 and 2011 were queried in this study. Of those, 32% were identified as AD patients, and the remaining 68% were non-AD patients, either military retirees or dependent family members. Further division of the non-AD duty patients identified by the 18–50- and 51–90-year age groups identified the percentages as 11–57%. The number and percentage of supranormal spirometry values for each group and the total cohort are shown in Table 1. For the total cohort, 912 (5.5%) were found to have supranormal values at 110% of predicted, and 248 (1.5%) had either FEV1 or FVC > 120% of predicted. The highest percentage of supranormal values at 9.7% was found to be in the 18–50-year-old non-AD group. The remaining demographic information is also given in Table 1. Notably, the overall gender distribution was 40% male and 60% female, but the AD group had a higher percentage of males at 57%. The percentage of military retirees (vs dependents) in the 50–90-year age group was 41%.
Patient Demographics
The PFT values for each group are shown in Table 2. Eighty-nine percent of studies with FVC > 120% also exceeded 95% CI, whereas only 32% exceeded 95% CI at 110% of predicted. For FEV1 > 120% and 110% of predicted, the percentage of studies above 95% CI were 78% and 26%, respectively. When all 3 groups were analyzed and found to have a normal distribution, a significant difference for FEV1 (% predicted) is shown, which can be accounted for by the higher FEV1 in the 50–90-year age group. Further subset analysis using a paired t test showed no statistical difference between the 18–50-year-old AD and non-AD groups for FEV1 (% predicted) (P = .927). The differences seen in FEV1 account for the significant difference seen in FEV1/FVC across all 3 groups; no difference exists between the 18–50-year-old AD and non-AD groups (P = .736) when directly compared. Analysis of TLC, RV, and DLCO as shown in Table 2 also showed a significant difference for TLC (P < .005) and DLCO (P < .005), which can be accounted for by the decrease in both values in the 51–90-year age group.
Comparison of Pulmonary Function Test Values for Active Duty and Non-Active Duty Groups
To further define the distribution of PFT values within this cohort, Z scores were calculated for the AD group (18–50 y) and the non-AD group (18–50 y) by gender and across age ranges. The results are shown in Table 3 and demonstrate statistical differences in actual FEV1 and FVC between the AD and non-AD groups (P < .001). However, when calculated using Z scores, there is normal distribution of both FEV1 and FVC, with P = .15 and .36, respectively.
Z Score Analysis
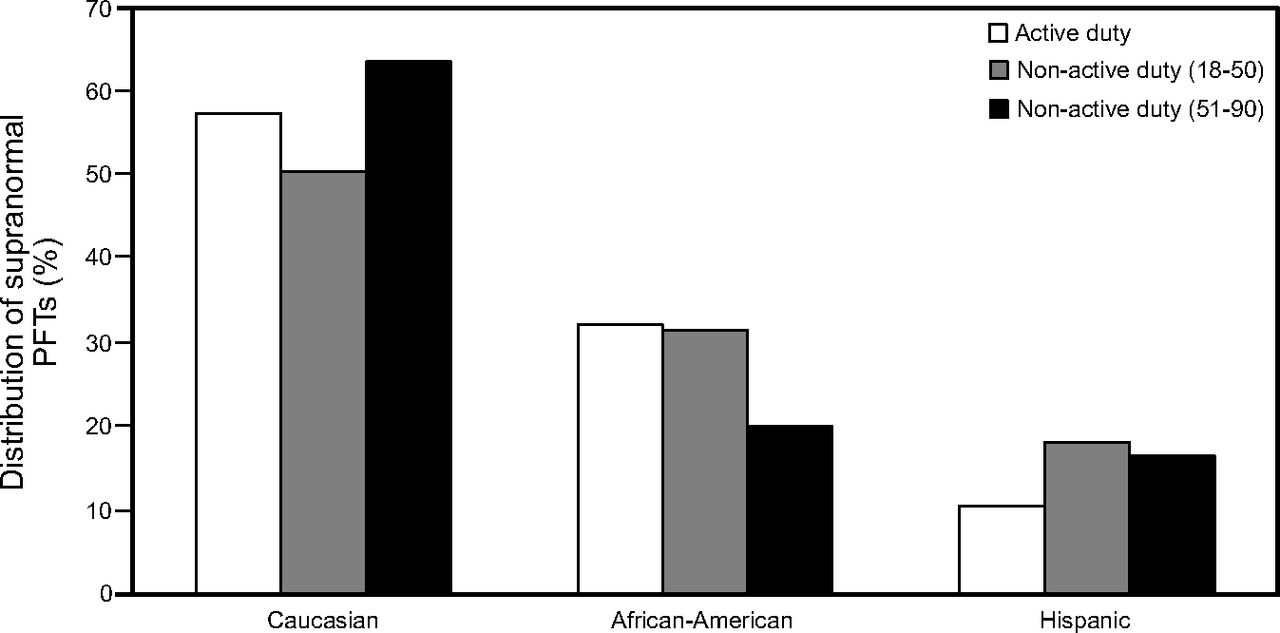
Distribution of the supranormal values was further analyzed by year of study and age ranges. Figure 1 shows the distribution of supranormal PFTs based on year of study. There were more PFTs completed in 2006 and 2007, but the non-AD population consistently had a higher percentage than the AD population for all years. The distribution of supranormal PFTS by age range is shown in Figure 2. A higher percentage of PFTs with supranormal values is seen in the 18–20-year age group but is evenly distributed between AD and non-AD persons. This is a consistent finding for the 20- , 30- , and 40-year age groups, with 7.6%, 7.2%, and 7.1% of all patients supranormal, respectively, with decreasing percentages in older age groups. Distribution by ethnicity (Caucasians, African-Americans, and Hispanics) is shown in Fig. 3, where there are similar percentages for supranormal values for the AD and non-AD groups.

Percentage of supranormal pulmonary function test (PFT) values divided by non-active duty and active duty per given year. Higher percentages are seen for each given year for the non-active duty persons.

Percentage of supranormal pulmonary function tests (PFTs) for each age group for both non-active duty and active duty persons. Higher percentages are seen in the 18–20-year age group but remain consistent for the next 3 age deciles.
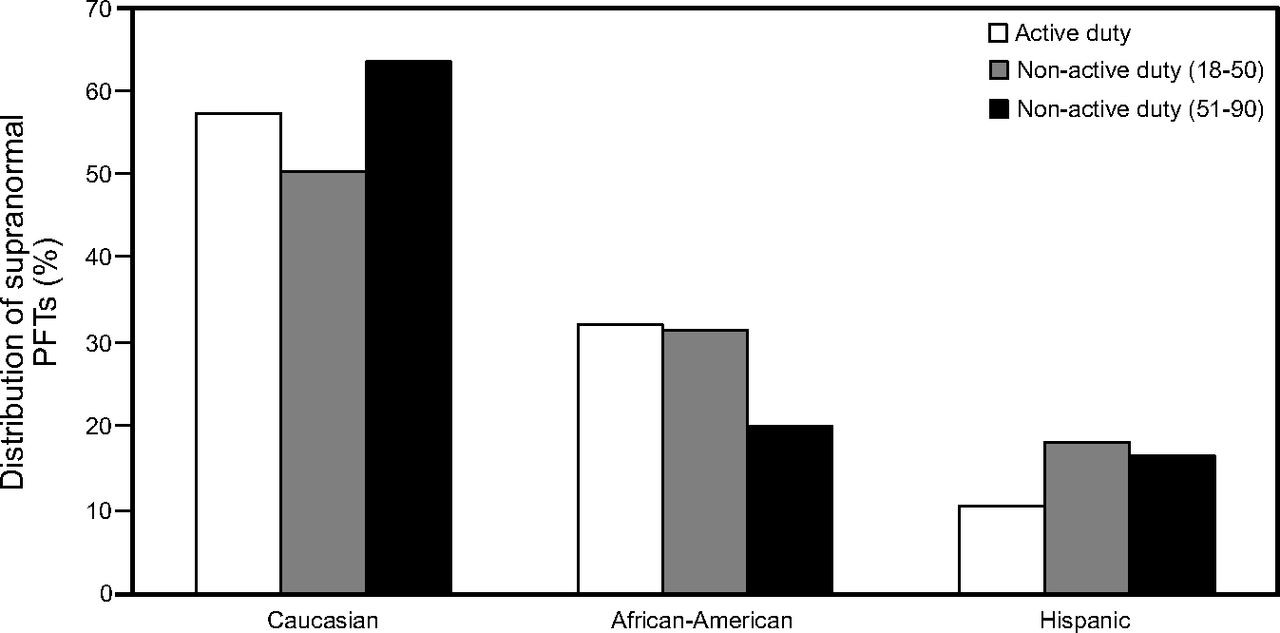
Distribution of supranormal pulmonary function tests (PFTs) by ethnicity (Caucasian, African-American, or Hispanic) for the three study groups. Similar percentages were found for each ethnicity.
Notably, the non-AD population included more female than male studies: 86% female versus 14% male in the non-AD 18–50-year age group and 65% female versus 35% male in the non-AD 51–100-year age group. The AD population was comprised of a higher percentage of male patients (57% male versus 43% female). Analysis for differences in PFT values (FVC, FEV1, and FEV1/FVC) for both males and females between groups demonstrated significance for FEV1 and FEV1/FVC (P < .001). Post hoc analysis again yielded no significant difference when the gender-based AD 18–50-year age group was compared with the non-AD 18–50-year age group for both FEV1 and FVC.
Discussion
Minimal information has been previously published on the frequency or significance of supranormal PFTs. Understandably, if elevated values are found during the performance of spirometry in a symptomatic patient, this finding is not typically indicative of a disease process and reassures the clinician that an obstructive or restrictive process is not present. Based on current population studies and spirometry reference values (eg, NHANES III), the derivation of expected normal values should be closer to 100% of predicted because of normal population distributions. However, knowing the baseline spirometry value of any given patient can be important in determining the presence or absence of pulmonary disease, as it can identify individual changes in pulmonary function over time. Especially in a younger, more fit population, does a normal spirometry in the presence of symptoms represent active pulmonary disease? This study has begun to answer several questions regarding supranormal PFT values. First, supranormal values were a common finding across all age ranges in our population and did not favor a specific age group where more comprehensive reference values may be lacking. Second, differentiating between AD personnel and their non-active counterparts did not demonstrate an increased frequency of supranormal PFT values. On the basis of this study, we have reservations about automatically defining the AD military population as having supranormal values on PFTs.
The joint American Thoracic Society/European Respiratory Society recommendations on pulmonary function testing and interpretation were published in 2005 and made several important changes.9 The primary change included incorporation of variances in the published reference equations from a higher percentage of minority populations.8 In addition, interpretation was changed to incorporate 95% CIs to define the lower limit of normal. There are multiple factors that can influence the performance of spirometry, and they are related primarily to patient effort and ability to consistently reproduce the forced expiratory maneuver. Incorrect height and age may drastically alter the predicted value, and thus incorrectly, the percent of predicted may be in the normal or supranormal range. Although both the upper and lower limits of normal for most reference equations are established, generally there is no clinical use of the upper limit of normal in the interpretation of spirometry. It is presumed that a patient being evaluated for pulmonary disease with normal values for FEV1, FVC, and FEV1/FVC would not have significant disease. In many instances, the evaluation for the presence of pulmonary abnormalities may end with a normal spirometry. In those evaluations in which there is concern for occupational disease, serial PFTs are used to detect significant clinical change. However, as the discussion in the American Thoracic Society guidelines adequately points out, there is a vast difference in the evaluation of healthy subjects and patients with disease or symptoms. Applying the same concept of “normal” based solely on PFT findings would be inappropriate, and the interpretation very much depends on the clinical question being asked.10
Early investigations suggested an increase in lung function during adolescence, especially noted in those individuals with high levels of activity.11,12 One particular group with supranormal values includes competitive swimmers due to their particular type of exercise. An Australian study of 8 swimmers compared with 8 runners showed higher FEV1 and FVC in the swimmer group, which were related primarily to an increase in chest wall width.13 This confirmed earlier findings in several other small studies of swimmers.14,15
Given the hypothesis that highly athletic individuals have supranormal PFT values, the published literature on PFTs in competitive athletes should provide ample information. Six published articles were identified that measured resting spirometry values in long-distance runners (both marathon and triathlon participants).16–21 These studies described primarily the effect of running on PFT values and provided baseline spirometry values in small groups of highly trained athletes. Table 4 provides the demographic information along with actual and predicted values for FEV1 and FVC. From this group of 67 athletes with a mean age of 27 years, the mean FVC was 102.7%, and FEV1 was 101.6%. None of the mean values from these 6 studies reached the 110% cutoff as defined in our study, although this group was younger (27 vs 31 y) than our AD population.
Pulmonary Function Testing in Elite Athletes
Because our study is retrospective in nature, there are several limitations to the data provided. Because the spirometers in our laboratory do not identify values outside the 95th percentile for the upper limit of normal, we had to establish a cutoff for review based on the percent of predicted, which showed a modest correlation with 90% and 95% CI. Other factors such as the indication for spirometry and smoking history were not listed in the PFT report, and we were unable to distinguish between symptomatic and asymptomatic individuals. Interpretation of spirometry is limited without other pertinent clinical information such as symptoms or underlying lung disease. Additional potential biases include the comparison of AD military with dependents and retirees. We assumed an overall improved fitness for the AD group but did not have any direct measurements. Also, although the repeatability of the values within a given test is required by PFT standards, we were unable to determine in our cohort if the supranormal values could be repeated over time. Finally, there are limited large population studies with PFT reference values with which we can compare our data.
Another consideration that has been discussed is the role of spirometry screening for all military service members. Spirometry is currently not used as a screening tool in asymptomatic individuals prior to enlistment or commissioning into the United States Armed Forces. Current guidelines do not recommend “screening” for common lung diseases in the general population and limit surveillance to those individuals with potential occupational exposures. There are a multitude of confounding factors surrounding this issue, including cost, manpower, quality control, and timing of screening spirometry, that make such a proposition difficult to accomplish. The main reasons not to perform spirometry screening include: (1) the limited use of a screening test in an asymptomatic population, (2) the very small likelihood of developing future respiratory disease in this population, and (3) the burden of evaluating abnormal baseline tests that may affect military careers.
Conclusions
The assumption that AD military have elevated or supranormal PFT values by virtue of their AD status is not supported by this study. There is a fairly even distribution of supranormal values across all age groups, and there is no proof that more athletic AD military have increased values over their non-AD counterparts. Although a prospective evaluation of a larger group of AD military is warranted, current practice standards should interpret PFTs according to published guidelines and not assume an underlying disease process in AD military or elite athletes when PFTs are found to be within normal limits.
Footnotes
- Correspondence: Michael J Morris MD, Pulmonary/Critical Care Service (MCHE-MDP), Brooke Army Medical Center, 3551 Roger Brooke Drive, Fort Sam Houston, TX 78234. E-mail: michael.j.morris34.civ{at}mail.mil.
The opinions in this manuscript do not constitute endorsement by Brooke Army Medical Center, the United States Army Medical Department, the United States Army Office of the Surgeon General, the Department of the Army, Department of Defense, or the United States Government of the information contained therein.
Dr. Morris is a paid speaker for Spiriva by Pfizer/Boehringer Ingelheim. The other authors have declared no conflicts of interest.
- Copyright © 2014 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}