

Abstract
BACKGROUND: The Acute Respiratory Distress Syndome (ARDS) Network low tidal volume (VT) trial paved the ground for mechanically ventilating ARDS patients with a VT of 6 mL/kg ideal body weight (IBW). Although there is no consensus that a low VT is advantageous in non-ARDS patients, it is accepted that high VT should be avoided. Because compliance rates with ventilator recommendations are 30%, there is a need for process improvement. We postulated that a computerized screen prompt that recommended VT based on height would improve compliance with low VT. During ventilator order entry, the computerized decision tool prompts the clinician and encourages ventilation of patients at 8 mL/kg IBW, and 6 mL/kg IBW for patients with ARDS.
METHODS: A retrospective review was performed on patients who required volume controlled mechanical ventilation over a 3-y period. Subjects were chosen randomly from the respiratory records of 6 different ICUs at a single tertiary care academic center. Half of the charts selected were before intervention of on-screen prompt, and the other half were after implementation of the computerized decision tool.
RESULTS: The initial set VT ranged from 6.26 to 13.45 mL/kg IBW, with a mean of 8.92 mL/kg. After implementation of the on-screen prompt, mean VT decreased by 0.84 mL/kg to 8.07 mL/kg (P = .001) with a lower range of 4.73–11.56 mL/kg IBW. We also noted a significant decrease in the number of subjects placed on an initial VT > 10 mL/kg IBW from 20% to 4% (P = .003).
CONCLUSIONS: A computerized clinical decision tool with the preferred initial VT settings based on the patients' sex and height is a safe and reliable way to increase low VT strategy compliance across multiple ICUs. Its limitations are similar to those shared by other computer-generated prompts.
Introduction
Mechanical ventilation is a lifesaving intervention that allows for oxygenation and ventilation of patients while their underlying disease or clinical issues resolve.1 Changes in ventilator strategy over the last decade have decreased the harmful effects of mechanical ventilation. In the evolution of mechanical ventilation, many factors have emerged as causes of injury to the lung. In 1998, ARDSnet researchers demonstrated that limiting tidal volume (VT) in patients with diffuse lung injury improved outcomes and mortality.2,3 High VT and high plateau pressures were found to be injurious to the lung parenchyma and were associated with worse outcomes.4 The goal in treating patients with respiratory failure receiving mechanical ventilation is to support the patients as their illness improves while preventing ventilator-induced lung injury.4,5 A low VT approach decreases ventilator-induced lung injury in patients without preexisting acute lung injury (ALI) and suggests that a low VT strategy is beneficial in all patients.6,7 Reasons for adopting a low VT strategy in all patients include limiting the development of delayed ALI and preventing barotrauma. However, there is no consensus on the optimal initial VT in patients without ALI.8
At our tertiary care center, pilot data showed that a large proportion of our patients were receiving an initial VT of > 10 mL/kg ideal body weight (IBW). Poor compliance with ventilation strategy guidelines/expert opinions can be seen throughout the literature.9,10 Because the time to irreversible injury is short, prompt recognition of abnormal VT is imperative.3 Minimizing ventilator-induced lung injury is an integral part of patient care in the modern ICU. A system to provide optimal current recommendations to physicians entering the initial mechanical ventilation orders is necessary. Previous educational efforts through lectures, handouts, and taping IBW cards to each ventilator at our institution helped, but did not protect all patients from inappropriate settings. These efforts have been used at other institutions as well to improve education to reduce ARDS triggers.11,12
Recognizing the overestimation of IBW, it was postulated that computer data would help guide clinicians to safer initial VT based on patient height and sex. Implementations of expert rules have traditionally lagged years behind published trials showing efficacy.13,14 Eslami et al15 have demonstrated that their computer decision support system (CDSS) was effective in changing clinical practice for patients ventilated for > 24 h. We hypothesized that an immediate computer-generated prompt on initial mechanical ventilation orders could improve compliance with ordering low VT strategy at the time of initial mechanical ventilation orders and reduce the risk of patients receiving VT > 10 mL/kg IBW.
QUICK LOOK
Current knowledge
The current standard of care for ARDS patients on mechanical ventilation includes tidal volumes (VT) of 6 mL/kg of predicted body weight. Despite the mortality benefit, compliance with lung-protective approaches including low VT remains < 50%. Methods to improve compliance are needed.
What this paper contributes to our knowledge
A computerized clinical decision support tool with the preferred initial VT settings based on gender and height proved to be a safe and reliable way to increase compliance using a lung-protective, low VT approach across multiple ICUs.
Methods
Intervention
For nearly 2 decades, every patient on a ventilator at our institution had to have an immediate order set generated electronically by the physicians caring for the patient. The order set requires ventilator settings to be entered, as well as other standard orders such as mouth care, head of bed up, and hemodynamic monitoring.
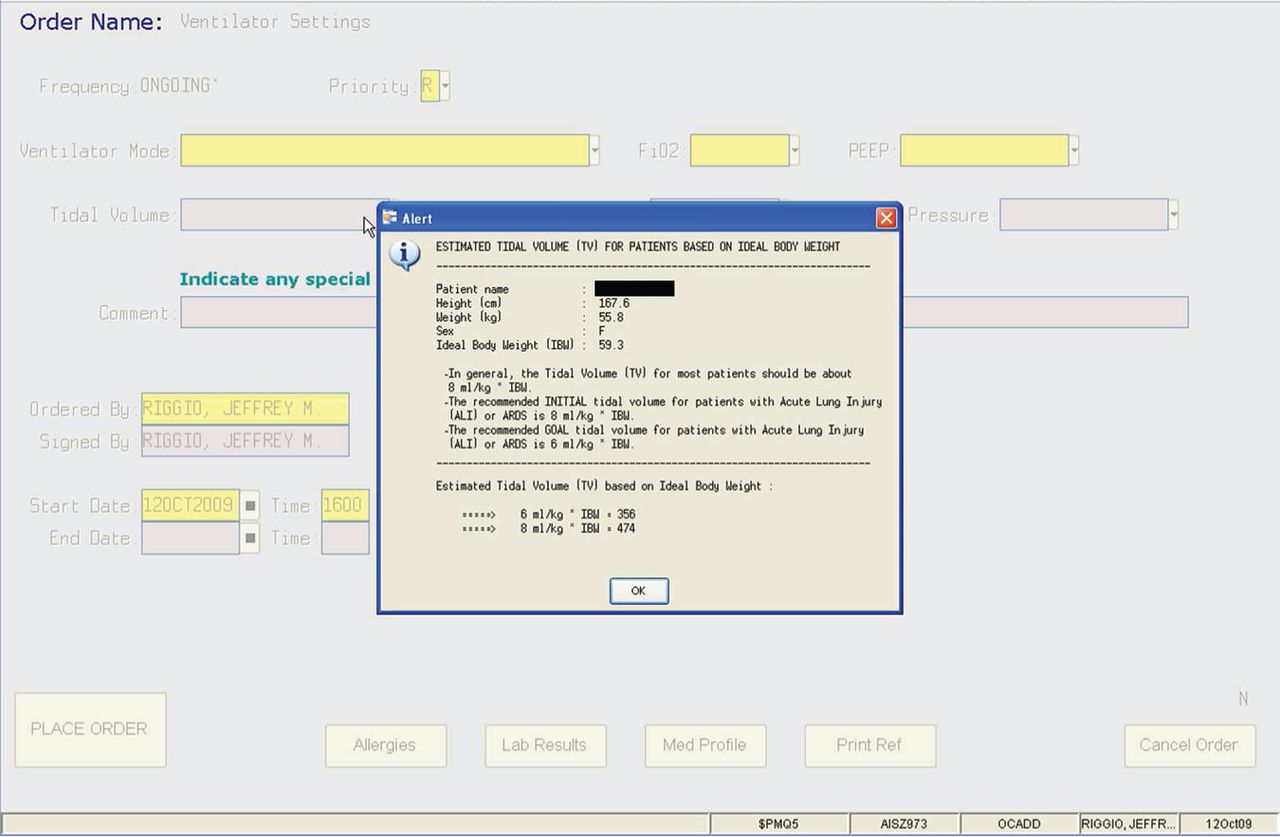
The intervention was the addition of an on-screen prompt (Fig. 1), which was triggered with each mechanical ventilation order. The computer-generated recommendation was a standard pop-up box that was displayed every time the physician initiated or changed orders for a ventilator. The on-screen prompt displayed the patient's height, sex, IBW, and recommendations for initial VT. Height and sex were already in the computer database and were previously collected as part of the admission database to help pharmacy with appropriate medication dosing. Height and weight had to be entered into the computer before entry of any hospital order. The IBW was calculated based on standard equations for ideal height to weight ratios.16 The clinicians had the option to enter any VT they wished, but they were given an actual number for the recommended VT based on the patients' recorded height and sex.

Screen shot of the automatic prompt displaying recommended tidal volume settings.
Study Design
We implemented and studied a computerized clinical decision tool, on the Centricity Enterprise (GE Healthcare, Madison, Wisconsin) platform at Thomas Jefferson University Hospital, a tertiary care academic medical center in Philadelphia, Pennsylvania, developed as an internal prompt by institutional information technologists for supporting low VT strategy. This retrospective review evaluates initial VT, based on IBW, before and after a computer-generated prompt was introduced hospital-wide on October 20, 2009 (Table 1). The order entry system had been in place for over 2 decades. The only change in practice was the addition of the pop-up decision tool to prompt clinicians to use 6 or 8 mL/kg IBW for initial ventilator settings. The prompt was a suggested VT, and the physician was able to enter any VT when finalizing order. No extra training was needed because the intervention only required the user to look at the pop-up box displayed in Figure 1, and acknowledge by selecting “OK” button. All physician order entries for mechanical ventilation (volume or pressure limited), either initial settings or change of settings, were presented with an intervention prompt and required acknowledgment before completion of orders, but we only evaluated the initial VT orders for volume controlled modes.
Timeline of Project
Study Settings
This study was performed in an urban university hospital with approximately 1,000 beds. The decision tool was implemented in all adult (age > 18 y) ICUs in the hospital. The units ranged in size from 8 to 25 beds. Many patients were referral-based, and cared for by intensivists trained in their specific subspecialty. All ICUs were staffed by full-time, academic intensivists. All units have teams of house officers to help care for patients and perform electronic order entry. As in many ICUs, the house officers rotate through the ICU on a monthly basis.
Subject Inclusion/Exclusion Criteria
The study data were collected from March 2008 to July 2010. The inclusion criteria for subjects were that they were intubated, transferred to an adult ICU during the above time period, and receiving volume controlled ventilation. Subjects were picked randomly, based on respiratory care records, from all 6 different closed ICUs. The data list of ventilated subjects was provided by the respiratory therapy department. This list was divided into 2 groups: patients cared for before and after intervention. The list was then further divided by month of admission to ensure that a variety of clinicians (resident/attending physician rotation schedules were monthly) were included for review. From each month, 1 or 2 charts were randomly (simple randomization by a non-study participant) picked from the list and retrieved for analysis. In subjects who were intubated multiple times, subsequent intubations were excluded. Ultimately, data from 240 charts were recorded for sex, height, date of intubation, mode of mechanical ventilation, and initial VT recorded on respiratory records. During the first 24 h of intubation, a diagnosis of ARDS cannot be confirmed (while ruling out other causes of respiratory failure); therefore, this was not used as an inclusion/exclusion criterion. The Thomas Jefferson University human research board approved this project.
Subject exclusion criteria were any of the following: patient was from the operating room, patient received a bone marrow transplant (because there was an insufficient sample size in the pre- and post-intervention periods), or patient was not started initially on volume control mechanical ventilation.
Statistical Analyses
Results of the study were analyzed using standard statistical techniques of paired t testing to determine the difference between 2 groups. Because the data were normally distributed, and the results showed a significant number of outliers outside of standard practice, the variance ratio test (F test) was used to calculate the reduction of variance in the high outliers. Analysis of variance detects change toward the mean that is reflected as a change of the SD.
Results
The demographics of the pre- and post-intervention groups showed similar ages of 65.6 and 64.3 y, respectively (P = .48). Likewise, subjects' height of 167.7 cm versus 170.7 cm (P = .17) and IBW (P = .79) were similar because they were based on height.16 There was no statistical difference between the groups, as can be seen in Table 2.
Demographics of Study Population
The initial set VT ranged from 6.26 to 13.45 mL/kg IBW with a mean of 8.92 mL/kg IBW. After implementation of the on-screen prompt, the mean initial set VT decreased by 0.84 mL/kg with a new mean of 8.07 mL/kg/IBW. The post-intervention range also shrank from 4.73 to 11.56 mL/kg IBW. The changes in the VT across the 6 ICUs are shown in Table 3. There was a large decrease in the number of subjects placed on an initial VT > 10 mL/kg IBW. The rate of high VT ventilation was 24 of 120 (20%), and this was reduced to 5 of 120 (4%) subjects post-intervention (P < .001). This reduction was seen across all the ICUs (see Table 4). Further analysis using the F test to compare SD (variation) of pre- and post-intervention samples found statistically significant differences overall and in specific units (surgical cardiac ICU, medical cardiac ICU, and neurological ICU).
Average Initial VT by ICU Before and After Intervention With Respective Statistical Analysis
Number of Subjects Ventilated With Initial Orders of Greater Than 10 mL/kg IBW Before and After Intervention
Pre- and post-intervention results displayed in Table 3 show multiple improvements. Average VT when comparing all pre-and post-intervention groups shows improvement with P < .001, but 4 of the 6 individual units show improvement as well. Not only is the mean improved, but the SD became narrower for all groups. The F test shows the significance of this smaller SD. The P is significant for this test in all units except for the medical ICU.
Discussion
In our retrospective review study, we noted a decrease in the initial VT after the implementation of our CDSS with on-screen prompts. The average decrease was 0.84 mL/kg. We noted a significant reduction in the number of subjects receiving a VT in excess of 10 mL/kg IBW. It is unclear from our study whether this reduction in VT had any clinical benefits; however, this was not the goal of the study. In patients with ARDS, a VT of 6 mL/kg IBW is considered the standard of care. It is uncertain that all patients requiring mechanical ventilation would benefit from a VT of 6 mL/kg IBW; however, having a VT > 10 mL/kg IBW is likely to be harmful.7 By using computer-generated prompts, we significantly reduced the number of subjects who were overventilated.
In patients without ALI, many physicians will set the initial VT above 8 mL/kg IBW. In patients with ARDS, a VT of 6 mL/kg is considered preferable, and there was a linear relationship between plateau pressure and mortality.17 The ARDSnet trial is the largest and most robust study to date to compare a VT of 6 mL/kg IBW to 12 mL/kg IBW.6 Despite clear guidelines backed by strong randomized, controlled trials in patients documented to have ARDS, adherence to low VT remains poor. Even in centers where the original trials were performed, follow-up studies have found that only 70% of patients with ALI are ventilated with a low VT strategy.18
Due to the difficulty of creating and enforcing guidelines in management of mechanical ventilation across multiple ICUs and different disciplines, we chose to initiate a simple informative screen prompt for all physicians responsible for placing initial mechanical ventilation orders. The impact of this intervention has shown a decrease in overall VT and a dramatic reduction in the percentage of patients receiving a VT likely to be injurious. This association with decreasing initial set VT and timing of intervention is encouraging, but causal relationship cannot be established in a retrospective manner. Although our sample size was relatively small, the subjects were chosen randomly, and there was a consistent effect across all the ICUs. We therefore believe that our findings are real and represent a change in the initial ventilator setting across our entire population of patients.
There are limitations to the study, in that it was a retrospective review of a single center. We do not know how often the order entry prompt was disregarded, how accurately the heights were recorded, how respiratory therapists chose initial VT before visualizing the order, or how soon after the initial orders the changes to VT were made and recorded. Another limitation was the difficulty in assessing how many different physicians placed the orders and under which physician's directions (attending to resident vs resident to intern) these orders were placed. Regardless, many positives were seen. Physicians were forced to see IBW, inexperienced clinicians were given a tool to help guide their choices, and the prompt maintained clinicians' autonomy to vary their practice when needed. Another advantage was that this was a free intervention that resulted in a difference in practice. The prompt saved time for those clinicians who would have otherwise looked up the height, and for those who did not care to look at the prompt, it took only 1 s to acknowledge. This quality improvement project has another practical aspect, as better evidence evolves about ideal ventilator settings, the tool can be modified to reflect best practices and up-to-date medicine. Furthermore, because the intervention occurred without the clinicians knowing that a CDSS intervention was being developed or studied, the Hawthorne affect was also minimized.
To our knowledge, only one other group of investigators have found a benefit of CDSS in changing clinical parameters in ventilator management.15,19 Eslami et al15 found that computers were effective in instilling change. Eslami et al19 also reported that removal of the prompt resulted in decay back to previous practice, thus showing that the reminders must occur with every ventilator order change. Our intervention used a frequent reminder model: a computer prompt was shown with every order that had to do with VT. In our study, we have demonstrated a significant decrease in the VT across all ICUs with a simple low-cost intervention that requires no training. The way this prompt appeared on the screen created no extra work for clinicians and helped improve adherence to guidelines. The success of this project has made this prompt a standard part of the order entry for all ventilator orders.
Conclusions
An on-screen, automatic visual prompt displaying initial VT settings is an effective way to improve use of a low VT strategy. This prompt calculated ideal VT based on sex and height, and also reminded clinicians to keep VT in the ARDSnet range. This tool improved compliance across multiple ICUs. The limitations are similar to those shared by other computer-generated prompts.
Acknowledgments
We thank the Jefferson Information Services & Technology staff, in particular Peggy Beattie RN MBA and Arlene Peters.
Footnotes
- Correspondence: Michael Baram MD, Jefferson Pulmonary Associates, 834 Walnut Street, Suite 650, Philadelphia, PA, 19017. E-mail: Michael.Baram{at}jefferson.edu.
None of the authors have disclosed a conflict of interest.
Dr Bagga presented a version of this paper at the 108th International Conference of the American Thoracic Society, held May 18–23, 2012, in San Francisco, California.
See the Related Editorial on Page 1310
- Copyright © 2014 by Daedalus Enterprises









{kind=link}