

Abstract
A 65-y-old Japanese man was referred to the respiratory medicine department because of abnormal radiologic findings. High-resolution chest computed tomography scans revealed a geographic distribution of ground-glass opacities and associated thickening of the interlobular septa (crazy-paving patterns) in both lower lobes. He had a habit of drinking 400–500 mL of milk and 400–800 mL of canned coffee with milk every day. A swallowing function test revealed liquid dysphagia. Bronchoalveolar lavage fluid cytology findings showed multiple lipid-laden macrophages. Taken together, these findings revealed exogenous lipoid pneumonia. We performed bronchoscopic segmental lavage therapy 3 times in the left lung. After the treatment, the radiologic findings improved in both lungs. The patient has not experienced a recurrence of lipoid pneumonia in 2 y to date. In conclusion, a case of exogenous lipoid pneumonia was successfully treated with bronchoscopic segmental lavage therapy.
- lipoid pneumonia
- exogenous lipoid pneumonia
- treatment
- milk
- bronchoscopic segmental lavage
- multiple segmental bronchoalveolar lavages
Introduction
Exogenous lipoid pneumonia is an uncommon form of pneumonia that is related to the inhalation or aspiration of fatty substances.1 Although there are reports of lipoid pneumonia being successfully treated with corticosteroids,2–4 immunoglobulins,5 and whole-lung lavage,6–10 treatment of lipoid pneumonia is not well studied, and the published literature consists only of case reports. We report a case of exogenous lipoid pneumonia successfully treated with bronchoscopic segmental lavage therapy.
Case Report
A 65-y-old Japanese man was referred to the respiratory medicine department at our hospital because of abnormal radiologic findings. He had undergone a left hepatic lobectomy 13 y prior because of hepatocellular carcinoma. The patient had no respiratory symptoms. He reported a cigarette smoking habit of 1 pack/d for 45 y, and surprisingly, he had a habit of drinking 400–500 mL of milk and 400–800 mL of canned coffee with milk every day. His oxygen saturation was 96% on room air, and his body temperature was 35.6°C. His respiratory sounds were normal, and leg edema was not observed. An arterial blood gas analysis on room air revealed a pH of 7.43, PaO2 or 82.5 mm Hg, and PaCO2 of 36.5 mm Hg. His white blood cell count was 9.9 × 103 cells/μL, C-reactive protein was 1.6 mg/dL, and the levels of serum Krebs von den Lungen-6 (KL-6) were elevated (1,255 U/mL). Pulmonary function tests demonstrated diffusion impairment as follows: vital capacity, 106.2% of predicted; FEV1, 98.1% of predicted; diffusing capacity of the lung for carbon monoxide, 74.3% of predicted; and diffusing capacity/alveolar volume, 58.5% of predicted. The laboratory data and pulmonary function tests are shown in Table 1. Chest radiography revealed bilateral reticular shadows in both the mid and lower fields (Fig. 1A). High-resolution chest computed tomography scans revealed a geographic distribution of ground-glass opacities and associated thickening of the interlobular septa (crazy-paving patterns) in both lower lobes (Fig. 1, B and C). An examination of bronchoalveolar lavage fluid (BALF) from the left B8 bronchus showed a normal total cell count (2.5 × 105 cells/mL), including 67% macrophages, 20% lymphocytes, 3% neutrophils, and 9% eosinophils. The CD4/CD8 ratio of lymphocyte subsets was 2.1. The BALF findings are shown in Table 2. The BALF appeared colorless and transparent and did not show a milky appearance. Cultures of the BALF were negative for bacterial, fungal, and mycobacterial pathogens. The BALF cytologic findings showed multiple lipid-laden macrophages (Oil Red O staining) (Fig. 2A). Lung specimens of the right B4 and B8 bronchi obtained by surgical lung biopsy showed airway-centered inflammatory lesions with foamy macrophages in the terminal air spaces (Fig. 2B). A swallowing function test revealed liquid dysphagia. Taken together, these findings revealed exogenous lipoid pneumonia.
Laboratory Data and Pulmonary Function Tests on Admission
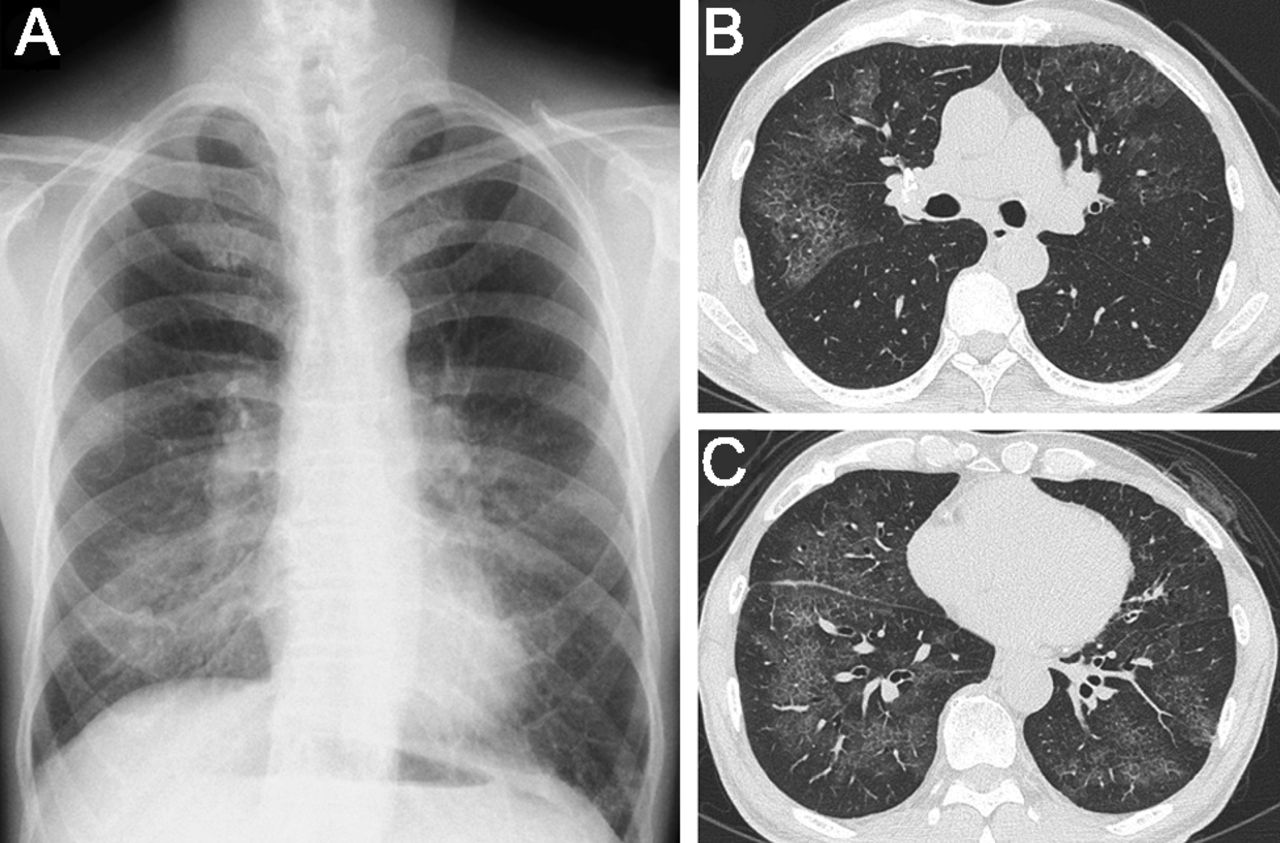
A: Chest radiography revealed bilateral reticular shadows in both mid and lower lung fields. B and C: High-resolution chest computed tomography scans revealed a geographic distribution of ground-glass opacities and associated thickening of the interlobular septa (crazy-paving patterns) in both lower lobes.
Bronchoalveolar Lavage Fluid Findings
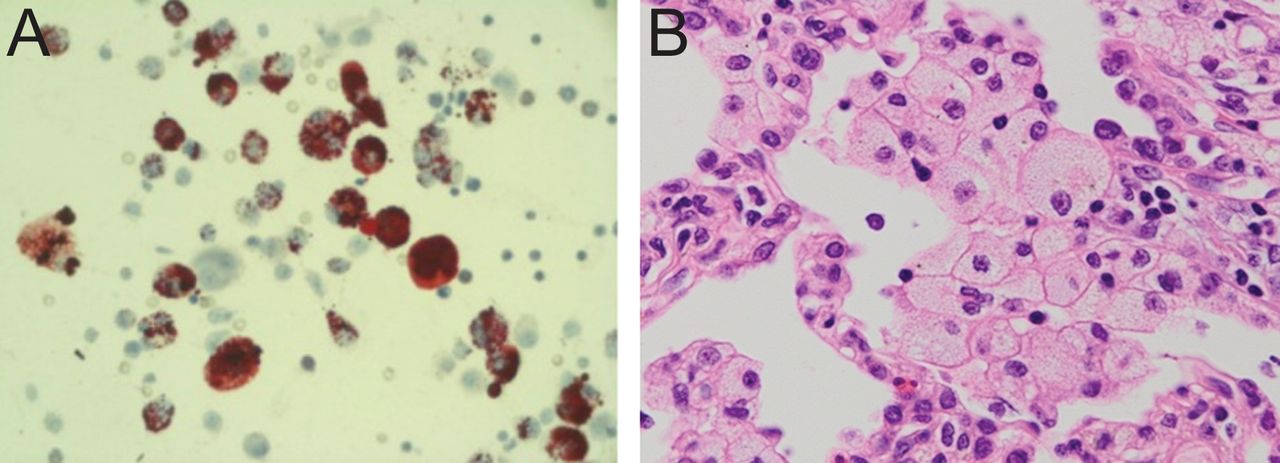
A: Bronchoalveolar lavage fluid cytology showed multiple lipid-laden macrophages (Oil Red O staining). B: Lung specimens obtained by surgical lung biopsy showed airway-centered inflammatory lesions with foamy macrophages in the terminal air spaces (hematoxylin and eosin stain).
In addition, we performed an electrospray ionization mass spectrometry analysis of the BALF pellet and milk. Two specific peaks were observed in both the BALF pellet and milk samples (Fig. 3, arrows and circles), which were not observed in BALF pellets of normal volunteers (data not shown). It was believed that these peaks were caused by monoglycerides produced in the triglycerides' resolution processes from their molecular weights. These findings indicated the possibility of milk-induced or milk-containing drink-induced exogenous lipoid pneumonia.

Electrospray ionization mass spectrometry analysis of the bronchoalveolar lavage fluid (BALF) pellet and milk at intensity 9,475 (A) and intensity 11,072 (B). Two specific peaks were observed in both the BALF pellet and milk (arrows and circles) that were not observed in BALF pellets of normal volunteers (data not shown). It was believed that these peaks resulted from monoglycerides produced in the triglycerides' resolution processes from their molecular weights.
This case received a follow-up examination because the patient had no respiratory symptoms. However, high-resolution computed tomography scans revealed extension of the ground-glass opacities and partial fibrosis after 10 months. Serum KL-6 levels were also elevated (2,300 U/mL). Pulmonary function tests revealed no remarkable changes. We performed bronchoscopic segmental lavage therapy 3 times in 15 d in the left lung, where radiologic findings had increased remarkably. For therapeutic purposes, 250-, 400-, and 250-mL volumes of warmed (37°C) sterile saline were instilled, and the recovery rates were 57%, 42%, and 76%, respectively. Chest percussion was not performed. The patient was given oral amoxicillin for a short duration to prevent infection after the bronchoscopy. He did not receive steroid therapy. We instructed the patient not to drink milk or milk-containing drinks at discharge.
Three months after the treatment, serum KL-6 levels decreased from 2,300 to 1,296 U/mL, and the radiologic findings improved in both lungs, including the right lung, where therapeutic BAL was not performed (Fig. 4). The patient has not experienced a recurrence of lipoid pneumonia in 2 y to date.
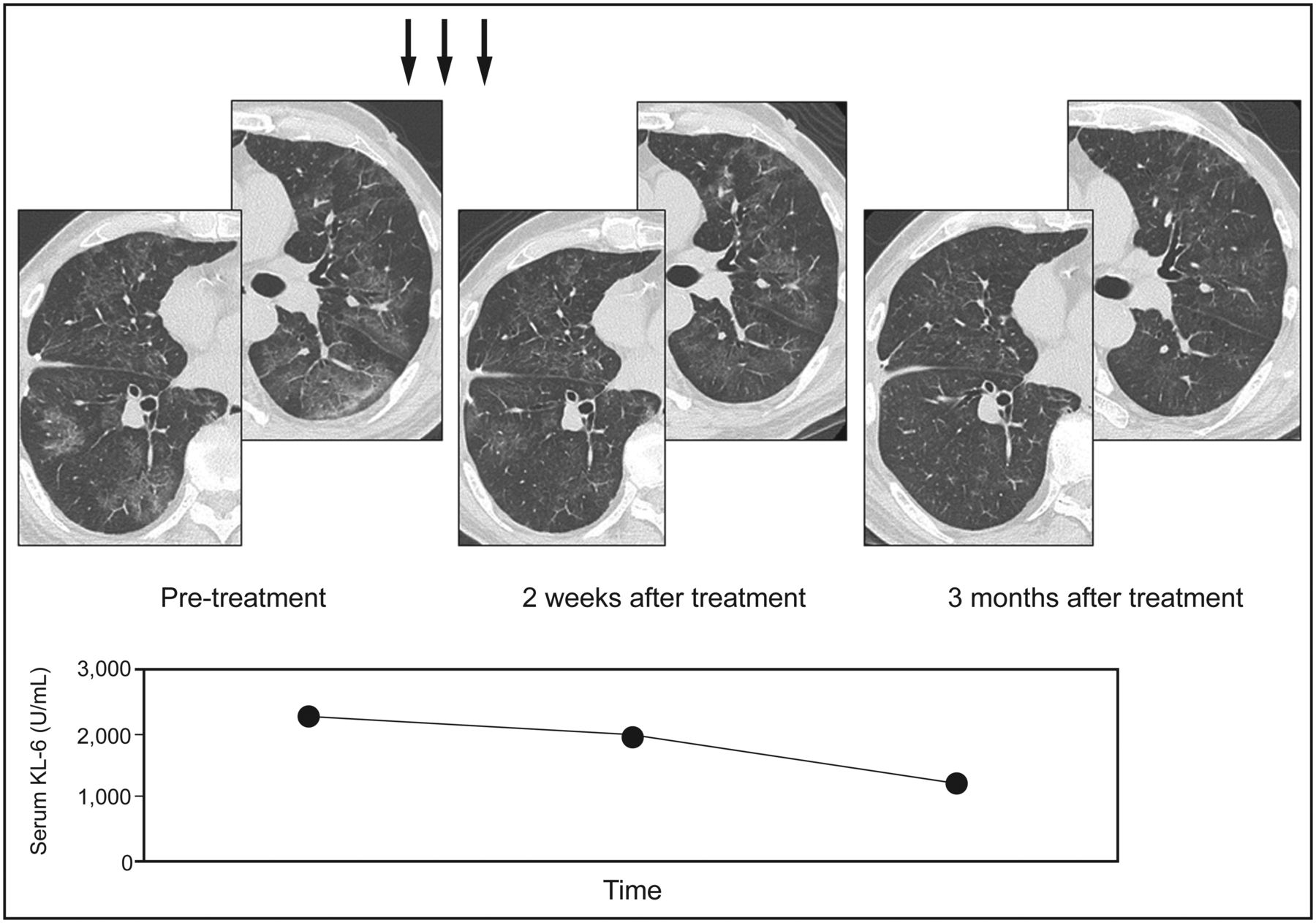
We performed bronchoscopic segmental lavage therapy 3 times in 15 d in the left lung, where the radiologic findings had increased remarkably. For therapeutic purposes, 250-, 400-, and 250-mL volumes of warmed (37°C) sterile saline were instilled. After the treatment (arrows), the levels of serum Krebs von den Lungen-6 (KL-6) decreased, and the radiologic findings improved in both lungs.
Discussion
Exogenous lipoid pneumonia is an uncommon form of pneumonia related to the inhalation or aspiration of fatty substances.1 In adults, most cases result from the use of oil-based laxatives for the treatment of constipation, followed by the nasal instillation of oily products for chronic rhinopharyngeal diseases.11 Other less commonly reported causes of lipoid pneumonia include the aspiration of milk. The diagnosis of exogenous lipoid pneumonia is based on a history of exposure to oil with radiologic findings consistent with the disease and the presence of lipid-laden macrophages in sputum or BAL analyses.12 The patient was diagnosed with exogenous lipoid pneumonia, as BALF cytology showed multiple lipid-laden macrophages.
Betancourt et al13 reported that exogenous lipoid pneumonia is classified into acute and chronic forms. Acute exogenous lipoid pneumonia is uncommon and typically caused by an episode of aspiration of a large quantity of a petroleum-based product. Chronic exogenous lipoid pneumonia usually results from repeated episodes of aspiration or the inhalation of fatty substances over an extended period.13
The patient had a habit of consuming large quantities of milk and canned coffee with milk every day. Taken together, his habits, liquid dysphagia, and the specific peaks observed for both the BALF pellet and milk on electrospray ionization mass spectrometry indicated the possibility of milk-induced or milk-containing drink-induced chronic exogenous lipoid pneumonia.
Treatment of lipoid pneumonia is not well studied, and the published literature contains only case reports. In cases of exogenous lipoid pneumonia, avoiding ongoing exposure and providing supportive care are the mainstays of treatment.1 There are reports of lipoid pneumonia successfully treated with corticosteroids,2–4 immunoglobulins,5 and whole-lung lavage.6–10 Pulmonary alveolar proteinosis can by treated with multiple segmental or lobar lavages by fiberoptic bronchoscopy using local anesthesia, which could be an alternative to a whole-lung lavage in patients with mild cases of pulmonary alveolar proteinosis.14 We chose this treatment because we thought that an immunosuppressive agent should be avoided because he suffered from hepatitis B virus infection. In addition, the patient showed a slight radiologic improvement after diagnostic BAL. We performed therapeutic BAL 3 times in the left lung, where the radiologic findings had increased remarkably. After undergoing multiple segmental lavages, the patient showed radiologic improvements in both lungs, including the right lung, in which normal saline solution was not instilled. These findings may indicate that segmental lavage therapy not only washes away lipids directly but also improves lung opacities by other mechanisms. However, the mechanisms are unclear. Hypoxemia during lavage was slight, and a lower respiratory tract infection did not occur. However, we should note that this treatment may not be effective for patients with advanced cases of exogenous lipoid pneumonia.
In conclusion, exogenous lipoid pneumonia was successfully treated with multiple bronchoscopic segmental lavages. Bronchoscopic segmental lavage therapy could be a therapeutic option for exogenous lipoid pneumonia.
Acknowledgments
We thank Naoya Kishikawa MSc, Mohamed Saleh Elgawish MSc, and Naotaka Kuroda MSc (Graduate School of Biomedical Sciences, Course of Pharmaceutical Sciences, Nagasaki University, Nagasaki, Japan) for performing the electrospray ionization mass spectrometry analyses. Editage provided editorial assistance.
Footnotes
- Correspondence: Yuji Ishimatsu MD PhD, Second Department of Internal Medicine, Nagasaki University School of Medicine, 1-7-1 Sakamoto, Nagasaki 852-8501, Japan. E-mail: yuji-i{at}nagasaki-u.ac.jp.
The authors have disclosed no conflicts of interest.
- Copyright © 2015 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}
{kind=link}