

Abstract
BACKGROUND: Foreign body aspiration is an uncommon entity in adults. Herein, we describe our experience with flexible bronchoscopy in the removal of tracheobronchial foreign bodies in adults. We also conducted a systematic review of the literature on the topic of foreign body inhalation in adults managed with flexible bronchoscopy.
METHODS: The bronchoscopy database (from 1979 to 2014) was reviewed for subjects > 12 y of age with a history of foreign body aspiration managed with flexible bronchoscopy. Demographic, clinical, and bronchoscopy data were collected and analyzed. PubMed was reviewed for studies describing the use of flexible bronchoscopy for foreign body extraction in adults.
RESULTS: During the study period, a total of 25,998 flexible bronchoscopies were performed. Of these, 65 subjects (mean age of 32.8 y, 49 males) were identified who had undergone bronchoscopy for foreign body aspiration. Nonresolving pneumonia (30.6%), direct foreign body visualization (24.6%), and segmental collapse (18.4%) were the most common radiological abnormalities. Foreign bodies were identified in 49 cases during bronchoscopy and successfully removed in 45 (91.8%) subjects with no major complications. Metallic (41%) and organic (25.6%) foreign bodies were the most common. Shark-tooth (44.9%) and alligator (32.6%) were the most commonly used forceps in retrieving the foreign bodies. The systematic review yielded 18 studies (1,554 subjects with foreign body inhalation). In adults, the proportion of flexible bronchoscopy (6 studies, 354/159,074 procedures) performed for the indication of foreign bodies among the total flexible bronchoscopies was 0.24% (95% CI 0.18–0.31). The overall success of flexible bronchoscopy (18 studies, 1,185 subjects) for foreign body extraction was 89.6% (95% CI 86.1–93.2).
CONCLUSIONS: Foreign body aspiration is a rare indication for flexible bronchoscopy in adults. Flexible bronchoscopy has a high success rate in removal of inhaled foreign body and can be considered the preferred initial procedure for management of airway foreign bodies in adults.
- foreign body aspiration
- foreign body inhalation
- tracheobronchial foreign body flexible bronchoscopy
- fiberoptic bronchoscopy
Introduction
Foreign body aspiration is an uncommon clinical entity in adults.1 Children account for the vast majority of all foreign body aspirations reported.2 Foreign bodies can either be organic (eg, peanuts, peas) or inorganic (eg, plastic caps, pins, screws, nails, teeth). Clinically, patients may present either with acute respiratory failure requiring urgent intervention or with recent onset of respiratory symptoms, including breathlessness, wheezing, coughing, and expectoration.1,3,4 Identification of foreign body aspiration requires a high index of clinical suspicion, especially in those presenting without a history of aspiration. Occasionally, a forgotten foreign body may be detected on a chest radiograph obtained for unrelated reasons or during bronchoscopy.
The radiological manifestations of foreign body aspiration include either direct visualization of the foreign body in the case of radiopaque foreign bodies or indirect signs (representing airway obstruction) in the form of nonresolving pneumonia, atelectasis, unilateral hyperinflation, or localized bronchiectasis, especially in those with organic foreign bodies.4,5 During bronchoscopy, a foreign body can be directly visualized, or granulation tissue, endobronchial stenosis, or edema, all features of tissue reaction to an aspirated foreign body, may be present.3,6 In children, rigid bronchoscopy is the procedure of choice for foreign body removal due to its ability to secure the airway, whereas in adults, flexible bronchoscopy can be used for both confirming the diagnosis and removing the foreign body.7–9 Furthermore, in children, foreign bodies lodge in the proximal tracheobronchial tree, which can be easily accessed using a rigid bronchoscope, but in adults, foreign bodies lodge in the distal tracheobronchial tree.3,10–12
Most published literature on foreign body aspiration in adults is in the form of case reports, with only few case series available.4,13,14 Here, we report our more than 35-y experience with flexible bronchoscopy for foreign body removal in adults at a tertiary care center. A systematic review of the literature on foreign body extraction by flexible bronchoscopy in the adult population was also conducted.
QUICK LOOK
Current knowledge
Foreign body aspiration is an uncommon clinical finding in adults. Children account for the vast majority of all foreign body aspirations reported. Rigid bronchoscopy is the standard practice in pediatric patients. Both rigid and flexible bronchoscopies for removal of foreign bodies in adults have been reported.
What this paper contributes to our knowledge
Foreign body aspiration was a rare indication for flexible fiberoptic bronchoscopy in adults. Flexible bronchoscopy had a high success rate in removal of inhaled foreign bodies and can be considered the preferred initial procedure for diagnosis and removal of airway foreign bodies in adults.
Methods
This was a retrospective analysis of all flexible bronchoscopies performed between September 1979 and April 2014 at the Postgraduate Institute of Medical Education and Research in Chandigarh, India. The study protocol was approved by the ethics review committee. Written informed consent was obtained from all subjects who participated in this study. The bronchoscopy database (Department of Pulmonary Medicine, Postgraduate Institute of Medical Education and Research) was searched for foreign body removal as an indication for bronchoscopy in the adult population (> 12 y of age). The following details were extracted for each subject: demographic profile, presenting symptoms, radiology, bronchoscopic findings, and type, nature, and location of the foreign body. The type of foreign body was categorized as organic, metallic, tooth, plastic, or tablet. Management (out- or in-patient), type of forceps used for foreign body extraction, procedure outcome (success or failure), and complications encountered during the procedure were also recorded.
Flexible bronchoscopy (BF-P20, BF-1T20, BF-1T150, or BF-XT40 bronchoscope with outer diameters ranging from 4.9 to 6.2 mm, Olympus, Tokyo, Japan) was performed in the bronchoscopy suite or occasionally at the bedside in subjects admitted to the hospital. Bedside bronchoscopy was performed in subjects who were ventilated and had aspirated a foreign body. The procedure was performed by either a consultant or a fellow under the direct supervision of a consultant. Flexible bronchoscopy was performed through the oral route in supine subjects suspected to have aspirated a foreign body. All subjects received nebulized lidocaine (4% solution) immediately before the procedure. Topical 10% lidocaine spray was used just before the procedure augmented by as needed instillation of 2% lidocaine over the vocal cords and during the bronchoscopy. No sedation was used during or before the bronchoscopy. Vital signs (pulse rate, breathing frequency, blood pressure, SpO2) were monitored during the procedure. The subjects were discharged the same day, after 2–3 h of observation.
A systematic examination of the airways was conducted, and once the foreign body was located, it was secured with suitable forceps, which were then withdrawn up to the tip of the bronchoscope. Once a firm grip was ensured, the entire assembly (forceps with the clasped foreign body and the flexible bronchoscope) was removed as a single unit. In the case of sharp objects, the foreign body was held with the pointed edge facing the forceps to avoid injury to the airway mucosa or vocal cords.
Systematic Review
PubMed was searched for studies written in English with subjects > 12 y of age using the terms foreign body aspiration OR foreign body inhalation OR lung foreign body OR endobronchial foreign body OR airway foreign body OR tracheo-bronchial foreign body. In addition, we reviewed our personal files. Reviews, case reports, studies with < 10 subjects, and data presented only as an abstract were excluded.
Initial Review of Studies.
The database thus created from the electronic searches was incorporated in the reference manager package Endnote X7 (Thomson-Reuters, New York, New York), and all duplicate citations were discarded. Two authors (ISS and RA) screened these citations by review of titles and abstracts to identify relevant studies. Any disagreement was resolved by discussion between the authors. The database was then scrutinized again to include only those studies describing at least 10 subjects with aspirated foreign bodies managed with flexible bronchoscopy. The full text of each of these studies was retrieved and reviewed in detail. The following items were recorded on a data extraction form: (1) publication details (authors, year, and other citation details), (2) type of study (prospective or retrospective), (3) number of subjects, (4) type of forceps used, (5) nature and location of the foreign body extracted, (6) success rate of foreign body removal by flexible bronchoscopy, and (7) complications associated with the procedure.
Meta-Analysis.
The statistical software package StatsDirect 2.7.8 (StatsDirect, Cheshire, United Kingdom) and Open MetaAnalyst 5.26.1415 was used to perform the statistical analysis. A meta-analysis was performed for (1) the prevalence of flexible bronchoscopy performed for the indication of foreign bodies in adults among the total flexible bronchoscopies and (2) the success of flexible bronchoscopy in foreign body extraction. The proportion (Freeman-Tukey variant of the arcsine square-root transformed proportion) with 95% CI was calculated for each study, and the data were pooled using a random-effects model to derive a pooled proportion with 95% CI.16–18 Heterogeneity was assessed using the I2 test, with a value of > 50% indicating significant heterogeneity.19 Publication bias was assessed using a funnel plot20 and 3 statistical methods (Egger test,21 Harbord test,22 and Begg-Mazumdar test23).
Results
A total of 25,998 flexible bronchoscopies were performed during the study period. Sixty-five (0.25%) subjects underwent flexible bronchoscopy for clinical suspicion of foreign body inhalation. The mean ± SD age of these 65 subjects was 32.8 ± 17.9 y; 49 (75.3%) were males. Of these, 60 subjects recalled inhaling a foreign body, and 5 subjects had abnormal chest radiographs with a foreign body detected during bronchoscopic assessment. The time to presentation was < 7 d in 16 subjects, and the remaining subjects presented > 7 d after aspiration. Bedside flexible bronchoscopy was performed in one subject to remove a foreign body. The subject had sustained a head injury and aspirated a tooth during intubation (aspiration pneumonia). A flexible bronchoscope was introduced through the endotracheal tube, and the tooth was identified in the right intermediate bronchus. Shark-tooth forceps were used, and the forceps, tooth, and flexible bronchoscope were removed together as a single unit. Radiological (chest radiograph or chest computed tomography) abnormalities were seen in the majority of subjects (56/65, 86.2%) at presentation, including mainly nonresolving opacities, segmental atelectasis/lobar collapse, bronchiectasis, or hyperinflation (Table 1). Chest radiograph was diagnostic in 16 (24.6%) of these 65 subjects (pins [n = 4], teeth [n = 5], pen caps [n = 3], buttons [n = 1], nails [n = 1], and screws [n = 2]), whereas it was normal in 9 subjects.
Demographic Profile, Radiology, Location, and Type of Foreign Body Encountered During Bronchoscopy Performed in Subjects With a History of Foreign Body Inhalation
During bronchoscopy, a foreign body was encountered in 49 (75.3%) subjects. Information regarding the type of foreign body was available for 39 subjects, whereas this information was not recorded for 10 subjects. In 16 (25%) subjects, no foreign body could be identified (these subjects were excluded from the analysis, and their data were used only to calculate foreign body aspiration as an indication for performing flexible bronchoscopy). Metallic foreign bodies were the most common type, followed by organic ones. The metallic foreign bodies encountered were: pins (n = 7), whistles (n = 5), screws (n = 2), springs (n = 1), and nails (n = 1). The organic foreign bodies included: betel nuts (n = 2), peanuts (n = 1), peas (n = 1), cotton swabs (n = 1), lentil seeds (n = 2), rice (n = 1), garlic bulbs (n = 1), and cinnamon sticks (n = 1). Plastic objects were found in 4 subjects (pen caps [n = 3] and buttons [n = 1]), and teeth were found in 8 subjects. One subject had aspirated a tablet, which was associated with surrounding edema and hyperemia. The foreign body was removed in 45 (91.8%) subjects during flexible bronchoscopy. In 41 subjects, the foreign body was removed in the first attempt, whereas in 4 subjects, it was partially removed, and a repeat procedure was required. Of the remaining 4 subjects, the foreign body was successfully removed by rigid bronchoscopy in 2 subjects, and 2 subjects were lost to follow-up. Granulation tissue was present in 11 subjects, mucosal edema in 8 subjects, and bronchial stenosis in 3 subjects. The subjects with granulation tissue and mucosal edema responded favorably to oral corticosteroids (0.5 mg/kg prednisolone tapered over 3 weeks), whereas the subjects with bronchial stenosis were managed with repeated balloon dilatation. Two of the 3 subjects who underwent balloon dilatation had minimal residual stenosis (15–20% occlusion) on follow-up bronchoscopy, whereas one subject had persistent stenosis (80%) of the right middle-lobe bronchus. On follow-up, only one subject had a radiological abnormality (persistent right middle-lobe collapse). Most subjects (n = 58, 89.2%) were managed in an out-patient setting and were discharged the same day.
The right lower-lobe bronchus (n = 15, 30.6%) was the most common location of foreign bodies (see Table 1). One subject had bilateral foreign bodies (metallic screws): one each in the right intermediate and left main bronchi (Fig. 1). The most common forceps used to extract foreign bodies were the shark-tooth forceps (n = 22, 44.9%), followed by the alligator forceps (n = 16, 32.6%). A Dormia basket and magnetic forceps were used in one subject each for foreign body retrieval. Complications were encountered in 4 (6.1%) subjects, including mucosal abrasion in one subject. In 3 subjects, the foreign body was extracted from the airway but slipped into the digestive tract. All 4 subjects were managed conservatively, and none required further intervention.

Chest radiograph showing 2 foreign bodies (metal screws): one in the right intermediate bronchus and one in the left main bronchus.
Systematic Review
A total of 1,314 studies were found on literature search, of which 18 studies (1,554 adult subjects with tracheobronchial foreign bodies) were included (Fig. 2).3,4,6,10–12,14,24–34 These studies were reported in developed and developing countries (Table 2). There was a slight male preponderance (16 studies: 536 males, 443 females). The right bronchial tree was the most common reported location of the foreign body. A wide range of foreign bodies were encountered, with the exact type depending on the geographic location.

Flow chart for studies included in systematic review.
Studies Using Flexible Bronchoscopy for Foreign Body Extraction
Six studies reported the proportion of bronchoscopies performed for the indication of foreign body removal among the total number of bronchoscopies performed. The proportion ranged from 0.16 to 0.33%, with a pooled proportion of 0.24% (95% CI 0.18–0.31) (Fig. 3).11,26,31–33,35 A total of 1,185 subjects (including the current study) underwent flexible bronchoscopy for extraction of foreign bodies. The success rate of flexible bronchoscopy for foreign body extraction ranged from 61 to 100%, with a pooled success rate of 89.6% (95% CI 86.1–93.2) (Fig. 4). In the remaining subjects, the foreign bodies were successfully retrieved by rigid bronchoscopy (n = 39, 3.3%) or thoracotomy (n = 26, 2.2%). Four (0.3%) subjects refused further treatment, and 5 subjects coughed out the foreign body after the procedure. Three subjects were lost to follow-up, and 2 subjects recovered without further treatment. The complications encountered during flexible bronchoscopy included bleeding (n = 18), hypoxia (n = 2), migration into another bronchial segment (n = 4), slippage into the gastrointestinal tract (n = 5), transient hypotension, and low-grade fever (see Table 2). There was clinical heterogeneity reflected by the varying age of subjects and the different geographic locales and types of foreign bodies.

Prevalence of foreign bodies during flexible bronchoscopy performed in adults (random-effects model). The prevalence in the individual studies is represented by a square (percent) through which runs a horizontal line (95% CI). The diamond at the bottom represents the pooled prevalence from the studies.

Success of flexible bronchoscopy in foreign body extraction in adults (random-effects model). The prevalence in the individual studies is represented by a square (percent) through which runs a horizontal line (95% CI). The diamond at the bottom represents the pooled prevalence from the studies.
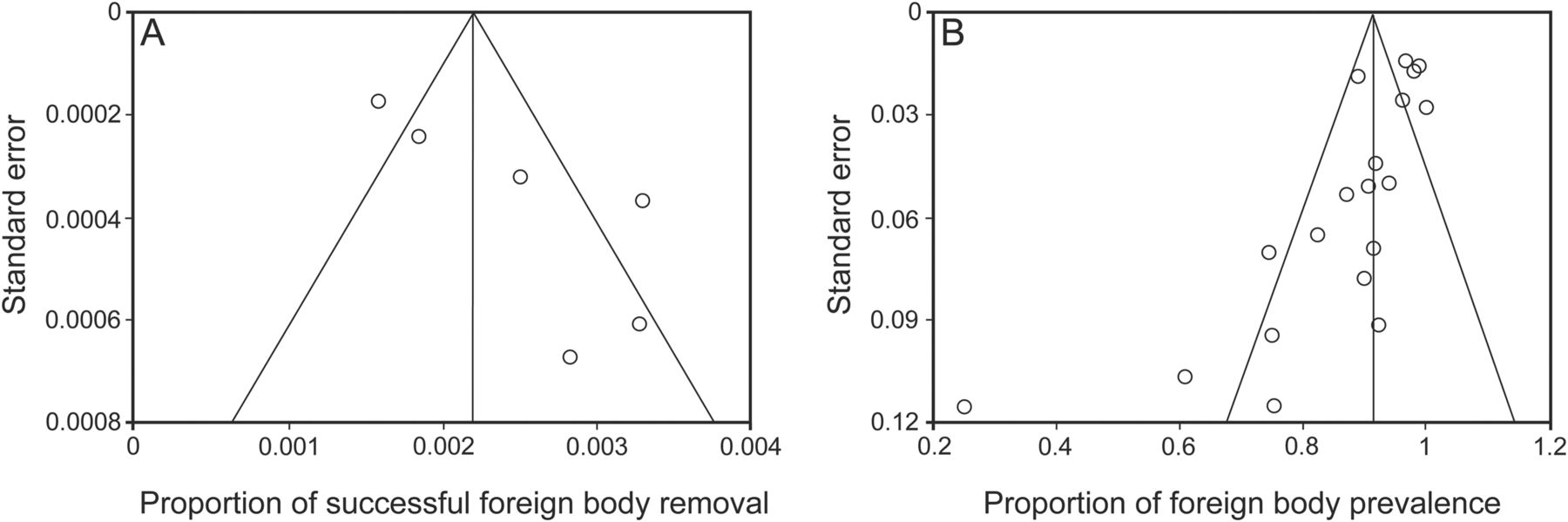
There was significant heterogeneity in both the outcomes (I2 > 80%) and evidence of publication bias in the funnel plot (Fig. 5). There was also evidence of publication bias in all statistical tests (Begg-Mazumdar: Kendall's tau = −0.532, P = .008; Egger: bias = −2.625, P = .009; Harbord: bias = −3.163, P = .046).

Funnel plots comparing proportion vs standard error of proportion for the outcomes of success (A) and prevalence of foreign bodies (B) during flexible bronchoscopy. Circles represent trials included in the meta-analysis. The lines in the center indicate the summary proportion. Angled lines represent 95% CI. There was evidence of publication bias.
Discussion
The results of this study and systematic review suggest that foreign body inhalation is a rare occurrence in adults. Also, flexible bronchoscopy is a safe and effective means of retrieving airway foreign bodies in the adult population. In this study spanning > 3 decades, only 1 in 400 bronchoscopies were performed for foreign body removal (similar to the proportion in the systematic review). The success rate of flexible bronchoscopy in the extraction of foreign bodies was 92% in this study, similar to that in the systematic review (89.6%).
Rigid bronchoscopy is required in a large number of cases of foreign body removal in children.12 However, in adults, flexible bronchoscopy avoids the need for rigid bronchoscopy in most cases (∼90% according to the systematic review). Flexible bronchoscopy also has several advantages over rigid bronchoscopy: it can be performed on an out-patient basis, is more cost-effective and widely available, and avoids the need for anesthesia and sedation. Furthermore, the use of flexible bronchoscopy was associated with lower mortality and morbidity compared with rigid bronchoscopy (1% vs 12%) in a study comprising 300 subjects, possibly due to the avoidance of general anesthesia.24 In the present study, flexible bronchoscopy was associated with minimal complications (4 subjects), whereas in the systematic review, the complications included minor bleeding, hypoxemia, slippage of the foreign body into the gastrointestinal tract, and migration of the foreign body into another bronchial segment.3,6,10,28,30,35–37 However, there are situations in which flexible bronchoscopy is unsuccessful in foreign body extraction, including foreign bodies that are impacted in extensive granulation tissue or excessive tissue scarring, a large foreign body that cannot be gripped with flexible forceps, asphyxiating foreign bodies, foreign bodies with a smooth margin, sharp foreign bodies, and several failed attempts by flexible bronchoscopy to retrieve a foreign body.38 In these cases, rigid bronchoscopy remains the procedure of choice (Table 3).3,4,6,10,14,22,23,25,35
Studies Reporting Details of Flexible Bronchoscopy Failure in Removing Foreign Bodies
A variety of instruments are used during flexible bronchoscopy to extract a foreign body, such as grasping forceps or Dormia basket, depending on the nature of the foreign body. Grasping or tooth forceps (alligator, shark-tooth, and rat-tooth) should be used to remove flat or thin inorganic or hard organic foreign bodies, with the choice depending on the shape of the foreign body.1 A fish net or Dormia basket is used to extract soft foreign bodies because grasping forceps can cause fragmentation. Shark-tooth and alligator forceps were used most often in this study because metallic or firm foreign bodies were the most common. In one subject, magnetic forceps and fluoroscopy were employed to fish out a metallic foreign body (sewing pin) lodged in a distal segment not visible on bronchoscopy. Once it was extracted up to the main bronchus, it was removed with alligator forceps.
The diagnosis of foreign body aspiration is difficult to establish in adult subjects who present without a history of aspiration.1,3 Most subjects with a history of foreign body aspiration present late to a medical facility (only 25% of subjects presented within 7 d of aspiration in this study). This is due to the innocuous nature of symptoms that foreign bodies incite in the adult population and the spontaneous resolution of symptoms that occurs due to lodging of the foreign body in the more peripheral airways.14,34 In contrast, foreign bodies in children are commonly found in the proximal airways and produce more drastic symptoms, including respiratory failure in several cases, requiring an early intervention.3,10–12
Many adult subjects with tracheobronchial foreign bodies described in previous studies had an underlying risk factor, such as neuromuscular disease, head trauma, alcohol intoxication, or altered sensorium.4,24,32,35 In contrast, all subjects (except one with a head injury) in the present study were healthy and did not have any specific risk factors for foreign body aspiration. Apart from the traditional risk factors, eating habits, local customs, and occupations not only predispose people to foreign body aspiration but also dictate the type of foreign bodies encountered in a particular population. In a study from Croatia, animal bone and cherry stone aspiration was common due to dietary habits.32 In a healthy Chinese population, foreign body aspiration was attributed to eating with chopsticks, which increases the risk of foreign body inhalation.10 In several studies from the Middle East, turban pins were the most common type of foreign body aspirated, as they are held between the teeth while tying the traditional turban.27,28,39,40
The most common location for a foreign body in the airway is the right bronchial tree, particularly the right lower-lobe and intermediate bronchi, due to the vertical orientation of the right main bronchus.1,2,4,14 Bilateral foreign bodies were present in only one subject and are rare.2,32,41,42 The foreign bodies could not be identified in 25% of the subjects possibly due to spontaneous expulsion of the foreign body, dissolution of an organic foreign body, or embedding of a small foreign body in granulation tissue or edematous mucosa.43
At the authors' center, the first step in the management of adult foreign body aspiration is flexible bronchoscopy, which, in most cases, is both diagnostic and therapeutic. In patients for whom flexible bronchoscopy is unsuccessful, rigid bronchoscopy is performed (Fig. 6). In those with granulation tissue after extraction of the foreign body, a short course of glucocorticoids (0.5 mg/kg prednisolone tapered over 21 d) is administered. If unsuccessful, patients are then managed with cryotherapy or argon plasma coagulation; balloon bronchoplasty is used in the management of bronchostenosis.

Algorithm for management of adult airway foreign bodies used at the authors' center.
This study has several limitations. As the study was retrospective, comprehensive information on procedure duration and other details are not available. There were significant heterogeneity and publication bias in the meta-analysis, possibly due to the difference in subject profiles and operator experience.
Conclusions
In summary, foreign body inhalation is an uncommon clinical entity in adults and requires a high index of clinical suspicion for diagnosis, especially in those without a history of foreign body aspiration. In adults, flexible bronchoscopy is safe and has a high success rate for identification and removal of foreign bodies.
Footnotes
- Correspondence: Ritesh Agarwal MD DM, Department of Pulmonary Medicine, Postgraduate Institute of Medical Education and Research, Chandigarh 160012, India. E-mail: agarwal.ritesh{at}outlook.in.
The authors have disclosed no conflicts of interest.
- Copyright © 2015 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}