

Abstract
BACKGROUND: Corticosteroids have been used for refractory Mycoplasma pneumoniae pneumonia and have beneficial effects. The aim of this study was to identify the biomarkers for predicting refractory M. pneumoniae pneumonia in a timely fashion to initiate steroid therapy.
METHODS: This was a prospective cohort study of children with M. pneumoniae pneumonia admitted to the Children's Hospital of Fudan University from September 2012 to August 2013. Lactate dehydrogenase (LDH) and other laboratory tests, including complete blood counts, C-reactive protein, erythrocyte sedimentation rate (ESR), alanine aminotransferase, aspartate aminotransferase, α-hydroxybutyrate dehydrogenase (HBDH), creatine kinase, and creatine kinase MB, were performed on admission. Based on the definition of refractory M. pneumoniae pneumonia, subjects were divided into 2 groups: refractory M. pneumoniae pneumonia and usual M. pneumoniae pneumonia. The diagnostic values of laboratory findings were analyzed.
RESULTS: In total, 653 subjects were enrolled, including 300 in the refractory pneumonia group and 353 in the usual pneumonia group. There was no significant difference in sex distribution between the 2 groups. The average age in the refractory M. pneumoniae pneumonia group was greater than that in the usual M. pneumoniae pneumonia group. Compared with the usual pneumonia group, the refractory pneumonia group showed significantly higher levels of C-reactive protein, serum LDH, serum HBDH, serum alanine aminotransferase, serum aspartate aminotransferase, and neutrophils and higher ESRs. Logistic regression showed that age, LDH, and ESR were the significant factors in predicting refractory M. pneumoniae pneumonia. In addition, LDH and HBDH were strongly correlated, and receiver operating characteristic curve analysis showed that the area under the curve of LDH was 0.718 with a cutoff of 379 IU/L, that of ESR was 0.683 with a cutoff of 32.5 IU/L, and that of HBDH was 0.691 with a cutoff of 259.5 IU/L.
CONCLUSIONS: Serum LDH can be used as a biomarker to predict refractory M. pneumoniae pneumonia at the early stage of hospitalization.
- Refractory Mycoplasma pneumoniae pneumonia
- lactate dehydrogenase
- α-hydroxybutyrate dehydrogenase
- erythrocyte sedimentation rate
- receiver operating curve
Introduction
Mycoplasma pneumoniae is one of the major causative pathogens of community-acquired respiratory tract infections in children. M. pneumoniae infections occur both endemically and in cyclic epidemics every 3–7 y and account for 10–40% of community-acquired pneumonia cases in children.1 Although pneumonia due to M. pneumoniae is usually a benign, self-limited disease, some cases become refractory or severe and life-threatening.2–4 It can also cause a wide array of extrapulmonary manifestations5–9 and even lead to sequelae and disability, such as bronchiectasis, bronchiolitis obliterans, interstitial pulmonary fibrosis, and paralysis.10,11
Clinically, corticosteroids have been used for refractory M. pneumoniae pneumonia and have a dramatic beneficial effect in both children and adults.2,4,12 Clinicians must be cognizant of children with M. pneumoniae pneumonia at risk for developing refractory or serious illnesses and initiate steroid therapy in a timely fashion. Thus, it is desirable to predict refractory illness as soon as possible.
In a previous study,4 we found that lactate dehydrogenase (LDH), C-reactive protein, and erythrocyte sedimentation rate (ESR) on admission were increased in subjects with refractory M. pneumoniae pneumonia. We hypothesized that they play important roles in this illness. Based on a review of the literature, there are a few reports on the role of LDH, C-reactive protein, and ESR in refractory M. pneumoniae pneumonia, but they are limited to case series.4,13,14 In this study, we explored whether LDH, C-reactive protein, and ESR are potential laboratory markers that could be used to predict refractory M. pneumoniae pneumonia in a large sample.
QUICK LOOK
Current knowledge
M. pneumoniae is one of the major causative pathogens of community-acquired respiratory tract infections in children. Although pneumonia due to M. pneumoniae is usually benign, some cases develop into refractory, life-threatening disease. Corticosteroids are an effective treatment for severe disease. A biomarker or method to predict patients at risk for developing refractory disease could improve the timing of corticosteroid treatment and improve patient outcomes.
What this paper contributes to our knowledge
In a group of children admitted to the hospital for M. pneumoniae pneumonia, serum lactate dehydrogenase (LDH) predicted refractory disease at hospitalization. LDH may prove useful as a biomarker for predicting refractory disease and determining which candidates may benefit from early corticosteroid therapy.
Methods
Subjects and Groups
This was a planned secondary analysis of a prospective cohort study (Fig. 1). Children with M. pneumoniae pneumonia admitted to the Children's Hospital of Fudan University from September 2012 to September 2013 were enrolled. M. pneumoniae infection was confirmed by serologic testing to detect M. pneumoniae immunoglobulin M (IgM) by enzyme-linked immunosorbent assay and/or polymerase chain reaction testing for M. pneumoniae in nasopharyngeal secretions. Subjects with immune deficiencies, chronic diseases, or heart diseases or who were using immunosuppressive drugs were excluded. All enrolled subjects had negative tuberculosis IgM or purified protein derivative tests. In addition, their nasopharyngeal secretions were negative for respiratory syncytial viruses, influenza viruses, adenovirus, parainfluenza virus, and Chlamydia trachomatis. The subjects also had negative bacterial cultures of nasopharyngeal secretions and double-negative blood cultures. Consent for participation was obtained. The study was approved by the hospital's ethics committee.

Flow chart.
Refractory M. pneumoniae pneumonia is defined as a case with prolonged fever accompanied by deterioration of radiological findings despite appropriate management with macrolide treatment for ≥ 7 d.2,15,16 On the basis of this definition, we reviewed subjects' records and divided them into 2 groups: a refractory M. pneumoniae pneumonia group and a usual M. pneumoniae pneumonia group.
Study Variables and Data Collection
The main outcome measure of the study was serum LDH on admission. We also obtained complete blood counts, ESRs, and levels of C-reactive protein, alanine aminotransferase, aspartate aminotransferase, and other enzymes, including serum α-hydroxybutyrate dehydrogenase (HBDH), creatine kinase, and creatine kinase MB. Demographic characteristics were collected from the subjects' records.
Respiratory Pathogens
Nasopharyngeal aspirates were tested for respiratory pathogens using a real-time, multiplex polymerase chain reaction assay (Diagnostic Hybrids, Athens, Ohio) in our hospital's clinical virology laboratory. The specific pathogens identified included influenza A and B, respiratory syncytial viruses, adenovirus, parainfluenza virus, C. trachomatis, and M. pneumoniae. A positive polymerase chain reaction (Shanghai Shen Yousheng Biotech, Shanghai, China) result for M. pneumoniae was a copy number of >2,500/mL. Bacterial culture results based on nasopharyngeal aspirates and blood were obtained from the hospital's microbiology laboratory. M. pneumoniae IgM was detected using a commercial enzyme-linked immunosorbent assay kit (Beijing Rongzhi Haida Biotech, Beijing, China) according to the manufacturer's instructions, and the positive result was an M. pneumoniae IgM titer of > 1:320.
Statistical Analysis
Statistical analysis was performed with SPSS 16.0 (SPSS, Chicago, Illinois) and MedCalc (MedCalc Software, Mariakerke, Belgium), and P < .05 was considered statistically significant. Categorical variables were analyzed using the chi-square test. Normally distributed measurement data were analyzed with t tests, and non-normally distributed measurement data were analyzed with Mann-Whitney U tests. Multivariate analysis was performed using a stepwise logistic regression model. Receiver operating characteristic (ROC) curves were used to analyze the power of the laboratory markers for prediction of refractory M. pneumoniae pneumonia.
Results
Demographical Characteristics
We enrolled 653 subjects. There were 300 cases (171 boys and 129 girls) in the refractory M. pneumoniae pneumonia group, and 353 cases (221 boys and 132 girls) in the usual M. pneumoniae pneumonia group. There was no significant difference in sex distribution between the 2 groups (P = .15). The average age in the refractory M. pneumoniae pneumonia group was 66.8 ± 37.5 months (range of 3–184 months, median of 66 months) and 51.4 ± 34.4 months (range of 1–156 months, median of 46 months) in the usual M. pneumoniae pneumonia group. The average age in the refractory pneumonia group was greater than that in the usual pneumonia group (P < .001).
Laboratory Findings
The laboratory findings on admission are summarized in Table 1. Compared with the usual M. pneumoniae pneumonia group, the refractory M. pneumoniae pneumonia group showed significantly higher levels of C-reactive protein (31.4 ± 39.1 vs 15.5 ± 20.5 mg/L, P < .01), neutrophils (61.9 ± 15.0% vs 51.7 ± 17.1%, P < .01), serum LDH (449 ± 258 vs 304 ± 78.1 IU/L, P < .01), serum HBDH (357 ± 233 vs 249 ± 69.3 IU/L, P < .001), serum alanine aminotransferase (23.2 ± 42.8 vs 12.4 ± 18.2 IU/L, P < .001), and serum aspartate aminotransferase (30.1 ± 28.7 vs 21.9 ± 20.7 IU/L, P < .01) and higher ESRs (40.8 ± 23.4 vs 28.2 ± 20.0 mm/h, P < .01). However, the percentage of lymphocytes in the refractory M. pneumoniae pneumonia group was lower than that in the usual M. pneumoniae pneumonia group (28.8 ± 13.5% vs 39.3 ± 16.3%, P < .01). The other laboratory findings were not significantly different between the 2 groups.
Comparison of Laboratory Findings on Admission for the Refractory and Usual M. pneumoniae Pneumonia Groups
Logistic Regression
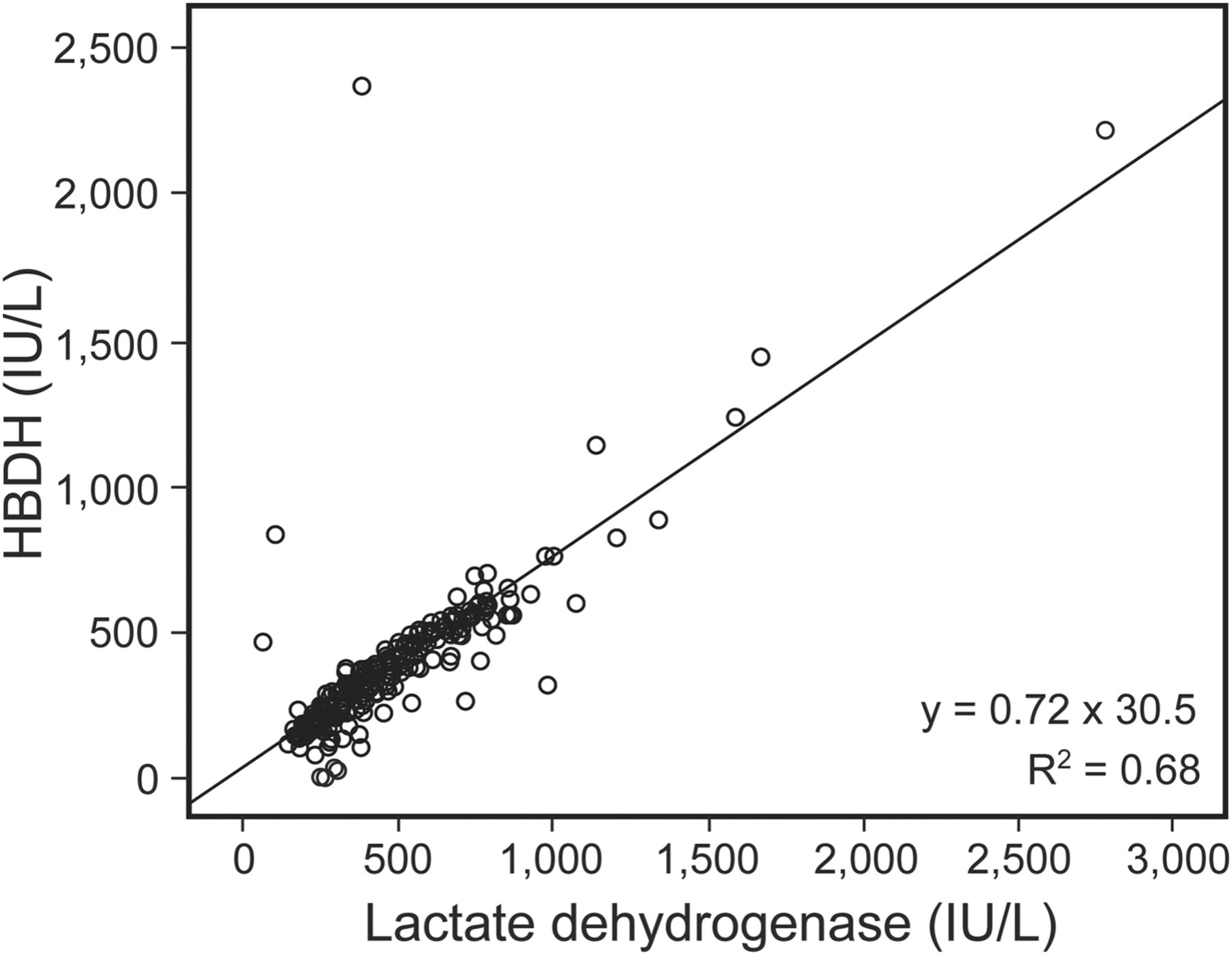
Age, LDH, HBDH, alanine aminotransferase, aspartate aminotransferase, neutrophils, lymphocytes, C-reactive protein, and ESR were analyzed in a stepwise logistic regression model. The results showed that serum LDH (odds ratio of 1.01, 95% CI 1.00–1.01, P < .001) and ESR (odds ratio of 1.02, 95% CI 1.00–1.03, P < .001) on admission were significant risk factors for refractory M. pneumoniae pneumonia (Table 2). In all covariates, we found that LDH and HBDH had a positive correlation, and the Pearson correlation was 0.822 (P = .01) (Fig. 2).
Logistic Regression Analysis of Associated Factors in Refractory M. pneumoniae Pneumonia
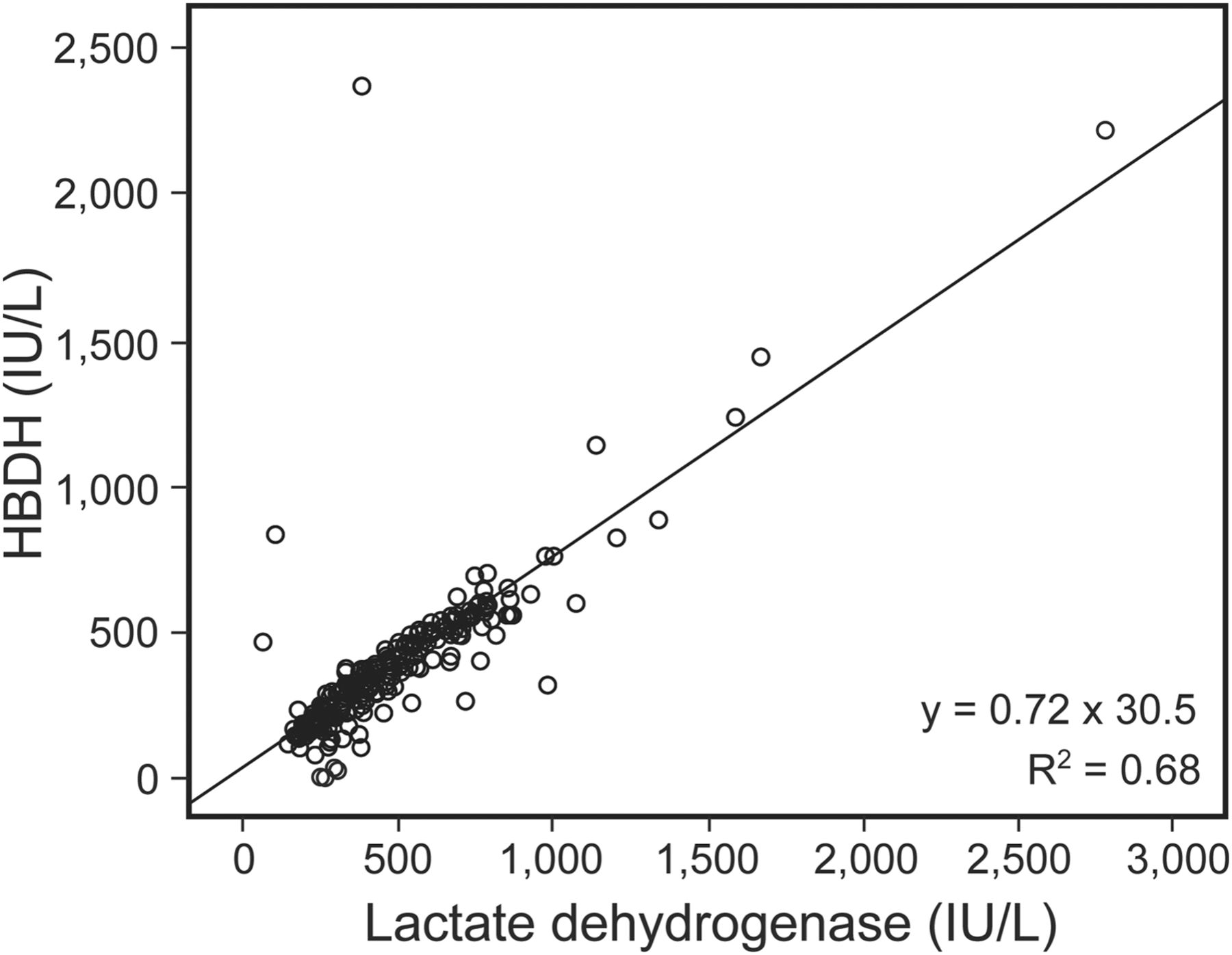
Correlation between lactate dehydrogenase and α-hydroxybutyrate dehydrogenase (HBDH).
ROC Curve Analysis
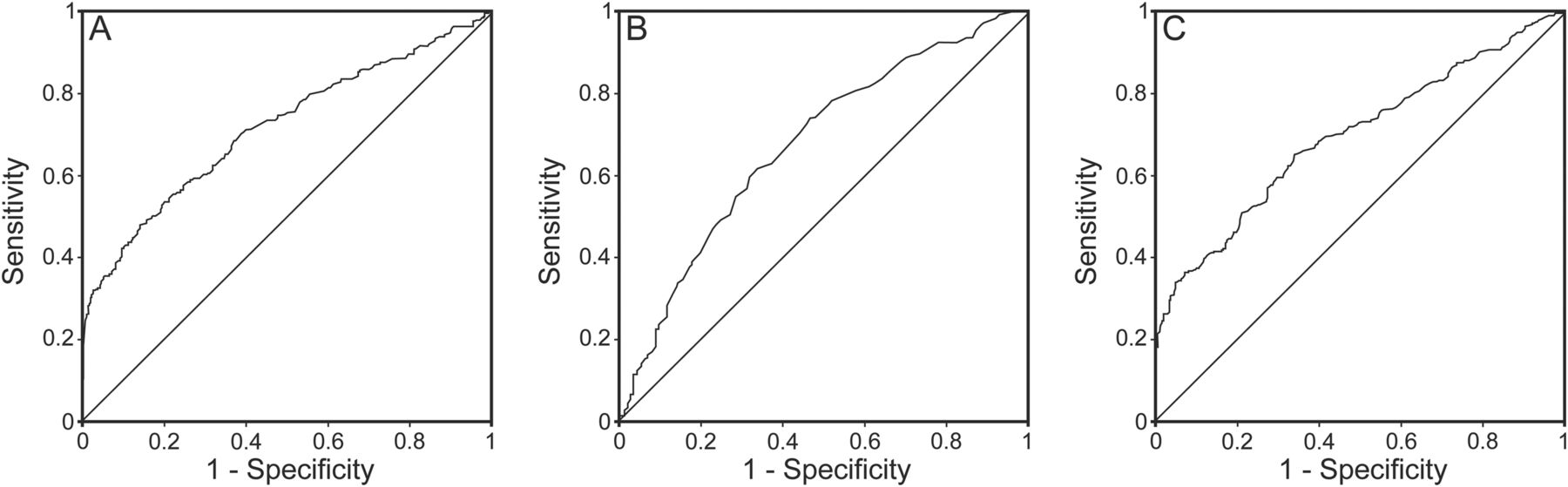
The area under the curve for LDH was 0.718 (95% CI 0.678–0.758) as determined by ROC curve analysis (Fig. 3). The optimal cutoff of LDH for predicting refractory M. pneumoniae pneumonia was 379 IU/L, with a sensitivity of 48%, specificity of 85.8%, positive predictive value of 74.2%, and negative predictive value of 65.9% (Table 3). The area under the curve for ESR was 0.683 (95% CI 0.626–0.740), and that for HBDH was 0.691 (95% CI 0.650–0.733) (Fig. 3 and Table 3).
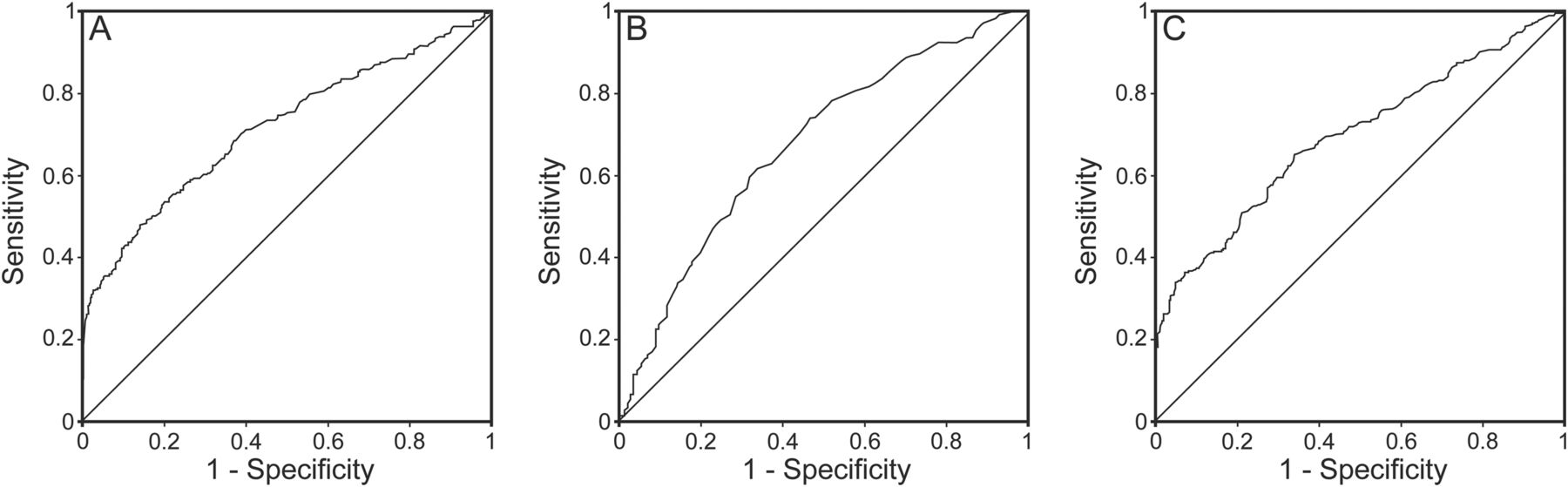
Receiver operator characteristic curves for predicting refractory M. pneumoniae pneumonia. A: Lactate dehydrogenase. B: Erythrocyte sedimentation rate. C: α-Hydroxybutyrate dehydrogenase.
Predictive Value of LDH, ESR, and HBDH
Discussion
The incidence of refractory M. pneumoniae pneumonia has recently increased,4,16,17 and it is associated with macrolide-resistant strains.18–21 Cell-mediated immunity of the host rather than direct microbial damage plays an important role in the progression of this illness.22,23 Clinically and experimentally, steroids have a positive effect on refractory M. pneumoniae pneumonia.2,4,16,24 However, steroids are usually initiated after the condition deteriorates. Thus, those with unrecoverable damage due to refractory M. pneumoniae pneumonia cannot rehabilitate completely.25–28 Although there is no case-control study on the benefit of steroids in refractory M. pneumoniae pneumonia, it is believed that early steroid therapy might prevent disease progression and reduce disease morbidity without adverse reactions.29,30 However, it is impossible to initiate steroids early for all M. pneumoniae infections because most of them are self-limited, and there is no evidence to support the use of systemic steroids in community-acquired pneumonia due to other pathogens.31 In addition, an epidemiological investigation showed that there is no apparent risk factor for refractory M. pneumoniae pneumonia32; therefore, predicting this illness at an early stage may improve the prognosis of M. pneumoniae infection, as this might help identify subjects for trials of early steroid administration.
Logistic regression showed that serum LDH and ESR were the main risk factors for refractory M. pneumoniae pneumonia after age difference was adjusted. Studies showed that LDH was associated with many pulmonary diseases, such as obstructive diseases, microbial pulmonary diseases, and interstitial lung diseases.33,34 Several studies2,4,13 also found that serum LDH was elevated in refractory M. pneumoniae pneumonia; however, there was no evidence showing that this elevation was associated with host immune response or virulence of M. pneumoniae. In this study, we found that the area under the curve for LDH was 0.718 in ROC curve analysis, indicating fair discriminative power for predicting refractory M. pneumoniae pneumonia. The optimal cutoff for LDH was 379 IU/L, with a sensitivity of 48% and specificity of 85.8%. This indicates its clinical utility in identifying patients at high risk for refractory M. pneumoniae pneumonia: namely, patients with usual M. pneumoniae pneumonia will not be misdiagnosed with refractory pneumonia and started on steroid therapy. Another study showed that children with M. pneumoniae infection who were possible candidates for steroid therapy usually had significantly elevated levels of LDH (> 480 IU/L).35 Inamura et al13 performed ROC curve analysis and showed that the cutoff of LDH for refractory M. pneumoniae pneumonia was 410 IU/L. The cutoffs were greater than in our study. The main reason may be that their results were obtained from a small case series, and they had more serious illnesses. In this study, at the cutoff point, the positive predictive value of LDH was 74.2%. As positive predictive value is also sensitive to disease prevalence, which may be different in different clinical settings, the LDH test may have a lower positive predictive value in populations with a lower prevalence of refractory M. pneumoniae pneumonia.
The serum HBDH test measures mainly the LDH-1 and LDH-2 isoforms, reflecting serum LDH activity.36 Few reports are available on the serum activity of HBDH in pulmonary disease. In this study, we found that HBDH was associated with refractory M. pneumoniae pneumonia and could be used as a potential predictive marker for this illness. However, ROC curve analysis in this study showed that it was not an ideal biomarker for predicting refractory M. pneumoniae pneumonia. In addition, we found that HBDH was positively correlated with LDH in M. pneumoniae infections, which may be the reason why HBDH was not a risk factor in the logistic regression analysis. To our knowledge, this is the first report on the association between HBDH and refractory M. pneumoniae pneumonia.
There are limitations to our study. First, we divided our subjects into 2 groups based on the definition of refractory M. pneumoniae pneumonia,2,16 and this definition was broad. Therefore, spectrum bias was introduced into our results. Moreover, this bias may be the main reason why the ROC curve analysis of LDH showed just a fair discriminative power for refractory M. pneumoniae pneumonia. However, the children in the refractory pneumonia group remained at the highest risk for severe or refractory illness. Thus, our findings could still be applied to a very common clinical scenario for screening those refractory cases.
Conclusions
In summary, serum LDH can be used as a biomarker for predicting refractory M. pneumoniae pneumonia and determining candidates who may benefit from corticosteroid therapy during the early stages of hospitalization. Furthermore, more research is needed to identify the potential utility of early steroid administration, which could be performed based on the use of LDH as a biomarker to initiate steroid treatment.
Acknowledgments
We gratefully acknowledge the statistical help given by Mr Peng Shi (Department of Information Management, Children's Hospital of Fudan University, and Center of Evidence-based Medicine, Fudan University, Shanghai, China). We also acknowledge LetPub (www.letpub.com) for linguistic assistance during the preparation of this manuscript.
Footnotes
- Correspondence: Libo Wang MD and Liling Qian MD PhD, Children's Hospital of Fudan University, 399 Wan Yuan Road, Shanghai 201102, China. E-mail: wanglbc{at}163.com and llqian{at}126.com.
This study was supported by the Program for New Century Excellent Talents in University (NCET-12-0126). The authors have disclosed no conflicts of interest.
- Copyright © 2015 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}