

Abstract
This systematic review examines levels of evidence and recommendation grades of various therapeutic interventions of inspiratory muscle training in people who have had a stroke. Benefits from different levels of force and resistance in respiratory muscles are shown in this population. This review was conducted following the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) directives and was completed in November 2014. The search limits were studies published in English between 2004 and 2014. Relevant studies were searched for in MEDLINE, PEDro, OAIster, Scopus, PsycINFO, Web of Knowledge, CINAHL, SPORTDiscus, DOAJ, Cochrane, Embase, Academic Search Complete, Fuente Académica, and MedicLatina. Initially, 20 articles were identified. After analyzing all primary documents, 14 studies were excluded. Only 6 studies were relevant to this review. Three different types of interventions were found (maximum inspiratory training, controlled training, and nonintervention) in 3 different groups. One specific study compared 3 inspiratory muscle training groups with a group of breathing exercises (diaphragmatic exercises with pursed lips) and a control group. Future long-term studies with larger sample sizes are needed. It is necessary to apply respiratory muscle training as a service of the national health system and to consider its inclusion in the conventional neurological program.
Introduction
People who have had a cerebrovascular accident have a greater risk of associated pneumonias, which involve increased morbidity and mortality and a high consumption of drugs.1,2 Cerebrovascular diseases or stroke is the third most frequent cause of death in developed countries, only after heart disease and cancer.3 It has been observed that subjects who have had a cerebrovascular accident have weak respiratory muscles.4 Patients after stroke show a restrictive pattern, with significant reduction in the maximum voluntary ventilation and maximum respiratory pressures coupled with an altered dynamic costal and diaphragmatic movement. Currently, nonpharmacologic treatment and therapeutic exercise training are necessary to prevent stroke-associated pneumonia to improve the effectiveness of a cough.5
Three-quarters of strokes affect patients over 65 y of age because of the aging population in the area.3 Strokes are also the most significant permanent disability in Europe; therefore, strokes create a cumbersome economic load for families and the community.
There is evidence of the benefits of peripheral muscle training in subjects after stroke.6 However, there is little literature on respiratory muscle training in this population. Only a systematic review on respiratory muscle training in neurological subjects exists.7 No large-scale studies have been conducted using threshold pressure devices during breathing exercises in subjects after stroke. Several studies showed consistent results according to the use of inspiratory exercises with threshold devices to improve the strength of respiratory muscles; however, these studies had small sample sizes.8,9
A 4-week study combined inspiratory exercises and expiration with pursed lips, which significantly improved Tiffeneau index (FEV1/VC), total volume, and inspiratory capacity.10 Undoubtedly, subjects seated with the spine at 90° had better mobility in the thoracic cage, which significantly favored better maximum inspiration with respect to the supine position.11 Furthermore, it was observed that the therapeutic inspiratory muscle training intervention had functional effects on the recovery of subjects after stroke.4 There are studies that support inspiratory muscle training interventions5,8–10,12; however, more studies are needed to determine whether patients who have had a cerebrovascular accident can improve respiratory muscle strength and endurance to improve their quality of life.
The main aim of this review was to detect the level of evidence and grade of recommendation according to the inspiratory muscle training interventions of subjects after stroke. Therefore, it is necessary to develop the most appropriate protocol to improve respiratory muscle weakness and pulmonary function according to the aims of the respiratory therapist and physiotherapists.
Methods
Database Search
This review was performed following the guidelines of PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses; www.prisma-statement.org/statement.htm, Accessed July 28, 2015),13 The initial search was carried out in January and February 2014 and was completed with a new search to update the review in November 2014. The literature searches were performed to identify all possible studies that could help answer the research question. MEDLINE, PEDro, OAIster, Scopus, PsycINFO, Web of Knowledge, CINAHL, SPORTDiscus, DOAJ, Cochrane, Embase, Academic Search Complete, Fuente Académica, and MedicLatina were searched. In addition, the search was performed in a relevant bibliographic database. Twenty articles were identified in this systematic review. All reference lists of the revised articles were reviewed. Abstracts published in conferences and congresses were also considered.
Two reviewers performed several searches in the databases. The following combinations of key words were used: stroke, cerebrovascular accident, threshold valve, respiratory muscle training, respiratory exercises, and threshold training of inspiratory muscles. The limits of searches were studies published in English between 2004 and 2014.
Inclusion and Exclusion Criteria
Inclusion criteria were considered using the PICO (population, intervention, control/comparison, and outcome variables) model. First, subjects who were included had experienced a moderate or severe stroke according to the National Institutes of Health Stroke Scale with a score of 5–25 at the time of admission.14 Second, the intervention included inspiratory exercises of different intensities and duration through resistance, which was controlled by a threshold valve adapted to the needs and changes of people after stroke as soon as subjects progressed through the study. Third, different types of studies were included: 2 randomized trials, 3 cross-sectional studies, and a pilot study. Furthermore, 3 different types of interventions were included (maximum inspiratory training, controlled intervention, and nonintervention)8 in 3 different groups. One group (control group) carried out a neurological rehabilitation program (NRP) simultaneously with respiratory muscle training at a constant load of 10%, the second group carried out a NRP program and expiratory muscle training with resistance at 50%, and the last group carried out a NRP and inspiratory muscle training with resistance at 50%.5 There also was a study with 3 groups that compared inspiratory muscle training with a group of breathing exercises combined with diaphragmatic exercises with pursed lips and a control group.9
Finally, the outcome measures included functional maximum inspiratory pressure (PImax),8 maximum expiratory pressure (PEmax), respiratory muscle strength, FVC,5 inspiratory capacity, and forced expiratory peak.5,9 Other functional outcome measures, such as Nottingham Health Profile and a self-report questionnaire measuring the level of maximum physical activity,8 were also included.
Studies were excluded if subjects had cognitive difficulties or an intracranial pressure increase.5 In addition, studies were also excluded if the respiratory intervention focused on drainage techniques or aerobic training of peripheral muscles without respiratory muscle training with thresholds valves or only on ventilatory exercises with an incentive spirometer. Six studies were examined after subsequent selection based on the title and abstract. The excluded studies are listed in Appendix 1 (see the supplementary materials at http://www.rcjournal.com).
Evaluation of Methodological Quality
Twenty relevant articles were found in the main databases. Six original studies were examined after subsequent selection based on the title and abstract. After analyzing all primary documents, 6 studies were relevant to this review: 2 randomized controlled clinical trials, 3 cross-sectional studies, and a pilot study. Fourteen articles were excluded because they did not reference inspiratory training with threshold valves in subjects with stroke.
The methodological quality of the 6 studies was evaluated using the PEDro scale.15–17 Two independent reviewers (RM-V and MJC-H) completed the checklist based on the PEDro scale. This scale (0–10) is based on a list developed by Verhagen et al.18 The internal validity of the randomized controlled trials was evaluated. A study with a PEDro score of ≤6 is considered to have a level 1 of evidence (6–8 = good, 9–10 = excellent) and a study with a score of ≥5 is considered to have a level 2 of evidence (4–5 = acceptable, <4 = poor).17
Studies included in this review had PEDro scores of 3–8, as shown in Table 1. Studies were considered of high enough methodological quality if they had a score of at least 5. This was based on the fact that studies with a score closer to 4 did not employ a triple-blind methodology (subject, evaluator, and treatment provider). Applying this evaluation, 2 randomized controlled trials were found to have scores of 7 and 8, respectively; the pilot study had a score of 4; and the 3 cross-sectional studies each scored a 3. The grades of recommendation are listed in Table 2.
Evaluation of Methodological Quality of the 6 Selected Studies
Revised Articles About the Effectiveness of Inspiratory Training in Subjects After Stroke
Results
The main findings of this review are presented in Table 1, an evaluation of the methodological quality of the studies selected according to the PEDro scale. Table 2 shows the articles reviewed regarding the effectiveness of inspiratory training in subjects after stroke. Three articles were found that included information about spirometers.10,12,22 In these articles, respiratory muscle training, performed using threshold pressure load in inspiratory muscles, was included.23 A meta-analysis of the data from the randomized clinical trials was included in this review and is presented in Figure 1.
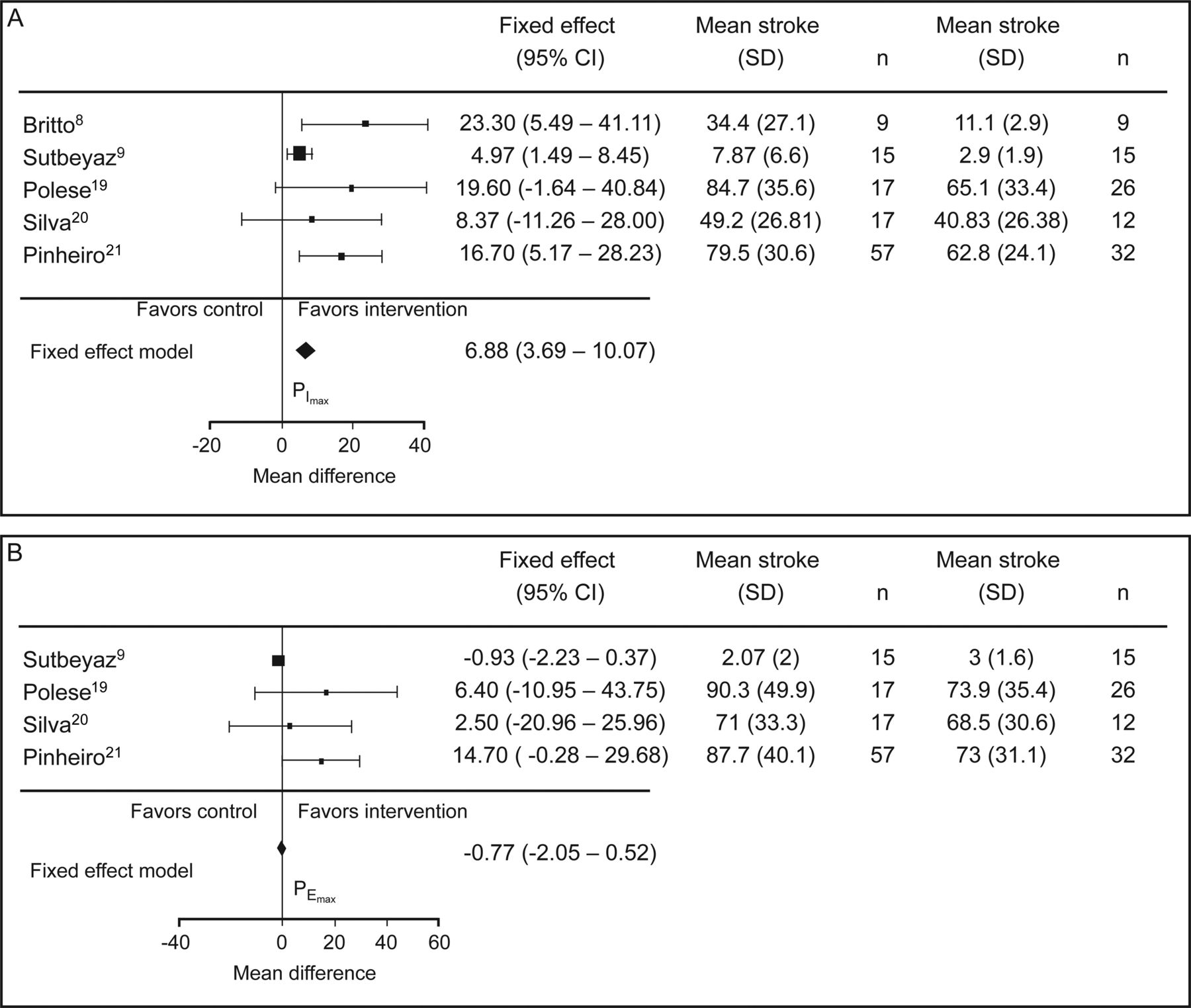
Meta-analysis of data of selected studies on PImax (A) and PEmax (B).
Discussion
This systematic review summarizes the levels of evidence and recommendation grades of different therapeutic respiratory muscle training interventions in subjects after stroke. It has been observed that respiratory muscle training can improve respiratory muscle strength (PImax) and inspiratory muscle endurance (IME) in this population. These findings support the benefits found in subjects with multiple sclerosis24 and COPD.25 In addition, 3 cross-sectional studies were found19–21 recommending the inclusion of respiratory muscle training in the PR program for subjects after stroke.
A study19 compared respiratory muscle strength in chronic stroke subjects according to their physical activity levels and did not find statistically significant results regarding PImax and PEmax outcome measures; however, a 6-min walk test showed statistically significant results regarding respiratory function in active subjects. Nevertheless, other cross-sectional research20 compared respiratory muscle strength in subjects after chronic and acute stroke and showed similar weaknesses in respiratory muscles in both phases. Thus, it was suggested that a program that includes respiratory muscle training for these individuals could improve rehabilitation after stroke.
Another study compared muscle strength in chronic stroke subjects according to their gait speed. It showed statistically significant differences between groups in PImax, but statistically significant differences in PEmax were not found.21 This study recommended respiratory muscle training, especially for subjects with lower functional levels.
Evidence of Respiratory Muscle Training With a Threshold Valve in Subjects After Stroke
Two primary documents gave an A recommendation grade to respiratory muscle training with a threshold valve in subjects after stroke; the authors showed functional and clinically important changes in most outcome measures in each study.8,9 One study had an evidence grade of C.5
First, in the study by Britto et al,8 subjects performed an 8-week training inspiratory muscle protocol at least 5 d/week for 30 min/d, starting with an intensity of 30% PImax and increased 2 cm H2O. At the end of the protocol, the force (PImax) and IME were significantly improved. Thus, the effect size increased to 34.4 (P = .05), and IME increased by 17.4 (P = .05). However, results from self-report questionnaires (Brazilian quality-of-life questionnaire according to the Nottingham Health Profile and the maximum physical activity questionnaire) did not show significant changes. The initial characteristics of participants and questionnaires employed were not sensitive to changes. Although if specific questionnaires had been used for patients with stroke symptoms, the results obtained would have been significant.8
On the other hand, stroke subjects who performed inspiratory muscle training found improvements in dyspnea,9 yet the group that carried out ventilatory re-education exercises improved only in peak expiratory flow. They carried out a program of conventional neurological rehabilitation that was supplemented by an inspiratory muscle training protocol with a threshold valve 6 times/week for 6 weeks with an initial load of 40% until they reached 60% of the PImax. Training was performed for 2 sessions/d, with each session lasting 15 min. After 6 weeks of the training intervention (which showed improvements in muscular inspiratory function associated with an increase in lung volume and exercise capacity), an improvement in dyspnea and quality of life was found using the 12-item Medical Outcomes Study Short Form questionnaire. However, the group that performed diaphragmatic and respiratory exercises with pursed lips and the control group did not show improvement.
Only Kulnik et al5 simultaneously incorporated a neurological PR program and expiratory muscle training. In the design of this research, there were 3 different groups: a control group, which performed a PR program simultaneously with respiratory muscle training at a constant load of 10%; the second group, which carried out a PR program and expiratory muscle training with resistance at 50%; and the final group, which carried out a PR program and inspiratory muscle training with resistance at 50%.
Practical Implications of the Incentive Spirometer for Ventilatory Re-Education
Incentive spirometers play a crucial role in preventing the reduction of mobility of the thoracic cage, and conventionally, spirometers carry out thoracic expansion.22 There are 2 types of spirometers: volume and flow.12 The incentive volume spirometer provides an increase in thoracic expansion and reduces asymmetries of these expansions.12 Thus, spirometers are recommended for patients undergoing stroke rehabilitation. Moreover, the incentive flow spirometer requires more muscle activity in older people because it needs to move a larger volume of air into the thoracic cage.22 Therefore, it is necessary to make a preliminary assessment of patients to consider which kind of spirometer is better suited to their age and clinical conditions.
Subjects who performed breathing exercises with spirometers showed a significant increase in peak expiratory flow.9 In addition, in a recent study, improvements in peak expiratory flow were found for inspiratory muscle training with resisted loads.5
In this search, we highlighted 3 studies regarding ventilatory re-education through conventional breathing techniques.8,10,11 In these studies, subjects completed exercises that improved breathing capacity. These exercises consisted of learning diaphragmatic breathing; for example, the physiotherapist told the subject to conduct an inspiration to fill the abdomen26 or to use inspiratory exercises combined with breathing through pursed lips.10 The physiotherapist helped in proprioception work by placing his or her hand on the subject's abdomen, which facilitated the understanding of abdominal breathing. The physiotherapist used a proprioceptive signal from the breathing equipment to tell subjects when to exhale slowly.10,11
Threshold Devices to Train Respiratory Muscles
There are 5 types of available devices with respiratory valves: Threshold IMT (Philips Respironics, Murrysville, Pennsylvania), POWERbreathe (HaB International, Southam, Warwickshire, United Kingdom), PowerLung (PowerLung, Houston, Texas), Respifit S (Biegler, Mauerbach, Austria), and ORYGEN DUAL (FORUMED, S.L., Catalonia, Spain) (Fig. 2). All articles in this systematic review used the Threshold IMT device, which uses 30% of the PImax to 41 cm H2O (the maximum load that this device can reach).27 The great dearth of studies in this neurological field was a very limiting factor. In fact, only 6 studies on respiratory muscle training were found. Additional studies are required to advance and strengthen existing scientific evidence, which was both limited and varied in its findings. Larger sample sizes are needed to improve respiratory muscle training.

Examples of thresholds valves in respiratory training. A: Threshold IMT. B: POWERbreathe. C: PowerLung. D: ORYGEN DUAL. E: Respifit S.
Finally, it is necessary to carry out a protocol of therapeutic respiratory muscle training interventions for 8 weeks, with a frequency of 3 or 6 d/week for one or two sessions. Each session should consist of 30 min/d or 15 min/set, 2 sets/d, with an intensity of 30–40% of PImax.
Conclusion
This research has examined levels of evidence and recommendation grades of various therapeutic interventions of inspiratory muscle training in people who have suffered a stroke. It has been observed that respiratory muscle training can improve strength and endurance of respiratory muscles in these subjects. At least one 8-week intervention carried out at a frequency of 3 to 6 days/week is recommended. Each session should last between 15 and 30 minutes per set with one or 2 daily sessions per day at an intensity of 30–40% of maximal inspiratory pressure. It is necessary to use the suitable spirometer for each person. The results of this research support physiotherapy respiratory techniques in people who have suffered a stroke.
Footnotes
- Correspondence: R Martín-Valero PhD, Department of Psychiatry and Physiotherapy, Francisco Maldonado University School of Oduna, Campo de Cipreses, 1, 41640 Osuna (Sevile), Spain. E-mail: rovalemas{at}gmail.com.
Supplementary material related to this paper is available at http://www.rcjournal.com.
The authors have disclosed no conflicts of interest.
- Copyright © 2015 by Daedalus Enterprises









{kind=link}
{kind=link}