

Abstract
BACKGROUND: Acid gastroesophageal reflux is a common problem in non-cystic fibrosis bronchiectasis and COPD. Invasive methods are used to diagnose gastroesophageal reflux, but the ability to detect pulmonary microaspiration of gastric contents using this method is unclear. A noninvasive option to detect pulmonary microaspiration is to measure pepsin in exhaled breath condensate (EBC), but this has not been related to esophageal pH monitoring in these lung conditions. This study aimed to measure pepsin concentrations and pH in EBC and to determine the relationship to gastroesophageal reflux in bronchiectasis or COPD.
METHODS: Subjects with bronchiectasis (n = 10) or COPD (n = 10) and control subjects (n = 10) completed 24-h esophageal pH monitoring for detection of acid gastroesophageal reflux, measuring the percentage of reflux time in the proximal esophagus and the DeMeester score (DMS). Concurrently, 3 samples of EBC were collected from each subject, and pH was measured and pepsin concentrations were analyzed by enzyme-linked immunosorbent assay.
RESULTS: EBC pepsin was detected in subjects with bronchiectasis (44%) or COPD (56%) and in control subjects (10%). A diagnosis of gastroesophageal reflux was not associated with a higher concentration of EBC pepsin in bronchiectasis (P = .21) or COPD (P = .11). EBC pepsin concentration did not correlate with DMS (rs = 0.36) or proximal reflux index (rs = 0.25) in subjects with bronchiectasis or with DMS (rs = 0.28) or proximal reflux index (rs = 0.21) in patients with COPD. EBC and sputum pepsin concentrations were moderately correlated in bronchiectasis (rs = 0.56) and in COPD (rs = 0.43).
CONCLUSIONS: Pepsin is detectable in EBC samples in bronchiectasis and COPD. Although no association was found between pepsin concentrations and a diagnosis of gastroesophageal reflux, a moderate relationship between sputum and EBC pepsin concentrations suggests that EBC pepsin may be a useful noninvasive marker of pulmonary microaspiration.
Introduction
Acid gastroesophageal reflux is recognized as a comorbidity of COPD and non-cystic fibrosis bronchiectasis.1–6 Although the significance of gastroesophageal reflux in respiratory conditions has not been clearly established,4 one hypothesis is that gastroesophageal reflux may contribute to the severity of lung disease via pulmonary microaspiration.7 Although the currently accepted standard for diagnosing gastroesophageal reflux is ambulatory 24-h esophageal pH monitoring,8 its potential weaknesses are that it evaluates proximal gastroesophageal reflux by focusing only on esophageal events and that it is an invasive method. An emerging biomarker of pulmonary microaspiration as an indirect marker of gastroesophageal reflux is the detection of pepsin, an enzyme located only in the gastrointestinal tract. Currently, pepsin may be detected in saliva, tracheal aspirates, or bronchoalveolar lavage fluid using proteolytic enzyme analysis9 or immunoassays.10–14 Although it has been recently demonstrated that pepsin is detectable in easily obtainable sputum samples of patients with COPD and bronchiectasis,6 this method imposes limitations for individuals who are not regular producers of sputum or in conditions not associated with sputum production.
An alternative noninvasive method of analyzing airway pH is exhaled breath condensate (EBC).15–17 EBC is a sample of breath water vapor containing pulmonary epithelial lining fluid that has been collected and condensed typically via cooling using a collection device (commonly to 4°C and subzero temperatures). The collection is readily obtainable, with access to fluids lining the pulmonary surfaces without sputum induction or bronchoalveolar lavage. A method used to collect EBC samples involves the portable RTube (Respiratory Research, Austin, Texas), a technique found to be reproducible and comparable in control subjects and those with COPD.18 Acidification of the hypopharynx occurs when gastric acid refluxes above the upper esophageal sphincter, resulting in acidic EBC and thus providing a noninvasive surrogate marker for detection and assessment of gastroesophageal reflux.
Detection of airway acidity based on EBC pH measurement has been described in COPD,19 with a lower pH of EBC following acid aspiration also demonstrated.15 Pepsin has been detected in EBC of patients following lung transplantation, with reduced concentrations following anti-reflux surgery.20 In addition, pepsin in EBC has been detected in patients with COPD with symptoms of gastroesophageal reflux.21 However, the relationship between EBC pH and pepsin and the esophageal pH monitoring profile has not been explored in COPD or bronchiectasis. The aims of this pilot study were (1) to evaluate EBC pH and pepsin concentrations in a group of subjects with COPD or bronchiectasis and control subjects and (2) to elucidate the relationships between sputum and EBC pepsin and EBC pepsin with gastroesophageal reflux parameters.
QUICK LOOK
Current knowledge
Gastroesophageal reflux is a common finding in COPD. Invasive methods are used to diagnose gastroesophageal reflux, but the ability to detect pulmonary microaspiration of gastric contents is unclear. A noninvasive option to detect pulmonary microaspiration is to measure pepsin in exhaled breath condensate (EBC), but the relationship of pepsin in exhaled condensate and esophageal pH monitoring has not been determined.
What this paper contributes to our knowledge
Pepsin was detected in EBC of subjects with bronchiectasis and COPD. There was no association between pepsin concentrations and a diagnosis of gastroesophageal reflux. There was a moderate relationship between sputum and EBC pepsin concentrations, suggesting that this might be a useful noninvasive marker of pulmonary microaspiration.
Methods
Subjects
This pilot study included subjects with stable COPD or bronchiectasis who attended respiratory out-patient clinics of a tertiary hospital (Alfred Health). A diagnosis of COPD was confirmed according to the Global Initiative for Chronic Obstructive Lung Disease criteria,22 with no evidence of asthma according to the Global Initiative for Asthma guidelines.23 A diagnosis of bronchiectasis unrelated to cystic fibrosis was confirmed by high-resolution computed tomography.24,25 Healthy control subjects were consecutively recruited from the community, with no history of smoking, respiratory disease, gastroesophageal reflux symptoms, or use of respiratory or anti-reflux medication. All subjects previously prescribed anti-reflux medication stopped the medication 7 d before the study.8,26 All subjects gave written informed consent, and the study was approved by the administering institution's ethics review committee (Alfred Health 106/05).
Ambulatory, dual-channel, 24-h esophageal pH monitoring was completed using the Polygram 98 ambulatory pH testing system and Digitrapper pH 400 (Medtronic, Minneapolis, Minnesota). Two antimony-tipped probes for distal and proximal monitoring (Slimline SU, Synectics, Lisbon, Portugal) were calibrated to pH 7.01 ± 0.05 (alkaline) and 1.07 ± 0.05 (acid) using pH buffer solution (7.01 and 1.07, Reagecon, CR Kennedy, Melbourne, Victoria, Australia). The distal probe was positioned 5 cm above the lower esophageal sphincter, with the proximal probe 15 cm above the distal probe, using a method previously described.6 The Digitrapper pH 400 with 3 subject-activated event buttons recorded the pH in the proximal and distal esophagus for 24 h. Each subject was instructed to activate the 3 event buttons to record start and finish time of meals, recumbent versus erect posture, and symptoms of gastroesophageal reflux experienced during the study. When symptoms were experienced, each subject was asked to press the event button on the Digitrapper at the beginning of each symptom-related episode. Subjects were encouraged to have as normal a day as possible during the 24-h esophageal pH monitoring with respect to oral intake, recumbent positioning, and all other daily activities to ensure that the results accurately reflected the effects of the subjects' normal life on gastroesophageal function. No restrictions with regard to type and quantity of food or drink or time spent in recumbent or erect position were imposed.
At the conclusion of 24 h, data were downloaded into the Polygram 98 ambulatory pH testing system for analysis. Principal gastroesophageal reflux parameters were the fraction of reflux time (reflux index) for the 24-h period in the proximal and distal esophagus and the DeMeester score (DMS). Based on studies of healthy subjects, the clinical definition of gastroesophageal reflux was a DMS (composite of distal reflux) of > 14.72,27 whereas proximal reflux was defined as proximal esophageal pH of < 4 for > 0.9% of the total study time.28 Symptoms of gastroesophageal reflux were collated using a structured symptom questionnaire, which has been validated against 24-h esophageal pH monitoring.29
Sputum and EBC Sample Collection
During the 24-h study period, EBC was collected using RTubes, with the RTube sleeve cooled to −2°C for a minimum of 1 h before use,30 and 3 samples were collected after insertion of the esophageal pH probe in all subjects. Sputum samples were collected at the same time as EBC samples in those with lung disease. Subjects refrained from eating 2 h before collection. EBC samples were collected during tidal volume breathing for 10–15 min with a nose clip consistent with the method of collection using the RTube.31 EBC pH was measured before freezing using a pH-meter with a thin and sensitive glass electrode (Metrohm 827 pH-meter, MEP Instruments, Gladesville, New South Wales, Australia). The pH-meter was calibrated before use. EBC samples were then aliquoted and immediately stored at −80°C until batch analysis. Due to sputum viscosity, sputum supernatants were prepared by centrifugation (10 min, 2,183 × g) within 4 h of collection, with aliquots stored at −80°C until batch analysis. Samples were stored for < 1 y due to a previous study demonstrating the stability of EBC pH following long-term storage.30
Sputum and EBC pepsin concentrations were tested using a locally developed enzyme-linked immunosorbent assay based on a monospecific antibody to porcine pepsin.11,32 Polystyrene microtiter plates (MaxiSorp, Nunc, Roskilde, Denmark) were coated with goat anti-pepsin antibody, diluted in carbonate-bicarbonate buffer at 0.1 μg/mL, and incubated for 4 h. After washing, wells were incubated with a blocking buffer (1% bovine serum albumin) and stored at 4°C overnight. For the assay, wells were washed, and enzyme controls (for standard curve) and clinical samples were added in duplicate. The signal for captured pepsin was amplified by the addition of biotinylated goat anti-pepsin antibody in Tris-saline buffer, followed by incubation with a secondary antibody (streptavidin-horseradish peroxidase conjugate). Enzymatic color development was carried out using a substrate (0.2% ortho-phenylenediamine) in citrate-phosphate buffer, with the wells read at 490 nm in the microplate reader. The assay was performed by one individual who was blinded to gastroesophageal reflux diagnostic status. For porcine pepsin, the intra-assay coefficient of variation was 4.5%, with an inter-assay coefficient of variation of 13%, and the lower limit of detection of 1.953 ng/mL.
Statistical Analysis
Statistical analysis was performed using SPSS 21.0 (SPSS, Chicago, Illinois). Between-group differences were compared using the Mann-Whitney U test or the Kruskal-Wallis test, as the data were not normally distributed. The correlations between EBC pH, EBC and sputum pepsin concentrations, gastroesophageal reflux parameters, symptom scores, and lung function were analyzed using Spearman's rho. P = .05 was considered to be statistically significant unless indicated otherwise.
Results
A total of 30 subjects were included in the study; 8 (27%) were female. Seven subjects with COPD and 4 subjects with bronchiectasis had been prescribed anti-reflux medication before the study. The majority of subjects with COPD had moderate disease severity,22 whereas those with bronchiectasis were classed as having mild disease. The demographics of subjects are outlined in Table 1.
Subject Demographics
Pepsin in EBC was detected in 60% (n = 6) of subjects with bronchiectasis, 70% (n = 7) of subjects with COPD, and 10% (n = 1) of control subjects, whereas pepsin in sputum was detected in 70% (n = 7) of subjects with bronchiectasis and 90% (n = 9) subjects with COPD.
EBC pH and EBC pepsin was measured in all 3 groups (COPD, bronchiectasis, and controls), whereas sputum pepsin was assessed only in the groups as shown in Table 2. The EBC pH values of control subjects were significantly higher than those of the subjects with COPD or bronchiectasis (P < .01). EBC pepsin concentrations were higher in subjects with COPD and bronchiectasis compared with control subjects (P = .02). Higher concentrations of EBC pepsin were strongly associated with lower EBC pH in subjects with bronchiectasis (rs = −0.78) and subjects with COPD (rs = −0.64), but not control subjects (rs = −0.23). A moderate correlation was observed between sputum and EBC pepsin concentrations in bronchiectasis (rs = 0.56, P = .02) and COPD (rs = 0.43, P = .04).
EBC and Sputum Features in 3 Groups
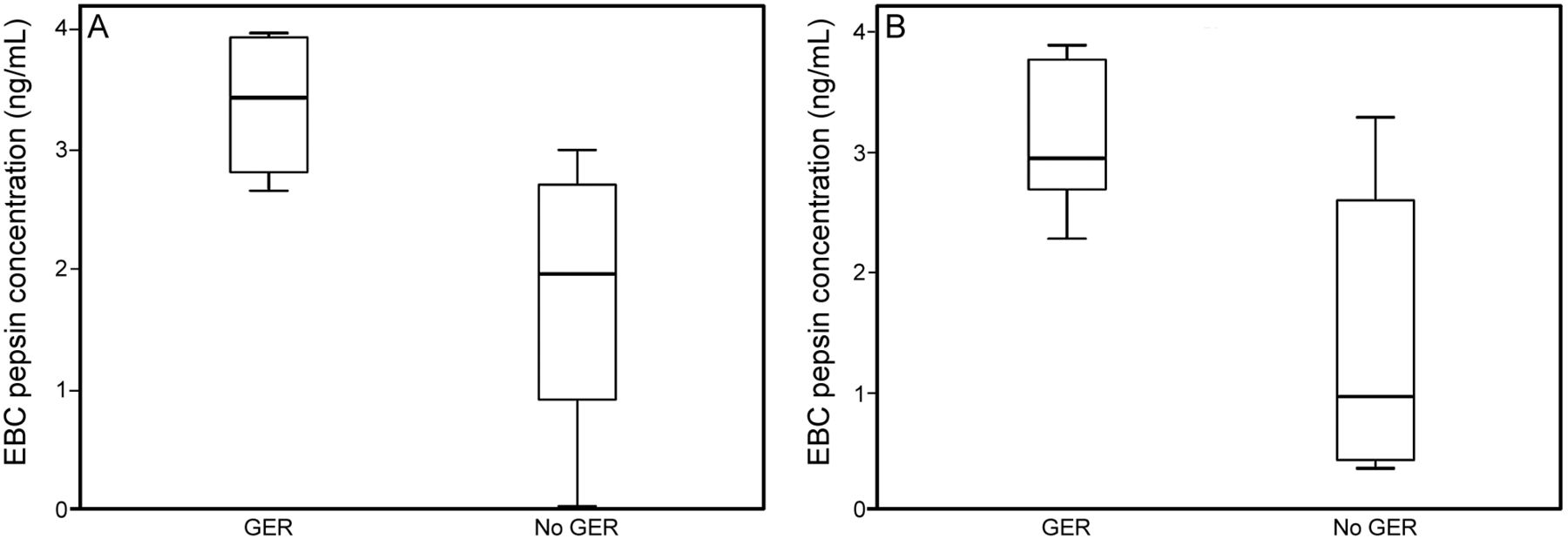
Four subjects with bronchiectasis had DMS scores of > 14.72 and a proximal reflux index of > 0.9%. Five subjects with COPD had DMS scores of > 14.72, whereas 2 subjects had proximal gastroesophageal reflux. In subjects with bronchiectasis, the median (interquartile range) DMS was 16.0 (9.5–23.1), and the proximal reflux index was 0.9 (0.3–2.7). In subjects with COPD, the DMS was 15.2 (4.8–32.2), and the proximal reflux index was 0.2 (0.1–0.5). There was no difference in EBC pepsin concentration in subjects with or without gastroesophageal reflux in the bronchiectasis group (3.42 [2.81–3.9] ng/mL vs 1.97 [0.91–2.73] ng/mL) or COPD group (2.95 [2.69–3.73] ng/mL vs 0.96 [0.41–2.64] ng/mL) (Fig. 1). In subjects with bronchiectasis, there was no correlation between EBC pepsin concentration and DMS (rs = 0.36, P = .76), distal reflux index (rs = 0.07, P = .97), or proximal reflux (rs = 0.25, P = .13). Similarly, in subjects with COPD, there was no correlation between EBC pepsin concentration and DMS (rs = 0.28, P = .34), distal reflux (rs = 0.37, P = .54), or proximal reflux (rs = 0.21, P = .83). The relationship between EBC pepsin concentration and lung function was not significant in bronchiectasis (rs = 0.17) or COPD (rs = 0.29). No relationship was evident between EBC pepsin concentration and symptom scores in bronchiectasis (rs = 0.12) or COPD (rs = 0.17).

Comparison of exhaled breath condensate (EBC) pepsin concentration according to diagnostic status of gastroesophageal reflux (GER) in bronchiectasis (A) and COPD (B). Data are shown as median and interquartile range. A: Bronchiectasis with gastroesophageal reflux (3.42 [2.81–3.9]) versus no gastroesophageal reflux (1.97 [0.91–2.73]). B: COPD with gastroesophageal reflux (2.95 [2.69–3.73]) versus no gastroesophageal reflux (0.96 [0.41–2.64]).
Discussion
Pepsin was detectable in EBC of subjects with a diagnosis of either bronchiectasis or COPD and at higher concentrations compared with subjects without lung disease. Although the presence of EBC is not directly related to a diagnosis of gastroesophageal reflux or specific markers of distal or proximal gastroesophageal reflux according to esophageal pH monitoring in both lung conditions, moderate correlations between pepsin concentrations in EBC and sputum were evident.
To our knowledge, this is the first report relating pepsin in EBC to esophageal pH monitoring findings in bronchiectasis and COPD. The EBC pH in subjects with COPD was consistent with previous reports of pH values in a stable clinical state, which ranged from 7.20 to 7.97.18,19,21,33,34 The lower pH in subjects with respiratory disease compared with healthy control subjects is consistent with earlier comparisons between the 2 groups.16,17,32–34 These lower values for EBC pH in COPD and bronchiectasis may be related to several factors, including airway inflammation, oxidative stress, bacterial colonization, and gastroesophageal reflux.18,30 The moderate correlations between EBC pH and pepsin concentrations in both bronchiectasis and COPD suggest that in this study sample, gastroesophageal reflux may account for the lower pH observed. Lower EBC pH and symptoms of reflux have been previously described in subjects with COPD, with a greater number and severity of gastroesophageal reflux symptoms related to a lower EBC pH.35 More recently, EBC pepsin concentrations and reflux symptoms according to the reflux disease questionnaire were also found to be significantly related.21 Both of these studies considered only the relationship between EBC pH or pepsin and symptomatic reflux. Although our sample of subjects was small, the use of esophageal pH monitoring takes into account the broader profile of gastroesophageal reflux in bronchiectasis or COPD, for which both symptomatic and asymptomatic reflux have been described.3,5,6,36–38
In this study, the absence of a relationship between a diagnosis of gastroesophageal reflux and EBC pepsin concentrations is contrary to the lower EBC pH and higher pepsin concentrations in patients with COPD and symptomatic reflux.21 This may reflect the small number of subjects in this study meeting the criteria for gastroesophageal reflux, a limitation when including subjects irrespective of reflux symptoms. This may also account for the lack of a relationship between symptom scores and EBC pepsin concentration. However, this lack of association is consistent with some reports of pepsin present in upper airway samples in individuals with lung disease in whom a diagnosis of gastroesophageal reflux could not be confirmed by esophageal pH monitoring.9–13,39 The DMS that was used to define gastroesophageal reflux in this study considers not only the frequency of reflux episodes but the position in which they occur (upright or supine) and their duration.27,40 Short isolated reflux episodes that result in occult aspiration and influence pepsin concentrations in EBC and sputum may be sufficiently infrequent to be detected by esophageal pH monitoring. Similarly, the small proportion of subjects demonstrating significant proximal reflux is a likely explanation for the lack of association between proximal reflux measures and EBC pepsin concentration. The timing of EBC sample collection was selected at random and was irrespective of reflux symptoms; this may influence the ability to fully describe the relationship between gastroesophageal reflux and EBC pepsin. The relationship may also be influenced by the overall EBC pepsin concentrations, which are lower than median levels evident in bronchoalveolar lavage samples (8.3–541 ng/mL) in lung transplant recipients10,11,14,40–42 and in individuals with pharyngeal reflux (up to 200 ng/mL).12,36,43 This lower concentration may be at the limit of the detection threshold for the enzyme-linked immunosorbent assay used in this study, which may influence the ability to detect a relationship in some patients.
Although the lack of a relationship between EBC pepsin concentration and spirometry measures suggests that the effect of pulmonary microaspiration of gastric contents on lung function in patients with COPD and bronchiectasis remains unclear, the power of this pilot study is limited and unable to describe this effect. A previous study of subjects with gastroesophageal reflux suspected of aspiration had an average pH of 5.1 in the peripheral bronchial branches44 as assessed by test strips positioned in these branches during bronchoscopy. Although no significant difference in FEV1 or FVC was found, lower measures of diffusion capacity in relation to gastroesophageal reflux were demonstrated, with the hypothesis that the acidic environment is responsible for resultant alveolar collapse and the development of microatelectasis and inflammation in the lung parenchyma.44 Both the diffusing capacity of the lung for carbon monoxide and the carbon monoxide transfer coefficient may be more sensitive indicators of the effect of gastroesophageal reflux on lung function, therefore providing a more accurate reflection. As these measures of lung function have not been included in this or previous studies, future exploration of the association between EBC pepsin and diffusion capacity measures in bronchiectasis and COPD is warranted. In addition, a higher frequency of exacerbations in subjects with COPD diagnosed with gastroesophageal reflux has been demonstrated.35,45 Evaluation of the link between EBC pepsin and trends in exacerbation frequency and longitudinal change in lung function, which was not measured in this study, in both COPD and bronchiectasis is required for greater understanding of the clinical application of this noninvasive marker.
Although these pilot results are encouraging for the proposed use of EBC as a marker of pulmonary aspiration of gastric contents in lung disease as evidenced in COPD and bronchiectasis, further clarification of this relationship with a larger sample across a broader range of disease severity is warranted. Despite this, these findings suggest that in patients with bronchiectasis or COPD who are being investigated for gastroesophageal reflux, measurement of pepsin levels in EBC has potential use as a noninvasive biomarker of aspiration. Although pepsin has been detected in sputum of patients with these respiratory conditions,6 for those patients who do not produce sputum or in whom induced sputum is not indicated/contra-indicated, EBC (an easily obtainable sample) may be a suitable alternative.
Conclusions
In conclusion, pepsin is detectable in EBC of patients with either non-cystic fibrosis bronchiectasis or COPD. Further work to validate this method of diagnosing pulmonary aspiration of gastric contents using ambulatory esophageal pH monitoring in a larger proportion of patients with these conditions is necessary to determine whether EBC is a useful tool in the routine noninvasive diagnosis of pulmonary aspiration.
Footnotes
- Correspondence: Annemarie L Lee PhD, Physiotherapy, Melbourne School of Health Sciences, The University of Melbourne, 161 Barry Street, Carlton 3010, Melbourne, Victoria, Australia. E-mail: annemarie.lee{at}westpark.org, annemarielee257{at}gmail.com.
This study was supported in part by the Physiotherapy Research Foundation of the Australian Physiotherapy Association and by the Australian National Health and Medical Research Council. The authors have disclosed no conflicts of interest.
- Copyright © 2015 by Daedalus Enterprises









{kind=link}