

Abstract
This systematic review focuses on respiratory effects of inhalational marijuana. The systematic review of the literature was conducted using a comparative method between 2 researchers. Abstracts were reviewed for inclusion of respiratory effects related to inhalational marijuana. Relevant abstracts were collected, and full text articles were retrieved for review. Articles were removed if they did not contain burning marijuana; were animal studies; or were editorials, systematic reviews, commentaries, non-English language, or non-respiratory-related articles. Forty-eight articles were collected and categorized by respiratory effects. In particular, lung cancer, bullous emphysema/COPD, and other respiratory symptoms were the primary categories. Articles were noted by study population country, sample size, age distribution, and findings that were pertinent to respiratory health. The research indicates that there is a risk of lung cancer from inhalational marijuana as well as an association between inhalational marijuana and spontaneous pneumothorax, bullous emphysema, or COPD. A variety of symptoms have been reported by inhalational marijuana smokers, including wheezing, shortness of breath, altered pulmonary function tests, cough, phlegm production, bronchodilation, and other symptoms. It is important to stay current with research findings to educate patients on this smoking behavior.
Introduction
Cannabis (marijuana) is the most commonly used drug in the United States and abroad. Marijuana consists of the dried leaves and flowers of the Cannabis sativa plant. Because of environmental influences on plant growth, chemical potency varies.1 Over 60 cannabinoids and 400 compounds have been identified in marijuana.2 Most common among these cannabinoids is THC (1-δ-9-tetrahydrocannabinol), which is believed to be the primary cannabinoid responsible for the psychoactive effects produced from consumption. The primary differences between marijuana smoke and cigarette smoke are the cannabinoids in marijuana and the nicotine in cigarette smoke. Nicotine is known to be the addictive substance of cigarette smoking. With the illicit nature of marijuana, less research has been conducted on the constituents of the smoke and on the respiratory effects of inhalational marijuana. However, both contain cancer-causing nitrosamines, polycyclic aromatic hydrocarbons, vinyl chlorides, and phenol.3
Before the Marijuana Tax Act of 1937, cannabis was used medicinally, and in 1970, it was classified as a Schedule 1 drug due to the potential for abuse, lack of acceptance as medical treatment, and lack of safety.4 Other drugs in the Schedule 1 category include heroin, ecstasy, and lysergic acid diethylamide (LSD).5 Over the past several years, legalization of recreational cannabis has occurred in 4 states and the District of Columbia, which will help to propel and allow more research on this formerly illicit drug.6 The use of cannabis has steadily increased over the years, with current past month users estimated at 19.8 million people.7 Adolescent use and perception has remained stable in recent years according to the National Institutes of Health.8 Nearly 64% of high school seniors in 2014 viewed cannabis as being not harmful compared with 35% in 1994.
The widespread use of marijuana has raised concerns for medical practitioners regarding the long-term respiratory effects. Most research has considered mental health effects, but research on respiratory effects has not been explored recently. Our systematic review of the literature serves to describe what empirical literature exists on the respiratory effects of inhalational cannabis, in particular. Although cannabis is consumed in various forms, our research study and comprehensive literature review was particularly focused on the inhalational effects to better serve as a comprehensive guide for respiratory therapists, pulmonologists, and others in the health-care field.
Review of the Literature
Search Strategies
Inhalational marijuana peer-reviewed articles published from 1967 to 2015 were identified from the PubMed, OVID, and Web of Science databases using the search terms shown in Table 1. Retrieval of the peer-reviewed articles was performed by 2 researchers (JBM and AM). The initial review commenced with an abstract review to exclude any commentary letters, reviews, editorials, non-English language studies, and animal studies (ie, non-research studies applicable to respiratory, synthetic marijuana, and medical cannabis). Additionally, the reviewers restricted the search to inhalational marijuana only and were focused only on its respiratory health effects.
Search Terms and Databases
The search term “lung diseases/chemically induced” revealed 27,220 abstracts. An advanced search on “lung diseases/chemically induced” was conducted using the term “marijuana” and resulted in one abstract therefore, similar search with term “respiratory system/drug effects*” yielded 2,548 abstracts. Abstracts that could not be categorized based on the lack of information provided in the abstract were reviewed in full text form to allow a final decision regarding classification.
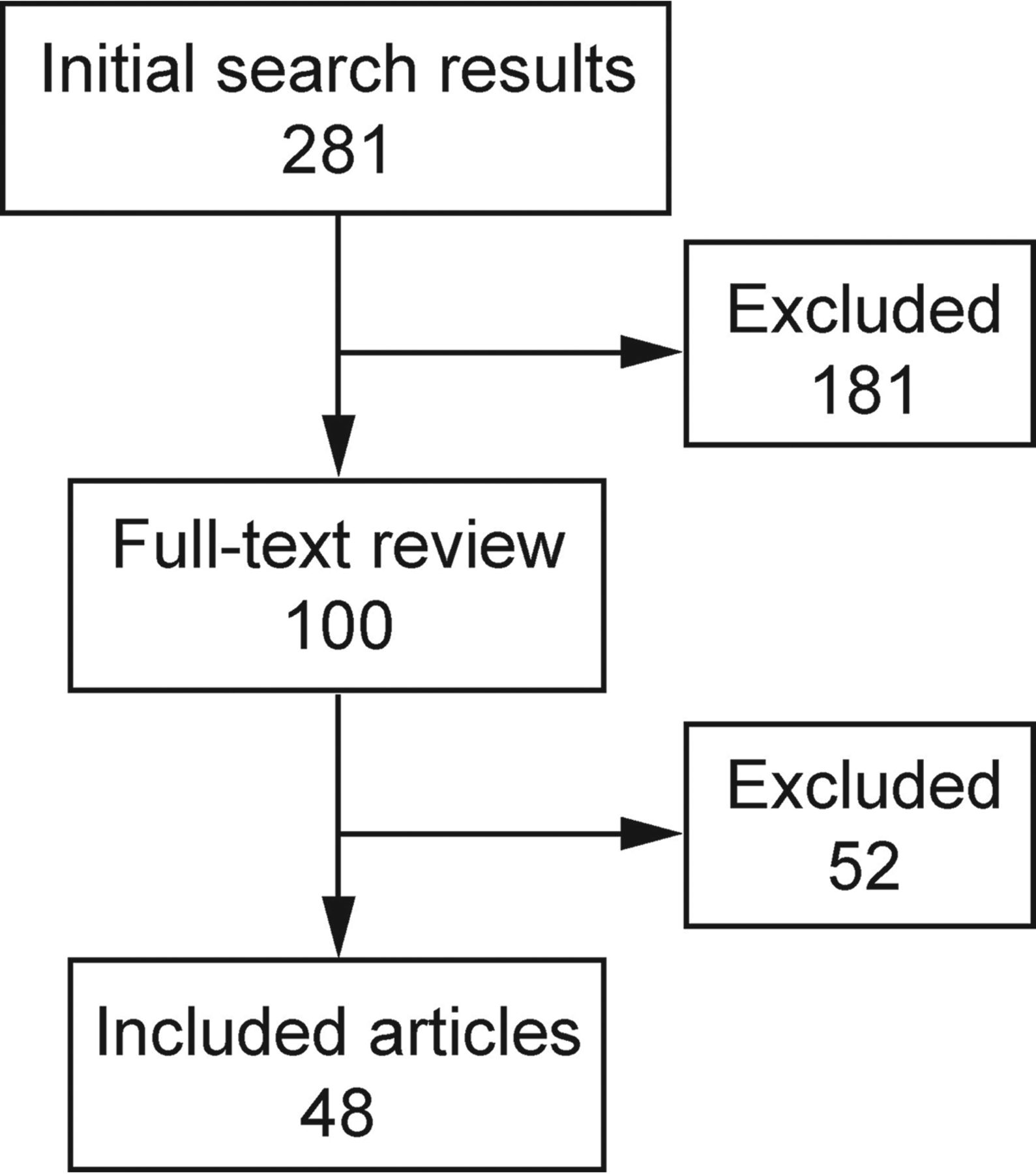
We identified 281 abstracts (250 from PubMed, 2 from OVID, and 29 from Web of Science) through the literature search, as noted in Figure 1. Omitted abstracts included any duplicates, systematic reviews, editorials, commentaries, non-English language articles, animal studies, unattainable full text articles, or those that were not inclusive of respiratory health. An additional 19 unidentified abstracts were listed but provided no direct access to the full text. Of these, 100 articles were reviewed for inclusion. Fifty-two were removed for lack of fit with the inclusion criteria. The final 48 articles were included in this systematic review.
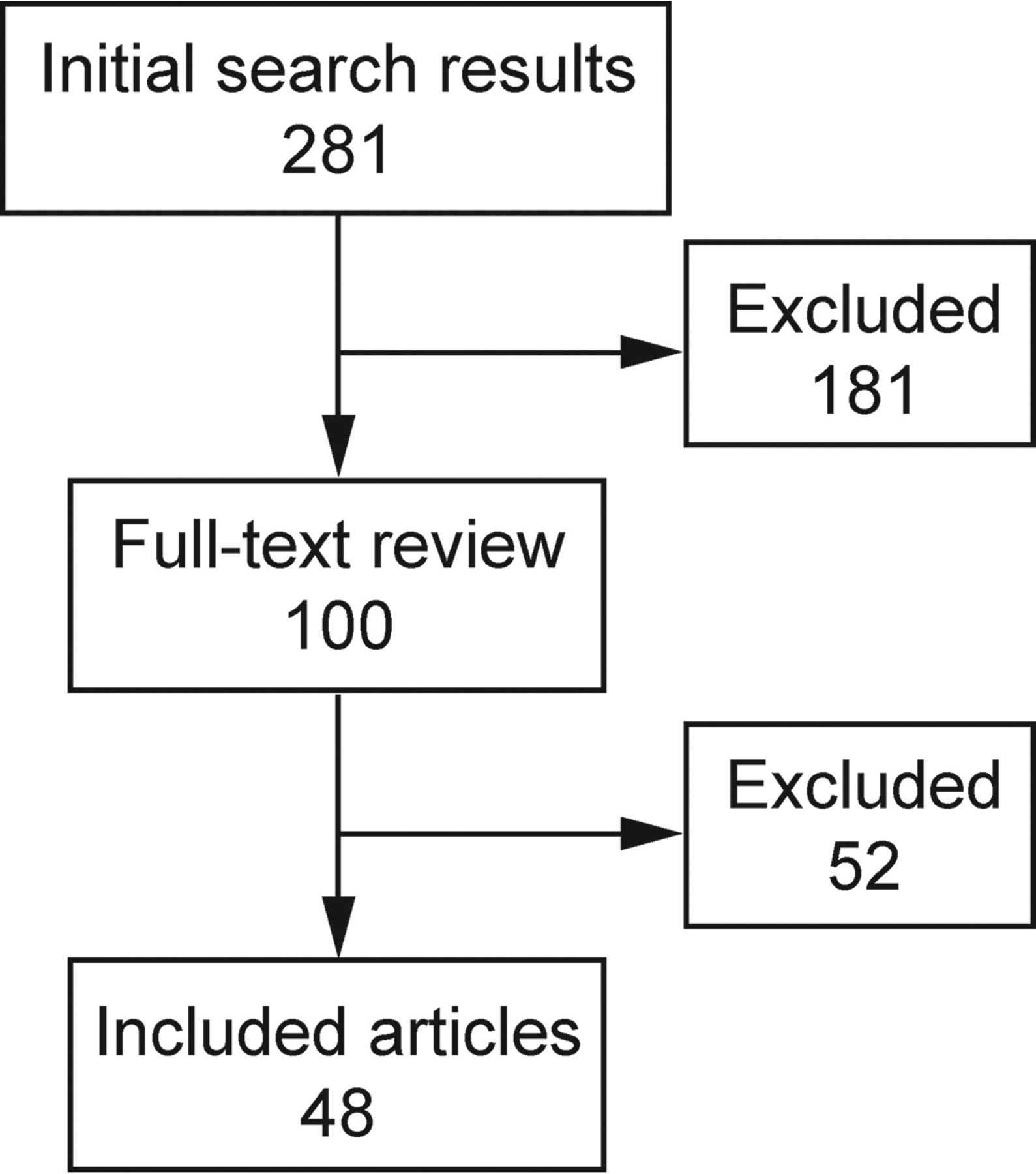
Flow chart.
After review of the articles, we developed a matrix to delineate articles by date of publication, study design, study population and country, age of study participants, and findings deemed important to respiratory health. Furthermore, the studies were organized into tables by disease. Table 2 indicates studies that primarily addressed lung cancer; Table 3 describes studies related to bullous emphysema, COPD, or pneumothorax; and Table 4 categorizes studies that reflected various respiratory-related symptoms or findings in cannabis smokers.
Lung Cancer and Inhalational Marijuana
Bullous Emphysema, Pneumothorax, and COPD Articles Associated With Inhalational Marijuana
Other Respiratory Symptoms and Inhalational Marijuana
Results
Our synthesis of the data represents a more current literature review on the inhalational health effects of marijuana use and other risk factors.57–60 Our findings are consistent with other systematic reviews that confirm studies indicating that marijuana use poses negative respiratory effects in smokers.12,16,61 Our study categorizes the literature by study type and generalized findings helpful for health-care professionals.
Regarding lung cancer risk, 12 studies were retrieved from the systematic review and are noted in Table 2. Of these studies, 4 were case-control studies,9,11,15,20 one was an experimental study,10 4 were secondary data analyses of cohort studies,12,13,16,18,21 one was a secondary data analysis of pathology reports,19 and 2 were case reports.14,17 Seven of the studies involved United States participants; one study was based out of New Zealand; one was based out of the United Kingdom; one was a pooled cohort from Tunisia, Morocco, and Algeria; one study involved Swedish military personnel; one study involved a cohort of Australian adults; and a final study was based solely on Tunisian males. The majority of the studies involved male and female adults. Eight of the studies indicated an increased risk of lung cancer from cannabis use or cases indicating lung cancer occurrence,9–12,14,16,17,19,20 and 4 studies found either no significant association or a lower risk for lung cancer.13,15,18,21 Some of the studies controlled for the effects of tobacco smoking in the data analysis. Of those that found an association, the risk range varied from 2.1- to 4.1-fold increased risk.
Our findings on lung bullae formation indicate research primarily involving case study reports with small sample sizes and 5 studies of larger sample size. Lung bullae were noted in 5 of the cases, as seen in Table 3. The bullae were noted in the middle to upper lung fields, with one mediastinum case.22,25,27,32,26 One subject was diagnosed with a pneumomediastinum upon review of symptoms and x-ray.24 Use of the bong for cannabis smoking is suggested as probably prompting the pneumomediastinum. Fiorelli et al22 conducted a matched study based on pneumothorax pathology and ascertained that of the study sample, younger smokers age <35 y were more likely to exhibit lung bullae.
COPD, emphysema, and lung hyperinflation were also noted in marijuana smokers.23,24,28–31 In particular, a study by Tan et al31 assessed self-symptoms and spirometry in a sample of >800 Canadian males and females to indicate a relationship between COPD and inhalational marijuana. Hancox et al23 published a population-based cohort study and did not find enough evidence for air flow obstruction but did indicate that hyperinflation is related to inhalational marijuana.
Other respiratory symptoms, infectious disease transmission, and altered pulmonary effects were noted in many of the studies found in Table 4. Five studies indicated symptoms such as wheeze, shortness of breath, phlegm production, and/or chest tightness.33,34,39,42,49,54 In contrast, 2 studies indicated bronchodilatory effects from inhalational marijuana.38,42 From a pulmonary function standpoint, one study found a significant V̇max75 in females and a significant FEV1/FVC in males.34 Studies by Pletcher et al45 and Roth et al46 found no abnormal spirometry. One author found significant increases in specific airway conductance,51 whereas a later study found specific airway resistance to be lower in marijuana smokers compared with nonsmokers.52 In a later study, the same author found airway conductance and airway resistance to be worsen in male cannabis users.53
Aspergillosis, legionnaires, tuberculosis, opportunistic infections, and eosinophilic pneumonia were noted in several studies, probably due to the device harboring opportunistic infectious agents that are inhaled into the respiratory system.35,40,43,44,47,48 Several of the bacterial transmission had been found in other shared smoking devices, such as hookah smoking pipes. One study found through bronchoalveolar lavage that the bronchoalveolar effects of cannabis on lymphocytic subpopulations increased in magnitude,55 and a contrasting study found smaller degrees of lung injury as compared with traditional cigarette smoking.36
Another respiratory effect involved carbon monoxide levels that were assessed with smoking cessation subjects indicating slightly higher CO levels with blunt use compared with non-cannabis users.41 There was no evidence of increased oxidants in cannabis users as compared with nonsmokers.50 The secondhand effects of marijuana smoke were evidenced in a case where an infant was exposed to the smoke and experienced altered state of consciousness, indicating that smoking can be toxic around infants.56 Tainted marijuana resulted in acute respiratory failure in 2 case reports.37
Conclusions
Although much is known about tobacco smoke, less is known about marijuana smoke, and inferences cannot be made about one based on the other. Both types of smoke contain particulate matter and carcinogens; however, it has been reported that marijuana components may minimize some carcinogenic effects.62 The particulate matter has an inflammatory response effect on the pulmonary system. There is some evidence in large studies to indicate that inhalational marijuana has adverse effects on the respiratory system22,25,28,31,34,53 and, conversely, bronchodilatory effects.42 More evidence is needed to support or refute these claims. In particular, direct relationships need to be formulated to avoid confounders in making cause/effect claims. With increasing usage and legalization of marijuana, more research will surface and serve to validate or refute current studies that are presented. Clearly, there are limitations in some of these studies based on self-reporting and also with subjects who smoke cigarettes alongside of their marijuana behavior. It is difficult to make claims of cause and effect with known effects of traditional cigarette smoking confounding some studies. Despite the limited research and limitations in the research on inhalational marijuana, the evidence provided does serve to educate respiratory therapists, pulmonologists, or other health-care professionals and provide knowledge of evidence-based research that can be shared with subjects who currently smoke cannabis.
Footnotes
- Correspondence: Mary P Martinasek PhD, MPH, RRT, 401 W. Kennedy Boulevard, Box 30F, University of Tampa, Tampa, FL 33618. E-mail: MMartinasek{at}ut.edu.
The authors have disclosed no conflicts of interest.
- Copyright © 2016 by Daedalus Enterprises









{kind=link}