

Article Figures & Data
Figures
- Fig. 1.
Cross-sectional cut through the active expiration assistance device. During inspiration (A), the outflow tract (1) and the side port (2) are closed (red circles), and the supply flow (3) is directed to the patient via the patient tract (4). During expiration (B), the side port is closed, and the supply flow is directed to the jet nozzle (5). There, following the Bernoulli principle, it creates a negative pressure, resulting in an active expiratory flow. When the side port is open, the system is inactivated (not shown).
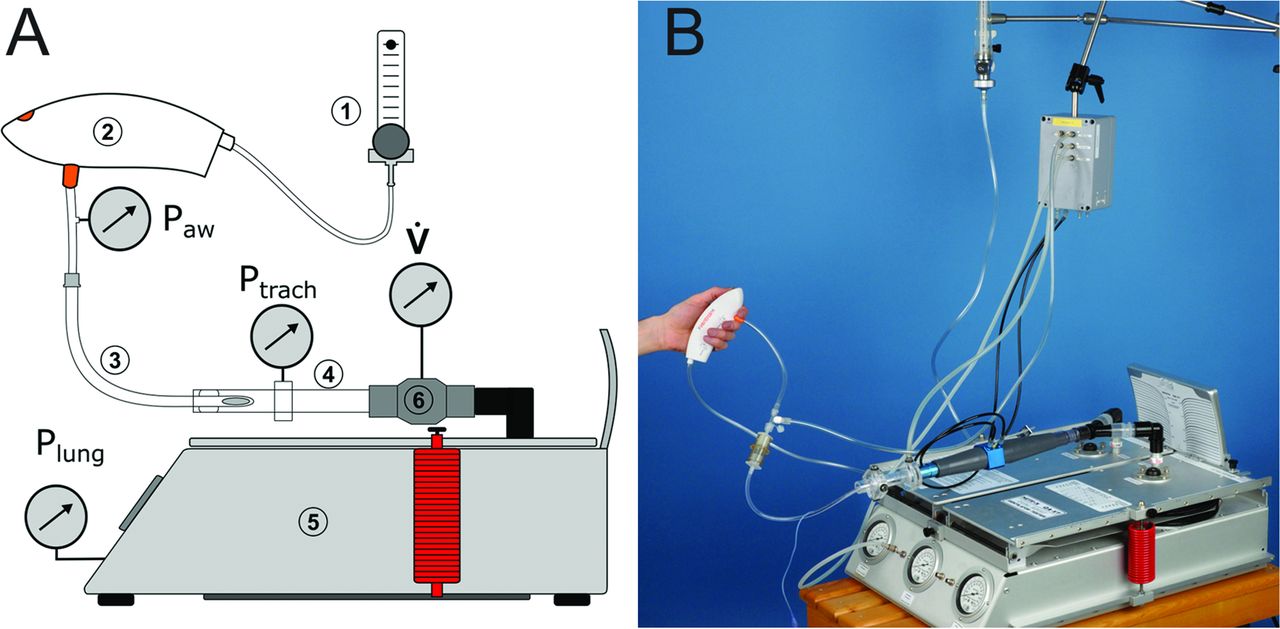
- Fig. 2.
Schematic (A) and photograph (B) of setups. A supply device (1) delivered the driving flow to the active expiration assistance device (2), which was connected via the respective tracheal tube (3) or catheter to a tracheal model (4). The tracheal model was connected to the physical lung model (5) via a pneumotachograph (6) for measuring flow (V̇). Airway (Paw), tracheal (Ptrach), and lung (Plung) pressures were measured at the proximal and distal tips of the tracheal tube or catheter and inside the lung model, respectively. In the measurements including conventional ventilation, the active expiration assistance system was replaced by the ventilator.
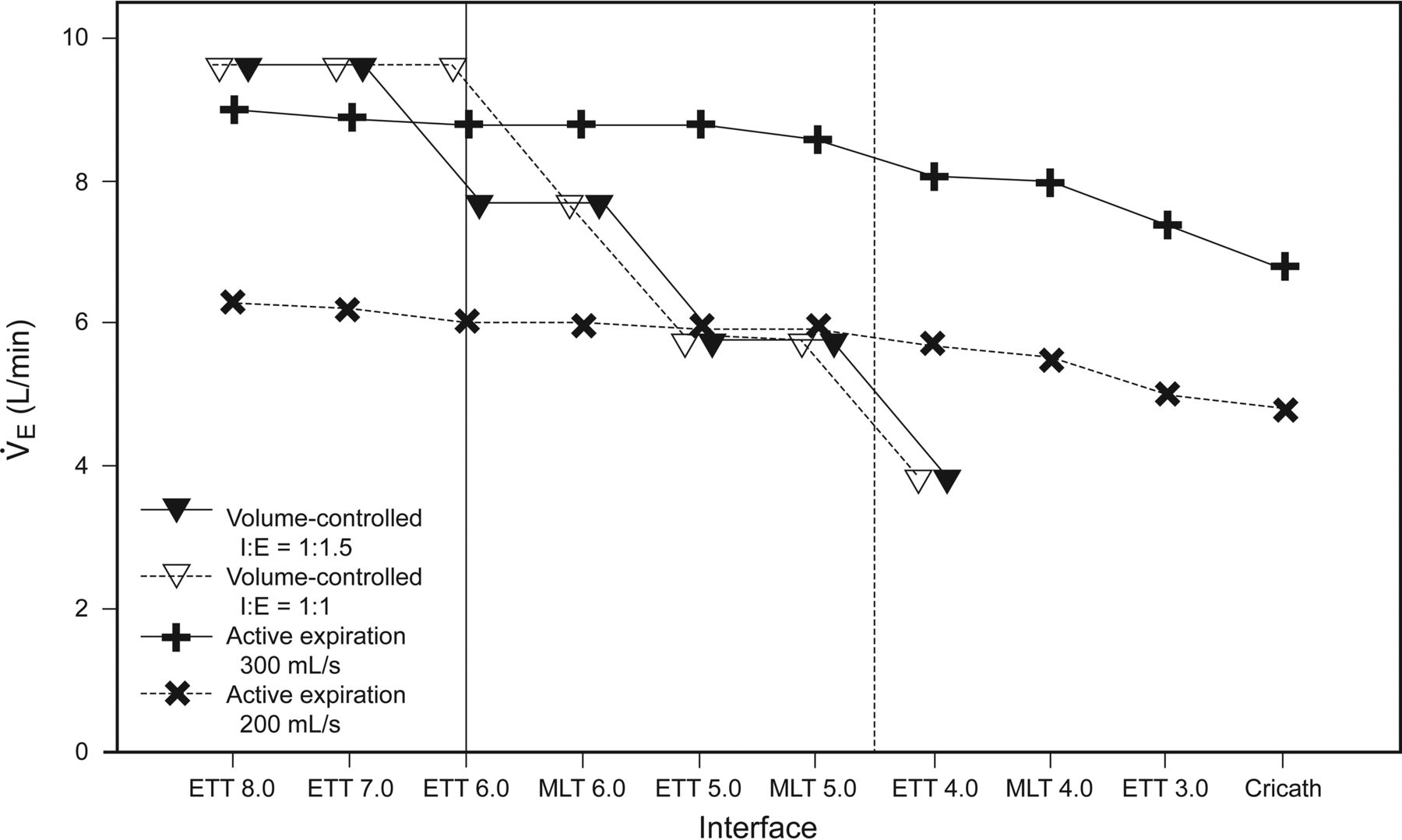
- Fig. 3.
Comparison of the respiratory minute volumes achieved via active expiration assistance and via volume-controlled ventilation (tidal volume = 640 mL, PEEP = 5 cm H2O) without generating intrinsic PEEP (≥1 cm H2O). Vertical lines represent the cut-off where ventilation via active expiration assistance with 200 mL/s (solid) or 300 mL/s (dashed) was superior to conventional mechanical ventilation (viewed from right to left) in terms of higher generable minute volume (as indicated by the crossings of the connecting lines). Missing values (volume-controlled ventilation for MLT 4.0, ETT 3.0 and cricath) indicate that no conventional ventilation could be established without generating intrinsic PEEP <1 cm H2O. ETT = endotracheal tube; MLT = microlaryngeal tube; cricath = cricothyrotomy catheter.














{kind=link}
{kind=link}
{kind=link}