

Abstract
BACKGROUND: The objective of this work was to evaluate the time course of clinical and health-related quality of life outcomes of long-stay ICU survivors' and caregivers' burden.
METHODS: The study included 23 subjects of mixed diagnosis (66 ± 11 y, body mass index 26.5 ± 5.6 kg/m2) with a recent episode of acute respiratory failure needing in-hospital rehabilitation. Subjects and caregivers were evaluated at hospital discharge (T0, n = 23) and 6 months later (T6, n = 16). At T0 and T6, subjects' clinical status (Dependence Nursing Scale), FVC (percent-of-predicted FVC and percent-of-predicted FEV), maximum inspiratory/expiratory pressures, effort tolerance (sit-to-stand, Takahashi test, 6-min walking distance), and disability (Barthel index) were evaluated. EuroQol-5D (EQ-5D), McGill Quality of Life, General Perceived Self-Efficacy Scale, and Hospital Anxiety and Depression Scale (HADS-A/HADS-D) were assessed. Caregivers' burden was measured by the Family Strain Questionnaire short form and Caregiver Needs Assessment. Correlation between subjects' clinical status and caregiver assessments was performed at T0.
RESULTS: At T0, subjects showed compromised EQ-5Dindex (0.42 ± 0.28); 69% of caregivers had high Family Strain Questionnaire and moderate Caregiver Needs Assessment scores (30 ± 13). EQ-5Dindex was significantly related to Dependence Nursing Scale score (P < .001), percent-of-predicted FVC (P < .02), effort tolerance (all P < .01), disability (P < .001), and caregiver Family Strain Questionnaire score (P < .02). At T6, subjects significantly improved percent-of-predicted FVC (P < .05), maximum expiratory pressure (P < .01), effort tolerance (all P < .05), disability (P < .02), and EQ-5Dindex (P < .05), whereas caregivers' burden scores were unchanged. However, the percentage of caregivers with strain increased.
CONCLUSIONS: In prolonged-ICU-stay survivors, EQ-5Dindex at hospital discharge is related to clinical status and caregivers' strain. Subjects' clinical status and EQ-5Dindex improves over time, but caregivers' burden remains high, suggesting the need to monitor/support caregivers.
- respiratory failure
- anxiety
- depression
- self-efficacy
- health-related quality of life
- family caregiver
- intensive care
Introduction
In the last 15 y, increased availability of beds in ICUs and new technologies coupled with improved levels of care have highlighted a new category of subjects identified as survivors of a catastrophic illness.1 This group of survivors is a heterogeneous population regarding characteristics such as age, cause of illness, comorbidities, and family situation.1 Some of these patients experience a prolonged stay in ICU (>7 d) and long and difficult time of mechanical ventilation (>20 d).1 These patients have limited clinical outcomes2 and may suffer depression or anxiety,3–5 with decreased health-related quality of life (HRQOL)6,7 in the months following intensive care. Indeed, patients continue to require health-care services, but few of them are transferred to rehabilitation facilities.8–11 Individualized rehabilitation can benefit ICU patients12 and, indirectly, sustain their relatives who, once at home, start to experience the responsibility of providing care12 with consequences for their personal needs.13
Knowledge of both clinical and HRQOL outcomes in survivors after a critical illness is crucial for planning early interventions for the patient and evaluating their effects in family members. Although some attention has been paid to the patient, the caregiver's strain and needs have been investigated mainly during the continuum of the hospital stay.13,14 Limited investigations have explored the patients' clinical outcomes and HRQOL and impact on caregivers' burden after a long period of in-hospital stay and rehabilitation and during the following months back home. This is a very important point, since there is little knowledge about changes of long-stay ICU patients and caregiver characteristics during a follow-up after rehabilitation.
The first aim of this paper was to evaluate the relationship between the long-stay ICU survivors' clinical status (in terms of respiratory and disability outcomes, and HRQOL) and its effect on family caregivers' burden at the time of rehabilitation discharge. The second aim of the study was to describe the characteristics of long-stay ICU survivors and their caregivers over time.
QUICK LOOK
Current knowledge
The impact of critical illness is profound and long-lasting both for subjects emerging from an ICU stay and for their caregivers. Limited investigations have explored long-ICU-stay survivors' clinical outcomes and health-related quality of life (HRQOL) and their impact on caregivers' burden after a long period of in-hospital stay and rehabilitation (T0) and the following months back home (T6).
What this paper contributes to our knowledge
The current paper studied the caregiver's burden as a condition dependent on the clinical and HRQOL outcomes observed in long-ICU-stay survivors discharged home after a long period of in-hospital rehabilitation. Caregiver burden was tested by the use of 2 questionnaires (strain and needs) never used in this caregiver population, at T0 and T6. Despite the fact that subjects' functional autonomy and HRQOL improved at T6, caregivers' burden was still high and similar to that observed at T0 but tended to involve a higher percentage of caregivers requiring urgent psychological help.
Methods
A prospective study was carried out in subjects admitted to the Salvatore Maugeri Foundation's rehabilitation center in Lumezzane, Brescia, Italy between April 15, 2011 and April 15, 2013 and their caregivers. The review board of the Fondazione Salvatore Maugeri approved the study (CEC Deliberation 751), and written informed consent was obtained from all participants. Caregivers also signed an informed consent at the time of their next-of-kin's discharge from hospital. All patients, irrespective of diagnosis, age ≥18 y, discharged from our rehabilitation center who (1) had experienced a recent (≤3 months) episode of severe acute respiratory failure, (2) had had a prolonged stay in the ICU (lasting ≥20 d),1 (3) had completed the in-hospital rehabilitation program, and (4) underwent psychological assessment at the time of discharge (T0) were eligible for the study.
The in-hospital multidisciplinary rehabilitation program has been described elsewhere.15 Counseling (one session or repeated sessions, depending on the subject's/caregiver's needs) was a part of the in-hospital program and was proposed to subjects/caregivers by a psychologist only during the subject's rehabilitation stay. No structured program was provided to the subject or caregiver over time. When discharged home, subjects were considered as under usual care (ie, drug and oxygen therapy, mechanical ventilation [if necessary], occasional visits from the general practitioner or nurse, and in-hospital check-ups on demand [ie, referred by the general practitioner] as required). Subjects were free to conduct physical activity without any monitoring or reinforcement provided by the hospital (ie, no structured program of rehabilitation was provided).
Measures
At hospital discharge (T0), anthropometric data (weight and body mass index), admission diagnosis (post-cardiac surgery, acute respiratory failure, COPD, or neurological disease), length of ICU and in-hospital rehabilitation stay, preexisting comorbidities evaluated by Cumulative Illness Rating Scale score,16 tracheostomy (%), and need for mechanical ventilation (%) were collected.
Twenty-four h before T0, subjects' clinical status (Dependence Nursing Scale),17 respiratory function (FVC, percent-of-predicted FVC, FEV1, percent-of-predicted FEV1, maximum inspiratory and expiratory pressures (cm H2O),18 dyspnea by means of the Borg scale,19 and arterial blood gases, effort tolerance (sit-to-stand test),20 Takahashi test,21 6-min walking distance,22 and general disability with the Barthel index23 were collected by health staff (physicians and physical therapists) (Table 1).
Measures Used for Subjects and Caregivers
Assessments
At T0, several validated questionnaires were used to assess subjective variables. HRQOL was measured using the EuroQol 5D (EQ-5D), a generic multiattribute health-state classification system,24,25 and the McGill Quality of Life Questionnaire (Italian version)26,27; self-efficacy was assessed by the General Perceived Self-Efficacy Scale28,29; and anxiety/depression was assessed by the Hospital Anxiety and Depression Scale (HADS Anxiety [HADS-A] and Depression [HADS-D]).30,31 All evaluations were repeated at T6 during the outpatient's visit.
Evaluations of strain and needs were performed by a family caregiver who was primarily responsible for providing care to survivors. At T0 and T6, a psychologist administered 2 different questionnaires: the Family Strain Questionnaire short form32 and Caregiver Needs Assessment33 (Table 1). These questionnaires have never been used for caregivers of ICU subjects. Afterwards, we classified 2 main subgroups of caregivers: low strain (the 2 first subgroups of the Family Strain Questionnaire short form [score ≤11]) and high strain (score ≥12). Only the high strain subgroup is suggested for a psychological intervention. We considered caregivers as having an improved level of strain over time if they presented a change in the Family Strain Questionnaire short form score causing a shift from an area of more severe strain to one of less strain at the retest (T6). We considered as having improved needs those caregivers who presented a reduction in the Caregiver Needs Assessment score of ≥1 point at the retest (T6). Precise timing and details of all of the above evaluations are shown in Table 1 (with further details in supplementary Table 1 at http://www.rcjournal.com).
Statistical Analysis
Statistical analysis was performed using the software STATA 11.2 (StataCorp LP, College Station, Texas). The Shapiro normality test was applied for the evaluation of normal data distribution. All data were expressed as the median (25th to 75th percentiles). The relationships between subjects' general clinical status (Dependence Nursing Scale score, dyspnea, respiratory function [percent-of-predicted FEV1, percent-of-predicted FVC, maximum inspiratory/expiratory pressure, and arterial blood gases], effort tolerance [sit-to-stand, Takahashi test, and 6-min walking distance], disability [Barthel index]), General Perceived Self-Efficacy Scale, and HADS) and HRQOL (EQ-5D and McGill Quality of Life) as well as caregivers' strain (Family Strain Questionnaire short form) and needs (Caregiver Needs Assessment) were evaluated by the Spearman ρ correlation.
Analysis across time of all of the above variables was conducted, evaluating differences of delta improvement (T6-T0 measures) by the Wilcoxon rank-sum test. An exception was the Family Strain Questionnaire short form pre- to post-assessment, for which we used the 2-sample test for proportions. Differences across time were considered significant for P < .05.
Results
Subjects and Caregivers
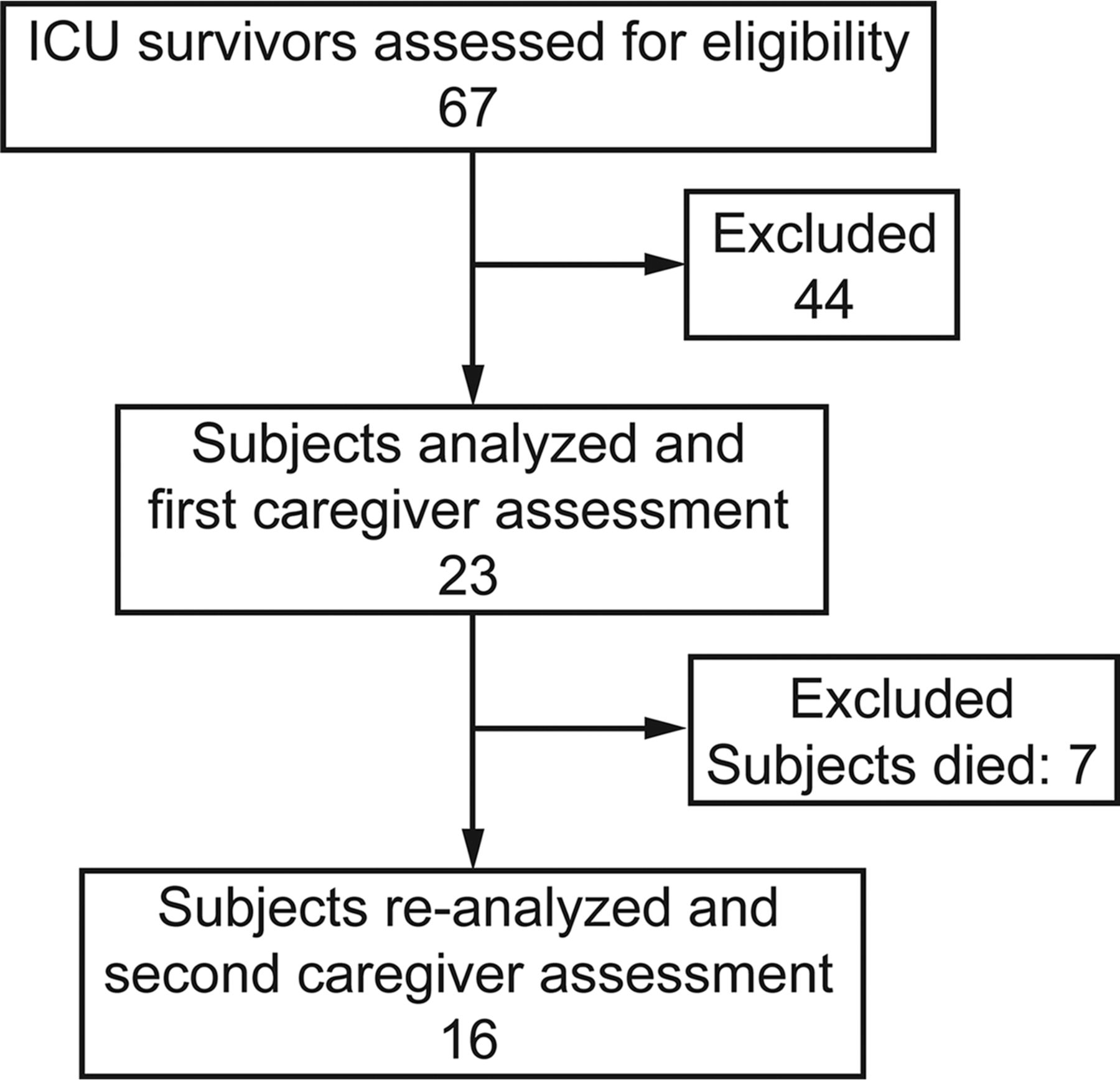
From April 15, 2011 to April 15, 2013, 23 subjects admitted to the rehabilitation center of the Salvatore Maugeri Foundation, Lumezzane, Brescia, Italy were eligible for the study (Fig. 1). Table 2 shows the demographic and clinical characteristics of subjects at discharge from the rehabilitation center. These long-stay ICU survivors were a heterogeneous group including a high percentage of neurological subjects, clinically compromised, presenting high comorbidities and disability and low effort tolerance capacity.
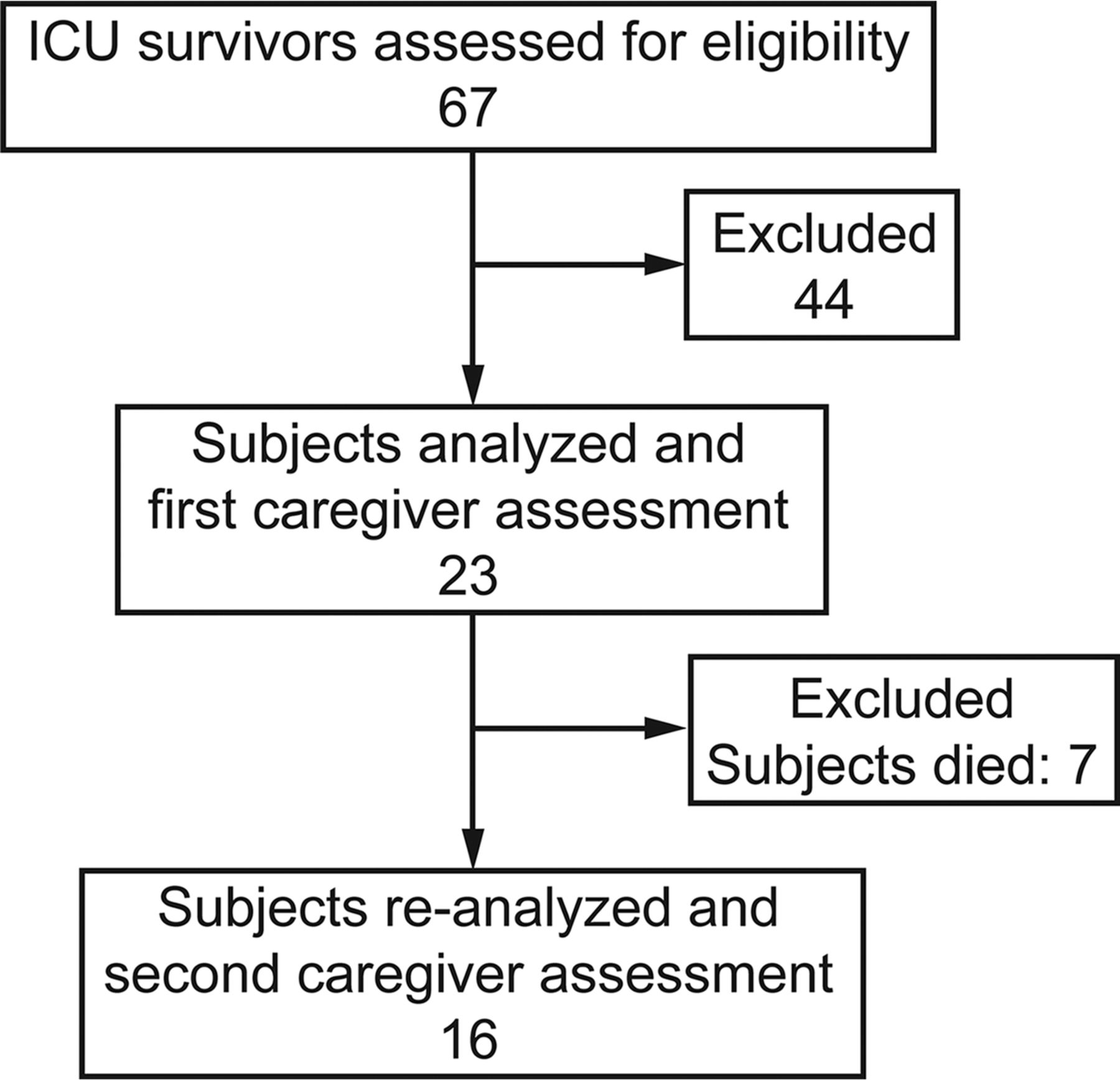
Flow chart.
Characteristics and Outcomes of Prolonged-ICU-Stay Survivors and Their Caregivers at Baseline (T0)
The socio-demographic characteristics of the caregivers of long-stay ICU survivors are described in Table 2. In general, caregivers were female (70%), 56 y old, and either the spouse (61%) or son/daughter (39%) of the subject.
Evaluation of Subjects and Caregivers at T0
At T0, the subjects showed a compromised HRQOL and a moderate impairment in perceived self-efficacy (General Perceived Self-Efficacy Scale) if compared with the best values of each test. Only EQ-5D was strongly correlated to clinical and disability outcomes (Fig. 2). HADS scores were in the normal range both for anxiety and depression (Table 2) and correlated with clinical outcomes (supplementary Table 2); however, 30% of the subjects showed anxiety, and 13% of subjects showed depression in a critical range.

Strong correlations (ρ > 0.5) between subjects' health-related quality of life (evaluated by EuroQol 5D index [EQ-5Dindex]) and clinical, respiratory function, effort tolerance, and disability outcomes. All evaluations were performed at discharge from the hospital following rehabilitation in 23 subjects. DNS = Dependence Nursing Scale; PImax = maximum inspiratory pressure; 6MWD = 6-min walk test distance.
At T0, 69% of caregivers were in the high risk area (ie, strongly recommended for an intervention by the psychologist; Table 2). Caregiver's strain score (Family Strain Questionnaire short form) was high and significantly related to the subject's clinical and HRQOL outcomes (Fig. 3) and to the caregiver's needs (ρ = 0.56, P < .01). The Caregiver Needs Assessment score was moderate (Table 2), being the highest-scoring for items belonging to the subarea related to information needs. In particular, the caregiver perceived a need for: information about what he/she was going to do for the subject, involvement in care decisions, and collaboration and communication with health staff. The lowest-scoring items referred to the need for interaction with other family caregivers with a similar problem, psychological support, and discretion in communications from the health staff.
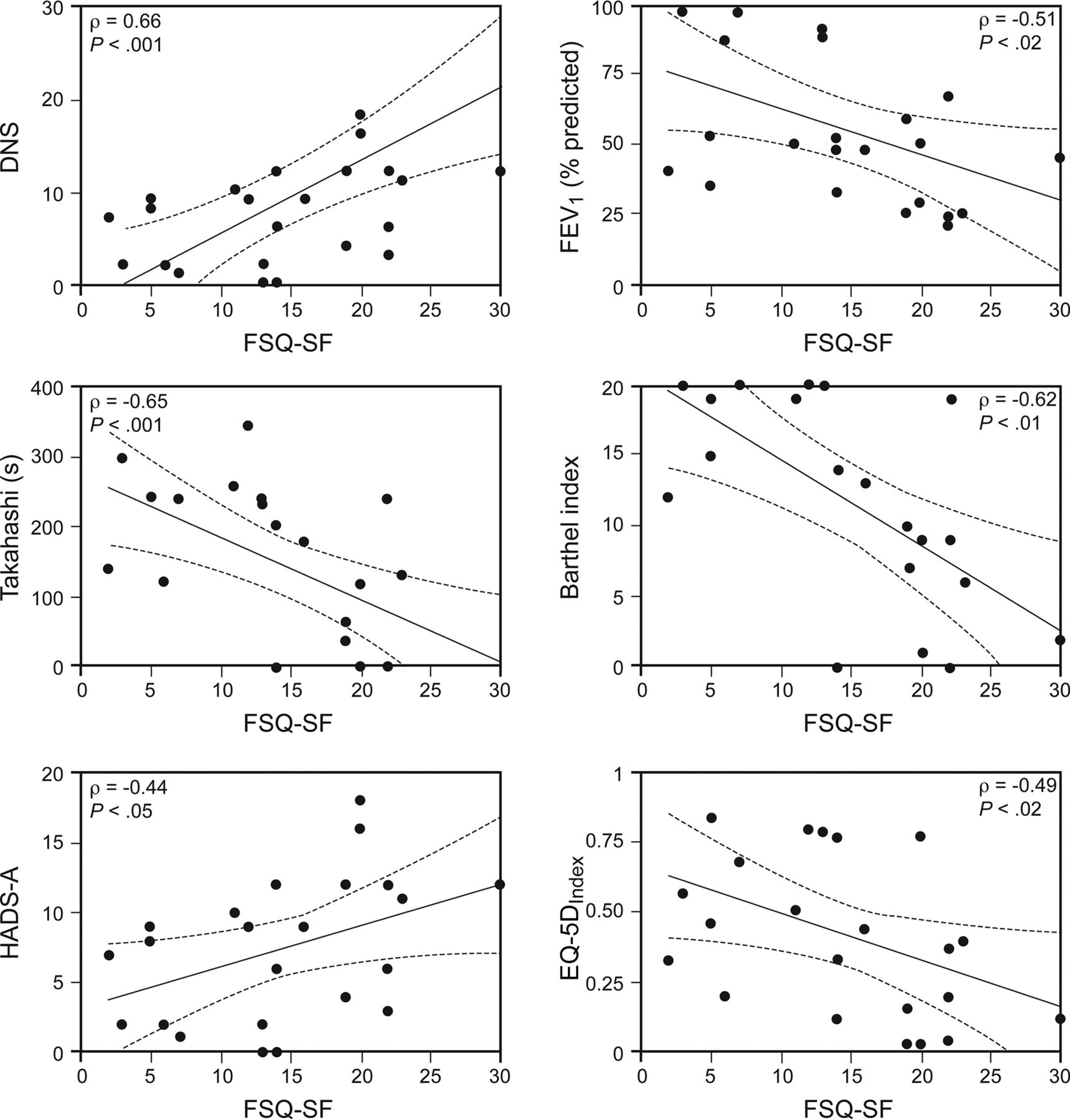
Correlation at hospital discharge between caregivers' strain (measured by the Family Strain Questionnaire [FSQ-SF]) and subjects' clinical, respiratory function, effort tolerance, and disability outcomes. All evaluations were performed at discharge from hospital following rehabilitation. DNS = Dependence Nursing Scale; HADS-A = hospital anxiety and depression scale (anxiety); EQ-5D = EuroQOL-5D.
Evaluation During the 6-Month Observation Period in Subjects and Caregivers
Subjects who died during the 6-month observation period had, at the time of hospital discharge (T0), clinical outcomes and HRQOL measurements similar to those of the subjects who completed the full 6-month follow-up (supplementary Table 3).
At T0, the majority of caregivers (86%) of subjects who died during the 6-month observation period had high strain and a higher need score (Caregiver Needs Assessment), although not statistically significant, than caregivers of subjects who completed the full 6-month follow-up (supplementary Table 3).
Evaluation of Subjects and Caregivers at T6
The 6-month follow-up (T6) was completed for 16 subjects and 16 caregivers, the relevant data of which are shown in Table 3. Long-stay ICU survivors mainly improved functional and disability outcomes and, in turn, their quality of life (Table 3).
Before to After Data on 16 Subjects Who Completed the 6-Month Follow-up Period and on Their Caregivers
At T6, caregivers' burden was similar to that observed at T0. However, observing how the caregivers had moved within the high risk area (Family Strain Questionnaire short form), we found that 50% of caregivers needed an urgent intervention, whereas for a further 12% of caregivers, it was simply recommended (Table 3).
Looking at specific items in the Caregiver Needs Assessment, a trend to a reduction in scores for caregiver-related needs was found for items such as the need to have information on the management of the disease, to communicate and interact with health-care staff, and to learn how to cope with the caring tasks. On the contrary, items that had been considered at T0 of less importance, such as the need for psychological support and discretion, tended to increase (for details, see supplementary Table 4).
Discussion
At the time of discharge from the in-hospital rehabilitation program, the HRQOL of subjects surviving a prolonged ICU stay was strongly related to their clinical, respiratory, and disability outcomes. A high percentage of their caregivers had a critical level of burden. Caregiver strain was related to the subject's outcomes and HRQOL. Six months after hospital discharge, although subjects' global condition had improved (in the absence of a structured program of rehabilitation), caregiver strain and caregiving-related needs remained unchanged, still high, and the percentage of caregivers needing urgent help/support tended to increase.
ICU survivors present a prolonged recovery trajectory,2 which depends on the patient's clinical6 respiratory,7 and HRQOL status.34 In contrast to other authors,8,35,36 we studied a heterogeneous subject population with concurrent comorbidities and high motor disability that had undergone a very long ICU stay and a long period of in-hospital rehabilitation.15 To our knowledge, this is the first study on ICU survivors with such a long stay correlating subjects' outcomes and HRQOL with caregivers' strain and needs. Moreover, the caregiver's strain and needs were tested with 2 questionnaires never used in caregivers of a long-stay ICU population.
In our study, the entry point both for subject and caregiver was the moment when the subject was deemed fit for discharge from the hospital by the physician after a period of rehabilitation; the end period of observation was 6 months after hospital discharge, to allow time for a longer recovery of the psycho-physical function in these very compromised subjects. Few studies, to our knowledge, have considered the impact of illness on perceived HRQOL in a mixed subject population in a similar setting to ours; either follow-up was 3 months after discharge,9 or a different instrument was used to evaluate HRQOL.34 Conversely, other studies36–38 used the EQ-5D but in very selected populations (ie, healthy elderly or COPD subjects) for a variable follow-up time from 6 to 24 months. Because each study used different outcome measures at different time points and in different settings, comparison with our study is difficult.
Changes in HRQOL after ICU discharge remain a controversial issue. Persisting disability and poor HRQOL have been documented up to 5 y after ICU discharge in survivors of ARDS.39,40
We evaluated quality of life using both the EQ-5D and McGill Quality of Life score. EQ-5D is a generic instrument recommended for the ICU setting.38,41 At hospital discharge, the EQ-5D has been reported to be one of the best predictive tools for full functional recovery at long-term follow-up in healthy elderly subjects surviving ICU.37 The median value for EQ-5Dindex in our study was 0.40, a value similar to that reported by Sacanella et al37 in elderly people who went on to survive 12 months after ICU discharge and lower than that reported by Berkius et al36 in a COPD-ICU population. Moreover, the EQ-5D visual analog scale we found was lower than in the study by Sacanella et al37 and similar to that reported by Berkius et al36 In our heterogeneous population, EQ-5Dindex was significantly correlated with clinical outcomes and, unlike in the study by Berkius et al,36 significantly improved 6 months after discharge. The EQ-5D visual analog scale also improved from 50 to 70, a level considered to indicate good health, but, in contrast to the results of Berkius et al,36 the increase was not statistically significant.
In our study, although in the absence of statistical significance, the McGill Quality of Life Score, including positive contributions to well-being, recovered over time. Our findings are in line with those reported by Cohen et al42 in subjects with terminal illness, where improvement in HRQOL went beyond symptom control following admission to a palliative care unit, and with findings from Roach et al43 in subjects with amyotrophic lateral sclerosis, suggesting that in subjects under critical conditions, life goals, hopes, and expectations are similarly independent from the diseases. In general, the current uncontrolled study confirms that long-stay ICU survivors tend to improve their HRQOL, as reported previously by other authors in compromised subjects with different pathologies.
The ICU survivor's life experience is transformative also for the family caregiver because the sudden onset of the illness allows no time to prepare for the practical and psychological demands involved. Therefore, caring for such complex cases may negatively affect caregiver burden, compromising the person's care in terms of the sustainability of providing care at home. It is reasonable to assume that caregiver burden of long ICU-stay survivors is high and increases during time. The current study considered the caregiver's strain and needs as conditions dependent on the subject's clinical and HRQOL outcomes observed in long-ICU-stay survivors discharged home after a long period of in-hospital rehabilitation.
At entry into the study, 69% of caregivers had high (43%) or very high (26%) strain, which was significantly related to the subject's level of anxiety, respiratory function, disability, and HRQOL. Our data confirm findings observed by Choi et al,44 who reported clinically important fatigue in 43% of caregivers of ICU survivors.
At follow-up, the percentage of caregivers in the high-risk subgroup was similar to that at entry, but the percentage in the very high-risk area (ie, recommended for an urgent psychological intervention) increased, although without statistical significance, >2.5-fold. This is consistent with data from others13,45,46 who have reported that clinical fatigue and needs involve family caregivers of ICU subjects and persist for a long time.
The importance of needs in family caregivers of ICU patients is well recognized in the literature, and several articles have explored the needs of the family in relation to subjects in the ICU.47 In the present study, Caregiver Needs Assessment scores at hospital discharge were similar to those reported by caregivers at entry and similar to those of caregivers of subjects with Alzheimer disease48 or amyotrophic lateral sclerosis.49 This finding suggests that caregivers of long-ICU stayers entered an adaptation phase after hospital discharge that is independent from the type of disease but probably related to the stage of the disease. Indeed, looking at caregivers' burden of subjects deceased before the 6-month follow up, needs scores were higher than those of caregivers at follow-up as reported by Nakken et al50 in a different caregiver population.
The Caregiver Needs Assessment questionnaire, developed to test the perceived needs related to assistance of family caregivers of subjects with a high level of disability, was used for the first time in this setting and was reliable. Caregiver Needs Assessment scores were unchanged over time, but the percentage of caregivers with needs increased, confirming that caregiving-related needs are a priority for family members.47
Limitations
Our single-center study and consequently small sample size raise potential questions about the degree to which the study participants are representative of the overall population of adults with a prolonged stay in the ICU, although from a purely demographic and clinical perspective, they appear quite typical. We used a questionnaire to screen strain (Family Strain Questionnaire short form) that does not provide any precise psychological diagnosis and the Caregiver Needs Assessment, which does not have a definitive cut-off score.
Clinical Implications
Looking at the subjects' clinical context, we should bear in mind that over a longer period of follow-up, an exacerbation could occur in subjects that would suddenly change the above-mentioned caregivers' picture, further influencing their burden. Prompt identification by the psychologist of caregivers with high strain and needs, at the moment of the patient's hospital discharge, could prevent their being left alone. The psychologist, informing the caregivers' family physician, could enable them to be referred to the psychologist for an appropriate individually tailored treatment.
Conclusions
The impact of critical illness is profound and long-lasting both for patients emerging from an ICU stay and for their caregivers. Despite the fact that subjects' functional autonomy and HRQOL were apparently good after 6 months, caregivers' burden remain high, suggesting the need to monitor/support them. Further studies are needed to explore benefits of a tailored psychological support dedicated to caregivers.
Acknowledgments
We thank Rosemary Allpress for the English revision of the manuscript and Francesco Grossetti for the statistical analysis.
Footnotes
- Correspondence: Laura Comini PhD, Fondazione Salvatore Maugeri, IRCCS, Direzione Sanitaria, Via Giuseppe Mazzini, 129, 25065 Lumezzane (BS), Italy. E-mail: laura.comini{at}fsm.it.
Supplementary material related to this paper is available at http://www.rcjournal.com.
This study was funded in part by an “Independent Research Grant 2010” (Decree 5685_May 2010, n. 475) from the Region of Lombardy, Italy. The authors have disclosed no conflicts of interest.
See the Related Editorial on Page 566
- Copyright © 2016 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}