

Abstract
BACKGROUND: Walking is part of obesity management. Assessment of ventilatory impairments and consequences for gait induced by obesity could be clinically helpful. We aimed to develop a method to accurately monitor ventilation with respiratory inductive plethysmography (RIP) in subjects with high body mass indices (BMIs) during a 6-min walk test (6MWT).
METHODS: 25 volunteers were divided into 2 groups based on BMI (<25 or >30 kg/m2) and performed a 6MWT with a calibrated RIP. Ventilatory parameters (tidal volume [VT], inspiratory [TI] and expiratory [TE] times, VT/TI ratio, and TI/Ttot ratio) were determined after processing RIP signals with a custom-made algorithm designed to discriminate tissue motion artifacts and respiratory cycles in the time domain. Six-min walk distance and average speed by minute were collected.
RESULTS: The number of artifacts removed by the algorithm used for artifact removal was higher for high-BMI subjects and was correlated to their individual values (r = 0.66, P < .001). Six-min walk distance was lower for the group with a higher BMI (P = .001). ANOVA revealed effects of exercise for VT, TI, and TE (P < .001) and also BMI effects in the course of the 6MWT for VT, TI, TE, VT/TI, and TI/Ttot (P < .001 for each of them).
CONCLUSIONS: This respiratory monitoring method is sufficiently sensitive to point out differences between rest and exercise as well as locomotor and ventilatory differences relative to BMI during the 6MWT. Thus, this system gives useful information from the 6MWT for clinicians who want to assess respiratory patterns of patients during this commonly used test.
- respiratory inductive plethysmography
- 6-min walk test
- tidal ventilation
- body mass index
- artifacts
- submaximal exercise
Introduction
There has been an increase in the number of overweight people in the general population of western countries. Body mass index (BMI), defined as the ratio of the body weight expressed in mass units (kg) over the square of body height in meters, is a widely accepted indicator of adiposity. Obesity, generally accepted as an increase of BMI beyond 30 kg/m2, is generally associated with a higher risk of health disabilities. Among disorders associated with obesity, impairments of lung function are well described at rest and during exercise.1–8 Even if obese subjects usually describe dyspnea when performing exercise, physical activity is recognized as an effective tool to limit comorbidities associated with obesity.9 Walking is currently recommended in the obese population as well as in the general population because it can provide a safe and effective lifestyle strategy to reduce abdominal obesity and metabolic marker abnormalities.10–14 In this context, developing a routine test to explore the impact of obesity-induced impairments of lung function on the ability to walk is essential.
The 6-min walk test (6MWT) used all over the world is a good candidate for evaluating submaximal exercise capacity, but the reference design is not able to give any data on respiratory patterns or limitations.15 Respiratory parameters can be measured by validated methods, such as by a pneumotachometer or metabolic device, but these methods require a mouthpiece or a face mask known to introduce biases on respiratory patterns.16,17 Respiratory inductive plethysmography (RIP) has been developed as an alternative technique to obtain ventilatory parameters avoiding these biases. Although this method has been validated by numerous studies,18–20 this is not the case when considering the obese population; Hollier et al21 reported some limitations, referring to an increased asynchrony and a propensity for generating artifacts in this population.
In this study, we propose an adapted method for using RIP to assess ventilation from subjects with low and high BMIs. The aim of the study was to determine whether the proposed RIP method during a 6MWT is able to describe ventilatory adaptations depending on BMI.
QUICK LOOK
Current knowledge
The 6-min walk test in its classical design gives useful information on functional capacity. However, ventilatory adaptations to peripheral oxygen demand increase during walking are not evaluated by this test.
What this paper contributes to our knowledge
This study reveals that the respiratory inductive plethysmography signal after calibration and filtering procedures can be used for monitoring ventilatory adaptations to exercise during a 6-min walk test without any biases. It allows the observation of different ventilatory behaviors, depending on body mass indices, which are compatible with what is known about ventilatory profiles and body mass index.
Methods
Subjects
The study was performed from January 2014 to June 2015 in the Service de Physiologie-Explorations Fonctionnelles, Hôpital Ambroise Paré AP-HP, Boulogne-Billancourt, France. Twenty-five healthy volunteers (6 men and 19 women) participated in this study and were divided into 2 groups depending on their BMI (Table 1). They provided their informed written consent, and the study was conducted in accordance with the principles of the Declaration of Helsinki. Approval for the study was obtained from the institutional review board of the French Learned Society for Respiratory Medicine “Société de Pneumologie de Langue Française” (2015-23).
Anthropometric and Spirometric Data
Recordings
A polygraph (NOX T3 sleep monitor, NoxMedical, Reykjavík, Iceland) usually used for sleep disorder diagnoses22 was used for several measurements. Subjects were equipped with a small nasal cannula and a thoracic belt connected to the polygraph.
6MWT
The 6MWT was performed in a 30-m route in a corridor according to recommendations from the American Thoracic Society.15 Average speed by minute was calculated from the walked distance determined by markers and walking time with a stopwatch. Data for activity were collected by using the 3-dimensional accelerometer included in the NOX T3 polygraph at a sampling frequency of 10 Hz and was used to synchronize signals by discriminating rest from walking.
Ventilatory Parameters
Nasal pressure and RIP signals were recorded with the polygraph NOX T3, allowing measurements of nasal pressure at a sampling frequency of 200 Hz, whereas thoracic RIP signal was recorded at a sampling frequency of 20 Hz. A pulmonary function test machine (Jaeger, Carefusion, Voisins-le-Bretonneux, France) measured FEV1 by integration of respiratory flow at the mouth measured with a calibrated pneumotachometer, whereas functional residual capacity was determined by helium dilution.23 Index for dyspnea and lower limb fatigue were assessed by mean of a modified Borg scale in centimeters with a precision of ± 1 cm before and after walking.24
Calibration
Before and after recordings of ventilation, calibration of RIP was carried out by simultaneously measuring volume change by a pneumotachometer and thoracic perimeter change by RIP while the subject was kept standing. Once the calibration maneuvers were initiated, the subjects were not allowed to change their standing posture and to reach the respiratory inductive plethysmograph with their hands. The relationship between perimeter changes measured by RIP and volume measured by the pneumotachometer was determined by a linear regression model. Slopes of these relationships were calculated offline to predict volume changes from perimeter changes between calibration maneuvers.
Protocol
Measurements were taken in a quiet, warm laboratory room. Determining the absence of obstructive or restrictive disorder by measuring FEV1, FVC, and functional residual capacity and calculating the FEV1/FVC ratio and total lung capacity was the preliminary phase of the protocol. Calibration maneuvers were performed before and after the 6MWT, and 1 min of standing at rest was inserted prior to the 6MWT.
Data Processing
Data Collection.
Data from RIP (nasal pressure, thoracic signal, and actimetry) were analyzed offline by extracting them in .edf format from the polygraph with the dedicated software NOXturnal 3.2 (Nox Medical, Reykjavík, Iceland). Data were then converted into ASCII format by EDFbrowser 1.52 (GNU general public license) in order to be imported into Matlab 2014b (The MathWorks, Natick, Massachusetts) for offline analysis.
Artifact Management.
Since motion artifacts can easily contaminate the RIP signal during walking, we used a custom-made algorithm with Matlab software designed in the time domain to remove them (unpublished data). Briefly, artifact removal by this algorithm consists of using nasal pressure signal as a time reference for identification of respiratory cycles on the thoracic signal. This temporal reference allows exclusion of artifacts by keeping only maximum and minimum values localized on ranges corresponding to respiratory cycles on the nasal signal. After artifact removal, ventilatory parameters (tidal volume [VT], inspiratory time [TI], expiratory time [TE], breathing frequency [f], TI/Ttot ratio, and VT/TI ratio) were calculated.
Statistics
Statistical analyses were performed by using GraphPad Prism 5.01 for Windows (GraphPad Software, San Diego California). Normality of data were first tested by using a D'Agostino and Pearson omnibus normality test.25 Because data were not normally distributed most of the time, correlations were evaluated by Spearman coefficient calculation. Comparisons between groups were evaluated using the Mann-Whitney test. Comparison of sex ratio was made by using a Fisher exact test.
Statistics during the 6MWT were performed with a 2-way ANOVA and the Sidak multiple-comparison test. Effects evaluated were BMI and time during the 6MWT. It is noteworthy that for evaluating these effects, the rest period (t = 0 min) was excluded. Two-way ANOVA with the Sidak multiple-comparison test was also performed to evaluate the effect of activity (between rest and the first 1 min) on VT, f, TI, and TE. Size effects were estimated with the Cohen equation, where the first term was (MBMI > 30 − MBMI < 25)/σ pooled, with MBMI > 30 the mean of the high-BMI group, MBMI < 25 the mean of the low-BMI group, and σ pooled the average population SD.26 Size of exercise effects was calculated with the same equation with the first term as (MT6 − MT0)/σ pooled, with MT6 the mean of the parameter at the last minute of the 6MWT and MT0 the mean of the parameters at rest. Sizes of the time effect during the 6MWT were calculated with (MTi − MTj)/σ pooled with i and j in a range from 1 to 6. Every pairing of i,j possible was assessed, and results were given by means and SD values of all calculations. The strength of the size effect could be interpreted according to the Cohen guidelines (≤0.4, small; 0.41–0.7, moderate; >0.7, strong).
Results
As shown in Table 1, there was no significant difference between the group with higher BMIs and the group with lower BMIs for age and height. BMI comparison established a highly significant reduction of functional residual capacity from groups with higher BMIs in comparison with groups with low BMIs (P < .001; effect size = −1.64 [strong]).
Six-min walk distance in the group with higher BMIs was significantly lower compared with the lower-BMI group (P = .001; effect size = −1.22 [strong]) (Table 2), which is in accordance with the effect of BMI from 2-way ANOVA (P < .001; effect size = −1.21 [strong]) considering walking speed (Table 3). Multiple comparisons show significant differences for walking speed between the higher-BMI group and the lower-BMI group for each minute of the 6MWT (P = .004, .003, .003, .003, .003, .005; effect size = −1.23, −1.18, −1.23, −1.23, −1.27, and −1.15 [all strong] from the first to the last minute) (Fig. 1). Results from the subjective data showed a significant increase of dyspnea and fatigue (P = .001; effect size = 1.23 [strong] and P = .049; effect size = 0.87 [strong]), respectively) for the higher-BMI group in comparison with lower-BMI subjects (Table 2).
Data From Walking Test
Time and Body Mass Index Effects of Recorded Parameters During the 6-Min Walk Test
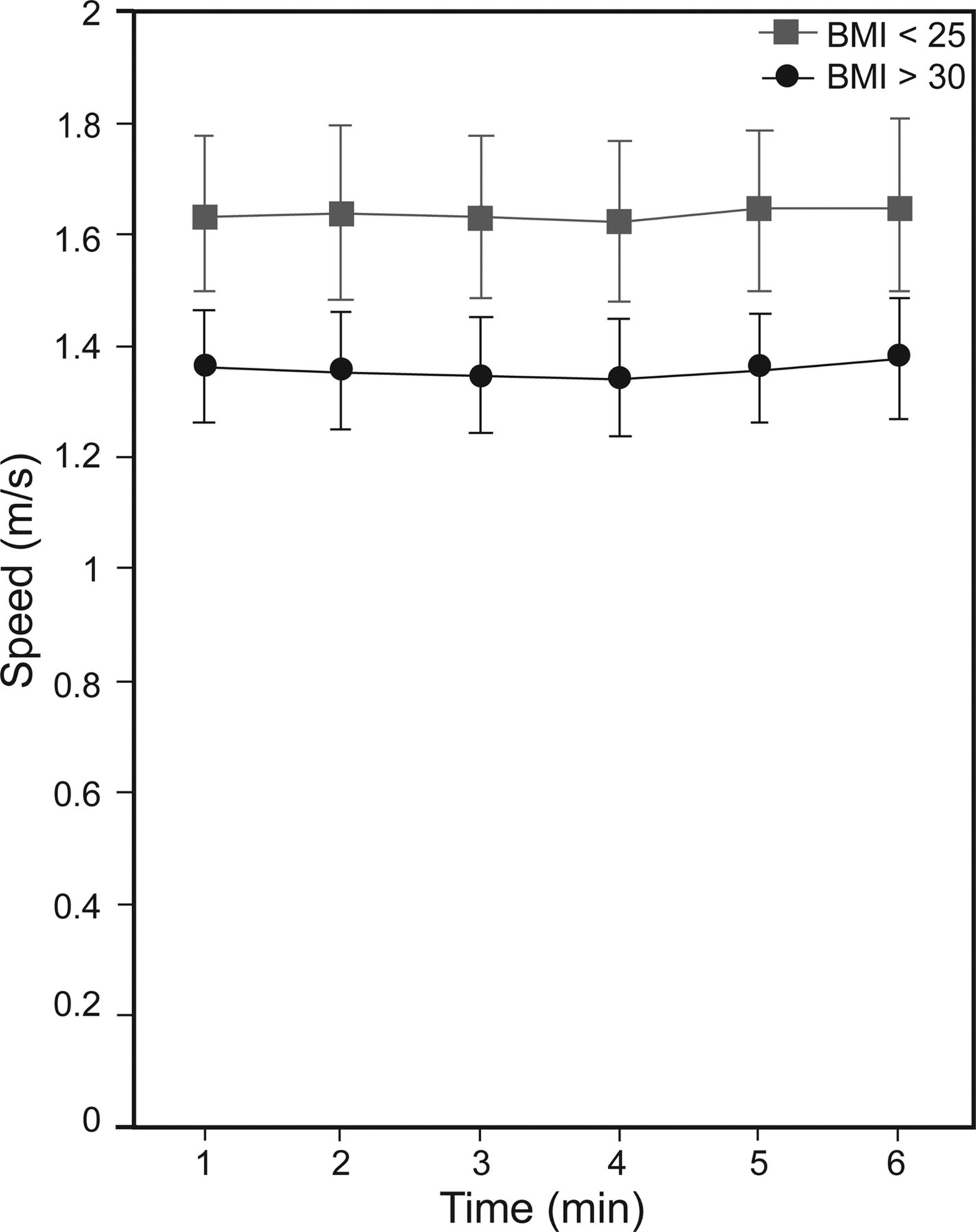
Average speed during the 6-min walk test. P < .01 between groups for all points. Data are shown as mean and 95% CI.
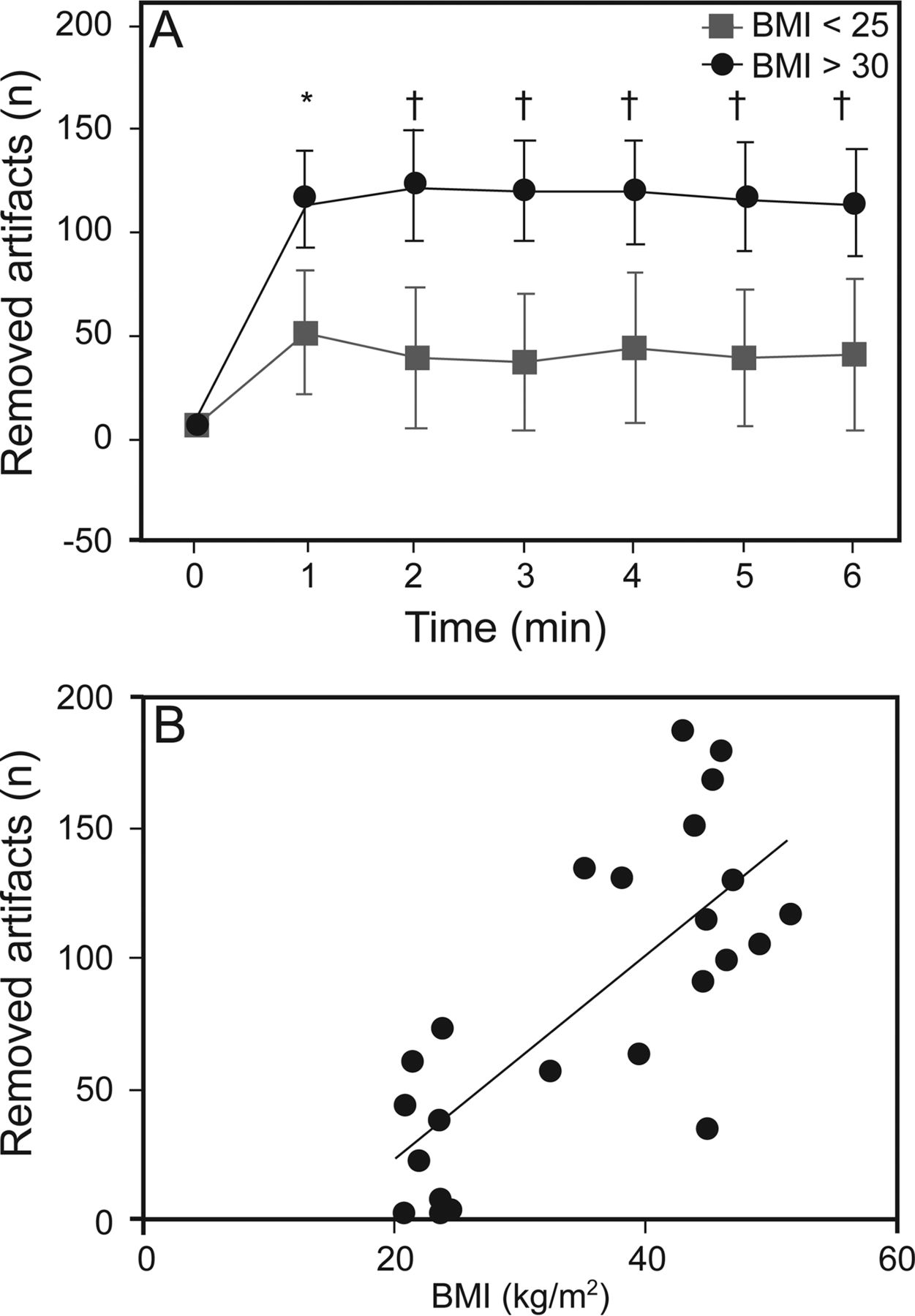
From a methodological point of view, 2-way ANOVA showed a BMI effect (P < .001; effect size = 1.07 [strong]), considering the number of artifacts removed by our custom-made algorithm (Table 3). In addition, we found a significant correlation between the number of artifacts removed and BMI individual values (r = 0.66 P < .001) (Fig. 3).
Two-way ANOVA revealed effects of exercise for VT, f, TI, and TE (P < .001 for each of them; effect size = 1.18, 1.54, −0.7 and −0.9, respectively [all strong]). The walking effect explained 10.8% of variation of VT, 45.4% of variation of f, 5.6% of variation of TI, and 11.1% of variation of TE. The effect of BMI explained 7% of variation of VT and did not explain variation of f, TI, and TE.
During the 6MWT, 2-way ANOVA revealed time effects (P < .001) for VT, TI, and TE (effect size = 0.2 ± 0.22, −0.13 ± 0.09, and −0.13 ± 0.08, respectively [all small]), whereas a BMI effect was found for VT (P < .001; effect size = 0.60 [moderate]), f (P = .003; effect size = 0.36 [small]), TI (P < .001; effect size = −0.16 [small]), and TE (P < .001; effect size = −0.25 [small]) (Table 3). Multiple comparisons showed highly significant (P < .001; effect size = 0.83, 0.62, 0.64, 0.68, 0.56, and 0.66 [all strong] from the first to the last minute) minute-by-minute rise of VT from higher-BMI subjects in comparison with lower-BMI subjects at each minute of the 6MWT (Fig. 4). Minute-by-minute comparisons of TI between the higher-BMI group and lower-BMI group showed at the third and fourth minute significant diminution of TI from the higher BMI value (P < .001; effect size = −0.40 (small) and P = .009; effect size = −0.28 (small), respectively). The same comparison for TE revealed a significant decrease for subjects with higher BMIs from the second minute up to the last one (P < .001; effect size = −0.38, −0.41, −0.31, −0.43, and −0.34 [almost all small] from the second to the last minute).
Two-way ANOVA revealed time effects for VT/TI ratio (P < .001) and showed BMI effects for TI/Ttot ratio and VT/TI ratio (P < .001; effect size = 0.14 [small] and 0.72 [moderate], respectively) during the 6MWT (Table 3). Multiple comparisons show significant minute-by-minute rise of TI/Ttot ratio from subjects with higher BMIs at the fifth minute of the 6MWT (P = .008; effect size = 0.28 [small]). VT/TI ratio values from higher-BMI subjects were significantly higher (P < .001; effect size = 0.90, 0.80, 0.85, 0.81, 0.73, and 0.76 [all strong] from the first to the last minute) than those from lower-BMI subjects, from the onset of the 6MWT to its end (Fig. 2). Moreover, significant correlation (r = 0.61, P = .002) was found when considering the relationship between BMI individual values and corresponding VT/TI ratio values (Fig. 2), whereas there was no correlation between VT/TI and speed or 6-min walk distance.

A: Comparison between groups relying on body mass index (BMI) of inspiratory time/total time (TI/Ttot) ratio during the 6-min walk test. B: Comparison between groups relying on body mass index of tidal volume/inspiratory time (VT/TI) ratio during the 6-min walk test. C: Relationship between tidal volume/inspiratory time ratio at the last minute of the 6-min walk test and body mass index. Data are represented as mean and 95% CI. * P = .008; † P < .001.
Discussion
Use of RIP in Populations With High BMI
The use of our custom-made algorithm (unpublished data) for artifact removal appears to be useful when considering the relationship between the number of artifacts removed by the algorithm and BMI (Fig. 3). This is compatible with the relationship described by Hollier et al21 of SD from VT error with waist circumference. This could be explained by a strong link between artifact genesis and overriding fat tissue, which can increase the probability of contaminating the signal when obese subjects are walking. Thus, our algorithm seems to fulfill the need for filtering the RIP signal of people with high BMIs during walking and increases the accuracy of ventilatory parameter measurements.

A: Comparison between groups relying on body mass index (BMI) for number of removed artifacts by custom-made algorithm during the 6-min walk test. * P = .005; † P < .001. Data are represented as mean and 95% CI. B: Relationship between the mean number of removed artifacts during the 6-min walk test and body mass index.

Comparison between groups relying on body mass index (BMI) during the 6-min walk test. A: Tidal volume (VT). B: breathing frequency. C: inspiratory time (TI). D: expiratory time (TE). * P = .009; † P < .001. Data are represented as mean and 95% CI.
To our knowledge, there are few data regarding the use of RIP in obese subjects. Hollier et al21 studied the validity of RIP in subjects with obesity hypoventilation syndrome but without any filtering method. This study raises some limitations to the use of RIP for obese people. First, they find good agreement for f in controls but not for OHS, suggesting the inefficiency for detecting onset and end of respiratory cycles when a high BMI is involved. This is compatible with a treatment of RIP without artifact removal, unlike in this study. Indeed, in our study, the use of nasal pressure signal to determine f seems much better than RIP alone. Previous authors also indicated that RIP belt slippage can easily invalidate assumptions made in the calibration phase. In our study, we chose to limit this issue by flanking measurement time by 2 calibration phases to minimize the possible effect of belt displacements and/or drift of calibration. Furthermore, a high level of respiratory load characteristic of obesity is compatible with a high level of asynchrony frequently occurring and leading to inaccuracy when a linear model is used. To avoid this phenomenon, and because nonlinear calibration is not commercially available, we decided to exclusively consider the thoracic belt, ignoring abdominal motions and thoracoabdominal asynchrony issues. Hollier et al21 also noted that deformity of adipose tissue of the belly could attenuate movement detection and lead to an underestimation of calculated VT. Following this, our significant difference between groups would have been higher if tidal volumes were truly underestimated for the higher-BMI group. However, by applying our method, the level of VT for higher-BMI subjects at the end of the 6MWT was very close to the range described previously in obese subjects by Di Thommazo-Luporini et al27 (1.4 ± 0.2 L with FVC = 3.4 ± 0.6 L vs 1.4 ± 0.6 L with FVC = 3.8 ± 0.6 L in our study). In the same view, exercise-induced evolution of ventilatory parameters calculated with this method are in accordance with well-known increased respiratory rate and tidal volume during exercise.28 This method seems sensitive enough to allow the observation of a ventilation rise during walking, which can be appreciated by time effects observed in this study.
Ventilatory and Locomotor Adaptation of High-BMI Subjects
Exercise dyspnea is very common in the obese population.29 Results from our study were significant with higher Borg scores of dyspnea at the end of the 6MWT. Despite the fact that the Borg score is a subjective index of dyspnea, it highlights the feeling of discomfort in high-BMI subjects when performing submaximal activities like walking for 6 min at a natural speed. As more objective indices, ventilatory parameters are shown to be significantly higher in high-BMI subjects (VT and f), demonstrating an increase in minute ventilation. The higher f values in high-BMI subjects may be explained by significant reduction of TI and a more significant diminution of TE, leading to a significant reduction of respiratory cycle duration. It is likely that they recruit expiratory muscles to increase minute ventilation around or beyond the 40 L/min threshold as reported earlier.30,31 In the same view, the transition from rest to activity was affected by BMI, with a steeper increase of VT at the first 2 min of the test. The good correlation between VT/TI at the end of the 6MWT and BMI is in accordance with the increased neural drive in obese subjects reported by Babb.32 Nevertheless, the difference between groups for TI/Ttot ratio is less marked and could be mainly explained by the greater shortening of TE than of TI in higher-BMI subjects. These results suggest a stronger stimulation of respiratory centers for people with high BMIs during walking.
Conclusion
Our study demonstrates that respiratory monitoring during 6MWT is able to detect the repercussions of high BMI values over ventilatory adaptation to submaximal exercise. Our results suggest that 6MWT is sufficiently stressful to point out significantly different breathing and locomotor patterns. The use of RIP during walking could be useful to investigate respiratory consequences of lung disorders among various subjects, including obese people.
Footnotes
- Correspondence: Yann Retory MSc, Service de Physiologie-Explorations Fonctionnelles, Hôpital Ambroise Paré AP-HP, 9, Avenue Charles de Gaulle, 92100 Boulogne Cedex, France. E-mail: yann.retory{at}aphp.fr.
This work was supported by funding from the Fonds de Dotation de Recherche en Santé Respiratoire and LVL Medical. The authors have disclosed no conflicts of interest.
- Copyright © 2016 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}
{kind=link}