

Abstract
BACKGROUND: Advancements in tracheostomy tube design now provide clinicians with a range of options to facilitate communication for individuals receiving ventilator assistance through a cuffed tube. Little is known about the impact of these modern design features on resistance to air flow.
METHODS: We undertook a bench model test to measure pressure-flow characteristics and resistance of a range of tubes of similar outer diameter, including those enabling subglottic suction and speech. A constant inspiratory ± expiratory air flow was generated at increasing flows up to 150 L/min through each tube (with or without optional, mandatory, or interchangeable inner cannula). Driving pressures were measured, and resistance was calculated (cm H2O/L/s).
RESULTS: Pressures changed with increasing flow (P < .001) and tube type (P < .001), with differing patterns of pressure change according to the type of tube (P < .001) and direction of air flow. The single-lumen reference tube encountered the lowest inspiratory and expiratory pressures compared with all double-lumen tubes (P < .001); placement of an optional inner cannula increased bidirectional tube resistance by a factor of 3. For a tube with interchangeable inner cannulas, the type of cannula altered pressure and resistance differently (P < .001); the speech cannula in particular amplified pressure-flow changes and increased tube resistance by more than a factor of 4.
CONCLUSIONS: Tracheostomy tube type and inner cannula selection imposed differing pressures and resistance to air flow during inspiration and expiration. These differences may be important when selecting airway equipment or when setting parameters for monitoring, particularly for patients receiving supported ventilation or during the weaning process.
Introduction
The work of breathing is the sum of elastic and resistive work; in addition to patient factors, apparatus, such as the ventilator, breathing circuit, and endotracheal or tracheostomy tube, can contribute to added work through altered airway resistance.1–3 Normal upper airway resistance accounts for approximately half of the total airway resistance,4,5 which is typically 2–5 cm H2O/L/s.4,6 Because the tracheostomy tube essentially replaces the upper airway, it has been suggested that tube resistance should ideally not exceed 1–2.5 cm H2O/L/s.4,7,8 However, the extent to which a tracheostomy tube creates resistance depends on its characteristics (diameter [including contrasting diameter of inner and outer cannulas], length, curvature, and materials used)3,7,9 as well as the rate and type of air flow delivered.7,10
Existing research on tracheostomy tube resistance has been limited to old models3,7,11 or tubes of a single manufacturer,7,9,12 or it has examined only inspiratory flows.9,12 Further, published data only relate to conventional tubes3,7,9,11,12 and not those enabling above cuff suction and/or speech. Tracheostomy tubes with subglottic suctioning lines were designed to allow removal of upper airway secretions and reduce the risk of ventilator-associated pneumonia.13 The external suction line may also be used to deliver air through the upper airway (including vocal cords) for speech14 (Fig. 1) while the lower airways remain isolated for ventilation. These tubes may come with an optional or mandatory inner cannula. An alternative and newer device is a fenestrated cuffed tracheostomy tube, into which one of 3 interchangeable cannulas can be inserted to enable different functions.15,16 The fenestration is utilized for speech through placement of a flexible tapered cannula with a distal flap valve to redirect expired air through the upper airway (Fig. 2, A and B), whereas the fenestration is closed upon insertion of a cannula with an internally embedded subglottic suctioning line (Fig. 2C) or a rigid standard cannula (Fig. 2D).

Speech via subglottic suctioning tracheostomy tube. Gas passes through the subglottic suctioning line into the upper airway for speech (dashed line); lower airways remain isolated for mechanical ventilation (solid line).

A: Speech via placement of speech cannula, with expiratory air flow redirected through the upper airway; air flow with interchangeable inner cannulae. B: Speech cannula. Inspiratory airflow from ventilator passes through tapered cannula with flap valve to lungs; expired air passes above a collapsible segment of the inner cannula and exits through the fenestration. C: Subglottic suction cannula with inner embedding of the suction line and closed fenestration. D: Standard cannula with closed fenestration.
It is possible that special design features of modern tracheostomy tubes (such as optional or interchangeable cannulae with varying inner dimensions) may alter pressure-flow patterns and resistance to air flow differently. This could be an important clinical consideration when providing mechanical ventilation and during the subsequent weaning process. Hence, the aims of this study were to establish the impact of inner cannula selection on inspiratory and expiratory pressures and resistance to air flow through a range of modern tracheostomy tubes.
QUICK LOOK
Current knowledge
In recent years, bench model investigations of air flow through standard tracheostomy tubes have reported increased resistance following insertion of an inner cannula. Modern tracheostomy tubes have special design features enabling subglottic suction and/or speech; these can have optional, mandatory, and/or interchangeable inner cannulas of varying dimension.
What this paper contributes to our knowledge
In a bench model study of pressure-flow patterns and resistance through a range of modern tracheostomy tubes, differing impacts on air flow dynamics were observed between tubes. Our findings confirmed an increase in pressure and resistance with insertion of an inner cannula and showed differences during inspiratory and expiratory flows according to the type of tracheostomy tube and inner cannula inserted.
Methods
We selected double-lumen cuffed tracheostomy tubes to represent standard design (Shiley LPC [Covidien Australia, Lane Cove, Australia]; Portex Blueline Ultra [BLU] [Smiths Medical Australasia Pty Ltd, Bella Vista, Australia]), subglottic suction design (Shiley Evac; Portex BLU Suctionaid), and a model with a speech cannula option in addition to standard and subglottic suction cannulae (Blom Pulmodyne, Indianapolis, Indiana). All tubes were size 8 but matched as closely as possible on outer diameter (Table 1). Additional testing of size 6 comparable tubes (see supplementary Table 1 at http://www.rcjournal.com) was also conducted and is reported in the supplemental material. Of note, the Portex tubes can also function as single-lumen without the optional inner cannula. All tubes were new and solely used for the purpose of the study. Ethical approval was not required for this bench model investigation.
Size 8 Tracheostomy Tube Specifications
Pressure-flow characteristics were studied for each tracheostomy using an in vitro model (Fig. 3). Constant air flows were generated by a device designed for flow calibration (18987-1, Gould Godard VB, Bilthoven, The Netherlands), capable of producing 0–300 L/min. Target flows of 0, 10, 20, 30, 40, 50, 60, 70, 80, 100, and 150 L/min were generated and confirmed with a calibrated Fleisch type pneumotachograph (HP-47034A, Hewlett-Packard, Palo Alto, California) and transducer. We chose this method because resistance was expected to be non-linear due to the presence of both laminar and turbulent air flow, and this method allows the simple presentation of resistance at a particular flow, which in turn allows flexibility in understanding the specific effect at different and varying flows. Pressure was measured with an air-filled differential pressure transducer (Bell and Howell 4-327-I, Trans-America Delaval, Pasadena, California). Constant pressure and flow data were recorded on an analog monitor (Hewlett Packard 78324A) connected to a personal computer via a 12-bit analog to digital converter (DT801, Data Translation, Marlboro, Massachusetts) at 100 Hz with waveform analysis software (ANADAT 5.2, RHT-InfoDAT, Montreal, California).

Apparatus setup for inspiratory testing.
Inspiratory data were collected as illustrated (Fig. 3), with tube orientation reversed for expiratory data and cuff pressures maintained at 25 mm Hg to ensure an adequate seal against the pressure transducer. Prior testing of the system confirmed no Venturi effect. Expiratory testing was only performed on the size 8 tubes capable of being used for speech production (Shiley Evac, Portex BLU-Suctionaid, Blom). Immediately before each expiratory measurement from the Blom speech cannula, a separate high-flow compressed air source (30 L/min) was used to ensure reinflation of the collapsible inner segment and simulate a normal respiratory cycle.
For analysis, inspiratory and expiratory data for each tube were plotted as flow (L/min) versus pressure (cm H2O) up to 150 L/min. Pressures between 0 and 80 L/min were compared across tubes using repeated measures analysis of variance with post hoc Tukey honest significant difference test tests (IBM SPSS 21.0 for Windows, IBM Corp, Armonk, New York) with significance at P < .05. Flows between 40 and 60 L/min are highlighted, given their clinical relevance,17,18 with pressures at these flows converted to resistance in cm H2O/L/s. Measurement reproducibility was tested for the size 8 tube range using a one-way analysis of variance to calculate technical error of measurement.19 Recorded flows were within 3.5% of the target rates, and our testing of above cuff suction and speech tubes was reproducible within a 2% technical error of measurement.
Results
For all inspiratory and expiratory comparisons, there was an increase in pressure with increasing flow (P < .001), a difference in pressure according to the type of tube (P < .001), and a difference in the pattern of pressure change with increasing flow according to the type of tube (P < .001).
Impact of Optional Inner Cannula
Tubes without inner cannula had the largest inner diameter (Table 1), and as expected, the pressures through the Portex BLU and/or Portex BLU-Suctionaid as a single-lumen tube were lower than all double-lumen tubes during inspiration (P < .001) (Fig. 4) and expiration (P < .001) (Fig. 5).

Pressures through size 8 tracheostomy tubes at increasing inspiratory flow. Clinically relevant flows are highlighted with gray shading. Pressures for the Portex BLU and Shiley LPC are not shown because they were nearly identical to those of the Portex BLU Suctionaid and Shiley Evac, respectively.

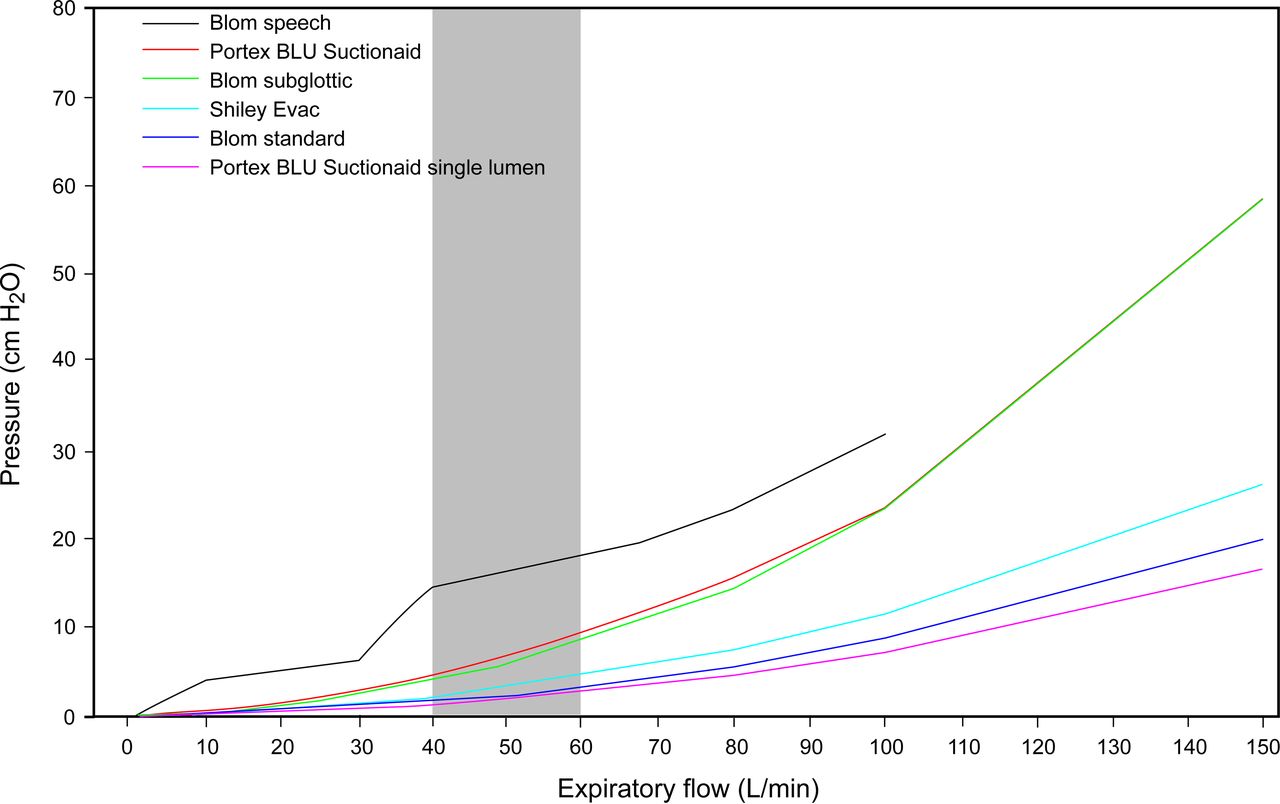
Pressures through size 8 tracheostomy tubes at increasing expiratory flows. Clinically relevant flows are highlighted with gray shading. Flows above 100 L/min could not be generated for the Blom speech cannula.
Pressures During Inspiratory Flow
Inspiratory pressures against increasing flows are shown in Figure 4, with clinically relevant pressures between 40 and 60 L/min highlighted. The Blom standard cannula and Shiley Evac generated equal lowest inspiratory pressures of all double-lumen tubes (P < .001); pressures increased with the Blom subglottic suction cannula (P < .001) and Portex BLU Suctionaid (P < .001), respectively. The Blom speech cannula generated the highest pressures (P < .001).
Pressures During Expiratory Flow
Expiratory pressures against increasing flows for the 3 tubes capable of being used in speech production are shown in Figure 5. The Shiley Evac generated the lowest expiratory pressures of all double-lumen tubes (P < .001), followed by the Blom standard cannula (P < .001). Pressures increased with the Blom subglottic suction cannula (P < .001) and Portex BLU Suctionaid (P < .001), respectively. The Blom speech cannula generated the highest pressures (P < .001).
Impact of Interchangeable Inner Cannulas
Pressure variation between the 3 interchangeable cannulas of the Blom was observed during inspiratory (Fig. 4) and expiratory flows (Fig. 5); in both directions, the speech cannula had higher pressures than the subglottic suction cannula (P < .001), which had higher pressures than the standard cannula (P < .001).
Bidirectional Pressures
Pressure-flow patterns varied with air flow direction between the different tube types. Within the Blom standard cannula and Portex BLU-Suctionaid (double- and single-lumen) there was no difference in pressures encountered during inspiratory or expiratory flows. Inspiratory pressures through the Shiley Evac and Blom speech cannula were greater than expiratory (P < .001), yet expiratory pressures were greater than inspiratory with the Blom subglottic suction cannula (P < .001).
Resistance
Inspiratory and expiratory pressures for the 3 tubes enabling speech (converted to resistance at 40–60 L/min) are shown in Table 2. During both inspiratory and expiratory flows, tube resistance increased by a factor of 3 upon insertion of the optional inner cannula in the Portex BLU-Suctionaid (compared with the same tube as single-lumen). Changing from the Blom standard cannula to the Blom speech cannula increased tube resistance by a factor of 4 at 60 L/min, a factor of 5 at 50 L/min, and a factor of 6 at 40 L/min. Similar patterns of pressure versus inspiratory flow were observed across all smaller size 6 and/or size 7 tubes examined but with markedly increased pressures and resistance noted (supplementary Table 2 and supplementary Fig. 1).
Inspiratory and Expiratory Resistance Associated With Clinically Relevant Flow Rates Through Size 8 Tracheostomy Tubes
Discussion
Since a primary aim of a tracheostomy is to reduce air flow resistance and work of breathing for patients weaning from mechanical ventilation,3 any increase in pressure and resistance imposed by the tube is an important clinical consideration when selecting airway equipment for vulnerable patients.10,12 All tracheostomy tubes caused greater resistance to air flow than a native upper airway in this study, but importantly, the imposed resistance was high in the majority of double-lumen tubes at clinically relevant flows. Although the clinical impact of changes in tube resistance cannot be directly determined from this bench model analysis, it can be theorized that the greater the inspiratory resistance through the tube, the greater the inspiratory effort required by the patient to overcome this resistance during a spontaneous or supported breath. Greater expiratory effort may result in gas trapping and difficulty initiating the next breath if recruitment of expiratory muscle force is inadequate. Our findings support our hypothesis that special design features of modern tracheostomy tubes can have differing impacts on air flow dynamics. It is likely that these findings have clinical importance for patients weaning from mechanical ventilation and breathing spontaneously through the types of tracheostomy tubes investigated.
Earlier studies have reported an increase in pressure and resistance with a decrease in tube diameter3,7,9,12; we confirmed a 3-fold increase in resistance with placement of an inner cannula in a tube that can function as either single- or double-lumen. This is marginally higher than reported previously.9,12 The largest inner aperture of tubes used in our study was 8 mm, and earlier models have shown that tube resistance does not drop below normal airway resistance until the inner diameter is 8.5–9.4 mm.20 Our tube choice, however, was based on the clinical predominance of the size 8 tube in the participating hospital and other published research.12,21,22 Placement of an inner cannula to reduce the risk of tube occlusion (by allowing removal for cleaning)3,23 markedly increased resistance to air flow. It could be argued that the optional inner cannula created unacceptable resistance when comparing it with a native airway. Conversely, the impact of retained secretions within a tracheostomy tube on resistance to air flow was not measured or discounted.
A novel finding was the marked variation in patterns of pressure against flow according to the type of inner cannula in situ across brands and functions. For 2 brands (Shiley and Portex), 2 commercial uses were possible within the one structure: (1) removal of subglottic secretions and (2) delivery of air above the cuff for speech. The mechanism/tubing enabling these functions was externally attached to the outer cannula; hence, air passage through the tracheostomy was not altered by changing the use or function of the tube (Fig. 1).
The other brand (Blom) had 3 commercial uses (standard, subglottic suctioning, and speech) within the one outer structure; however, the mechanisms enabling each function (insertion of a standard, subglottic suction or speech cannula) altered the dimensions of the inner aperture for respiration. When acting as a standard tube, the inspiratory resistance was equal to the lowest of all double-lumen tubes, but it increased by 70% upon changing to the subglottic suction cannula and by >400% when changing to the speech cannula. The speech cannula created high resistance even at lower flows, probably reflecting greater amounts of turbulent flow. Differing dimensions of the interchangeable inner cannula are therefore reflected: with the mechanism enabling removal of subglottic secretions embedded into the inner cannula (reducing proximal aperture) (Fig. 2C) and the tapered speech cannula with flap valve creating a narrowing at the distal end of the tube (Fig. 2B). In a patient receiving controlled mandatory ventilation, the added inspiratory resistance is probably of little concern; however, in the partially supported or weaning patient, the additional inspiratory work may be important.
Previous research suggests that adult tracheostomy tubes encounter greater pressures during inspiration than during expiration3 due to the angle of tube curvature, yet interestingly, this pattern was observed for only one brand in our study (Shiley). Regardless of inner cannula presence or absence, the Portex tubes had equal pressures during inspiration and expiration. The Blom was unique in that each inner cannula selection from a choice of 3 altered the pressures of bidirectional air flow differently. This included a novel finding of greater pressure and resistance during expiration than during inspiration with the subglottic suctioning cannula in situ, probably reflecting the internal embedding of the suction port.
Although few studies have explored pressure-flow characteristics during expiration, expiratory resistance may be an important consideration in conjunction with altered compliance and time constant for an individual patient, with any limitation in the expulsion of air potentially resulting in gas trapping and difficulty initiating the next breath. This may be an important factor even during controlled mandatory ventilation in a patient with inadequate expiratory muscle recruitment.
Any increase in respiratory work load can cause difficulty during weaning from mechanical ventilation and could delay or even completely abort the process.12,24 We acknowledge that resistance from artificial airways is not the only contributor. Additional equipment factors, such as ventilation mode and ventilation parameters and tracheostomy cuff status (inflated or deflated), will influence respiratory work, as will patient factors, including preexisting anatomy and physiology, comorbidities, lung compliance, and secretions. However, if the type of tube (including the presence or absence or type of inner cannula) can alter resistance to air flow in isolation, then tracheostomy tube selection should be an important clinical consideration; added resistance may be significant in some patients who may not cope with increased respiratory work during the weaning process, such as those with altered lung compliance or respiratory muscle weakness.7
There were limitations to this study. We measured airway pressure and calculated airway resistance at varying flows during both inspiration and expiration. This provides robust data that allow consideration of the clinical implications under a variety of conditions, including controlled, assisted, supported, and spontaneous ventilation in patients with normal or abnormal respiratory mechanics and muscle strength. Our results were highly reproducible, which may reflect the quality of calibrated equipment and apparatus set-up. However, it is acknowledged that the constant air flow used to derive resistance at a particular flow is not representative of the decelerating flow used during inspiration in many intensive care settings. Because the resistance data demonstrate a non-linear increase in resistance with increasing flow, probably due to variable components of laminar and turbulent flow, the additional resistive pressure due to the tracheostomy tube will reflect the moment by moment flow and hence the flow profile. Using the data we provide (see Table 2), an estimate of this variable effect can be made once the flow profile and rate are known. For example, with a decelerating flow profile, as is commonly used during inspiration, the additional pressure will fall over time in an almost exponential fashion due to both the reduction in flow itself and the associated fall in resistance. Depending on the form of ventilator assistance used, all of the waveforms will be different; therefore, the use of constant flow allows accurate estimation of resistance and aids understanding of the likely effects across a range of clinical situations.
An alternative method would have been to measure imposed work of breathing using a lung model. Whereas this may have given a more direct estimate of the inspiratory effects under a particular breathing pattern, the direct inspiratory resistive work component can easily be estimated from the resistance and a given inspiratory flow pattern; however, the effects of an increase in expiratory resistance are not easily modeled. For example, the magnitude of imposed expiratory resistance that we have documented with some of these tracheostomy tubes would probably lead to an excessive expiratory time constant and gas trapping. In turn, this might lead to efforts to increase expiratory flow by active contraction of the expiratory muscles and to difficulty triggering the next breath, leading to increased elastic work. The clinical implications of these potential effects would be dependent on patient factors, such as the strength of the respiratory muscles, the patient's respiratory mechanics, and the patient's ventilator demand. Given these caveats, we chose to report inspiratory and expiratory resistance effects to allow individual estimation of the potential impact depending upon the range of clinical parameters described above.
Although the current research has confirmed increased airway pressures with some of the equipment that may be used to facilitate speech, re-establishing communication for patients with a cuffed tracheostomy tube is of great psychosocial benefit for patients and their families and has a significant impact on quality of life.25–27 Furthermore, the restoration of communication can influence practical health care via expression of clinical needs, such as pain or consent,28 enabling discussion regarding treatment goals and direction of care, improved patient motivation and participation in therapy,29 and identification of laryngeal dysfunction, which may in turn impact respiratory goals and decision making.30 However, it is important that communication be re-established within a context that does not interfere with respiratory goals and patient recovery. Hence, it is necessary to understand the impact of using specialty tracheostomy tubes (including impact of specific inner cannulas) for communication and to establish the evidence for indications or contraindications for their use.
Conclusions
Tracheostomy tube type and inner cannula selection affected pressure and resistance to air flow during inspiration and expiration, which may have significant implications for air flow dynamics and work of breathing in vulnerable patients, particularly those receiving supported ventilation or during the weaning process. Our data provide clinicians with relevant information to guide decision making regarding selection of airway equipment or when setting parameters for monitoring patient tolerance.
Acknowledgments
The study was performed in the Flinders Medical Centre ICU. Illustrations were provided by TypeSpace Graphic Design Adelaide.
Footnotes
- Correspondence: Lee N Pryor SP, Speech Pathology Department, Royal Adelaide Hospital, North Terrace, Adelaide, South Australia 5000, Australia. E-mail: lee.pryor{at}health.sa.gov.au.
Royal Adelaide Hospital Research Foundation grant funding was used to purchase tracheostomy tubes and enable clinical backfill for Ms Pryor during bench model testing. Portex tubes were provided by the manufacturer, and Blom and Shiley tubes were purchased. Ms Pryor has disclosed a relationship with the Australian distributor of the Blom tubes in this study. The other authors have disclosed no conflicts of interest.
Supplementary material related to this paper is available at http://www.rcjournal.com.
- Copyright © 2016 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}