

Abstract
BACKGROUND: Transbronchial lung biopsy with flexible forceps is the most commonly used technique in diagnosis of diseases diffusely involving the lung parenchyma. Recently, transbronchial lung biopsy using the flexible cryoprobe (cryo-transbronchial lung biopsy) has also been reported. Herein, we perform a systematic review and meta-analysis describing the efficacy and safety of cryo-transbronchial lung biopsy.
METHODS: The PubMed and EMBASE databases were searched for studies reporting the outcomes of cryo-transbronchial lung biopsy in subjects with diffuse parenchymal lung involvement. The quality of individual studies was assessed using the QualSyst tool. The pooled diagnostic yield of cryo-transbronchial lung biopsy was calculated using proportion meta-analysis (random effects model). Heterogeneity was evaluated using the I2 test and Cochran Q test. Publication bias was determined using both statistical and graphical methods.
RESULTS: Our search yielded 14 studies (1,183 subjects). The pooled diagnostic yield of cryo-transbronchial lung biopsy was 76.9% (95% CI 67.2–85.3) if only definitive diagnoses were considered and 85.9% (95% CI 78.2–92.2) if both definitive and probable diagnoses were considered. Four studies (321 subjects) the performance of flexible forceps biopsy and cryo-transbronchial lung biopsy. The diagnostic yield of cryo-transbronchial lung biopsy (86.3, 95% CI 80.2–90.8) was significantly higher than that of flexible forceps biopsy (56.5%, 95% CI 27.5–83.2) with an odds ratio of 6.7 (95% CI 3.6–12.4) and a number needed to treat of 4. Lung tissue was obtained in 98% of all samples with cryo-transbronchial lung biopsy and was free of compression artifacts. The size of samples obtained with cryo-transbronchial lung biopsy was significantly bigger compared with flexible forceps biopsy (20.4 vs 4.3 mm2, P = .005). The complications of cryo-transbronchial lung biopsy included pneumothorax (6.8%), severe bleeding (0.3%), and death (0.1%). Clinical and statistical heterogeneity was present, and there was evidence of publication bias.
CONCLUSIONS: Cryo-transbronchial lung biopsy is a relatively safe procedure with good diagnostic yield in diseases diffusely involving the lung parenchyma.
- cryotherapy
- interstitial lung disease
- idiopathic pulmonary fibrosis
- idiopathic interstitial pneumonia
- sarcoidosis
- bronchoscopy
Introduction
Diffuse parenchymal lung diseases are a heterogeneous group of disorders that affect the pulmonary parenchyma and include sarcoidosis, connective tissue disease-associated interstitial lung diseases, occupational lung diseases, idiopathic interstitial pneumonias, and others.1,2 Certain infections, such as cytomegalovirus pneumonia, and post lung transplant conditions, such as acute rejection, diffusely involve the lung parenchyma and mimic other diffuse parenchymal lung diseases on radiologic evaluation.3,4
Transbronchial lung biopsy, performed with flexible forceps during flexible bronchoscopy, has been the most commonly employed technique for obtaining lung tissue for histopathological examination in diffuse parenchymal lung diseases.5,6 Flexible forceps biopsy is minimally invasive and does not require general anesthesia, thereby allowing the procedure to be performed on a day-care basis.7 However, it has significant limitations, including a variable diagnostic yield ranging from 30 to 75% (depending on the underlying disorders). It has an especially lower yield in fibrotic diffuse parenchymal lung diseases, such as idiopathic pulmonary fibrosis (IPF) and nonspecific interstitial pneumonia.6,8–10 Further, the size of the lung tissue specimen obtained with flexible forceps biopsy is small and frequently associated with artifacts (especially compression or crush artifacts), thus limiting its diagnostic utility.11,12 For this reason, flexible forceps biopsy is not recommended for the diagnosis of diffuse parenchymal lung diseases, such as IPF.13 Besides, the procedure is not without risk; pneumothorax and airway bleeding are important complications that might occur with flexible forceps biopsy and may result in hypoxia, ICU admissions, and prolonged hospital stay.7,14,15
Surgical lung biopsy provides large tissue samples for histopathological analysis and is the current reference standard for the diagnosis of idiopathic interstitial pneumonias, such as IPF, nonspecific interstitial pneumonia, and others.16 However, the procedure is performed in the operating room under general anesthesia and requires the mandatory insertion of an intercostal drain. It may be associated with significant morbidity (2–20%), including prolonged air leak and prolonged hospital admission, and mortality (2–17%).17–23
Transbronchial lung biopsy can also be performed using cryoprobes, termed cryo-transbronchial lung biopsy.24 Cryotherapy works on the principle of the Joule-Thomson effect, wherein the adiabatic expansion of a compressed gas leads to rapid cooling. The cooled tip of the cryoprobe adheres to the tissue due to crystallization of water molecules at the interface. Cryoprobes have been traditionally used during bronchoscopy for endobronchial tumor ablation, endobronchial biopsy, and recanalization by extraction of tumors and/or blood clots25,26; their use for performing transbronchial lung biopsy is relatively recent.27 Herein, we perform a systematic review and meta-analysis of studies investigating the yield and safety of cryoprobe for performing cryo-transbronchial lung biopsy in subjects with disorders diffusely involving the lung parenchyma.
QUICK LOOK
Current knowledge
Transbronchial lung biopsy with flexible forceps and surgical lung biopsy are commonly used modalities in the diagnosis of diseases diffusely involving the lung parenchyma. Recently, transbronchial lung biopsy using the flexible cryoprobe (cryo-transbronchial lung biopsy) has also been reported.
What this paper contributes to our knowledge
The results of this study suggest that cryo-transbronchial lung biopsy has a good diagnostic yield in diseases diffusely involving the lung parenchyma with an acceptable safety profile.
Methods
Search Strategy
We first confirmed the absence of any systematic review in the PubMed and EMBASE databases on the role of cryo-transbronchial lung biopsy in diffuse lung diseases. Subsequently, all of the authors performed an independent search of the PubMed and EMBASE databases for relevant studies published through August 2015 describing the use of a cryoprobe for performing transbronchial lung biopsy in subjects with diseases diffusely involving the lung parenchyma. The following free text search terms were utilized: (cryo OR cryobiopsy OR cryobiopsies OR cryoprobe OR cryotherapy OR cryotechnology) AND (lung biopsy OR transbronchial OR trans-bronchial OR lung biopsies). The list of references of original, editorials, reviews, and our personal files were also checked for relevant citations. We excluded the following: (1) case reports, abstracts, comments, editorials, and reviews; (2) studies describing cryo-transbronchial lung biopsy in <10 subjects; (3) studies describing the use of cryo-transbronchial lung biopsy for a localized lung lesion; and (4) studies that could possibly have overlap of data with another study from the same center.
Initial Review of Studies
The bibliographic list thus retrieved from the electronic and manual searches was imported into the reference manager package, and all duplicate citations were discarded. Two authors (SD and RA) scrutinized these citations by examination of the title and abstract to identify the relevant studies. Any disagreement was resolved by discussion between the authors. This database was then screened again to include only primary articles. The full text of each of these studies was obtained and reviewed in detail.
Data Abstraction
Data were entered into a standard data extraction form. The following items were extracted: (1) publication details (authors, year of publication, and other citation particulars, including the country of origin); (2) study design (prospective or retrospective); (3) patient population, number of subjects, and the comparator; (4) details of the procedure (anesthetic agents used and depth of anesthesia, use of rigid bronchoscopy or endotracheal intubation, the cryoprobe and cryogen used, duration of cooling, and duration of procedure); (5) characteristics of biopsy specimens (number, surface area, presence of lung tissue and alveolar spaces, presence of artifacts, and use of digital morphometry); (6) diagnostic characteristics (diagnostic yield, specific diagnoses, and diagnostic gold standard); and (7) complications associated with the procedure (severe bleeding defined according to British Thoracic Society guidelines,7 pneumothorax, and death). Complications were attributed to cryobiopsy for studies in which cryobiopsy and flexible forceps biopsy were performed in the same subject.
Assessment of Study Quality
Each study included in this review was adjudged for its quality and validity using the QualSyst tool for qualitative studies28 independently by 2 authors (SD and RA) for the stated criteria. Weighted Cohen's kappa co-efficient was used to define the inter-observer agreement for selection of studies.
Statistical Analysis
The statistical software package StatsDirect 2.8.0 (StatsDirect Ltd, Altrincham, UK) was used to perform the statistical analyses. The diagnostic yield of cryo-transbronchial lung biopsy was analyzed by calculating the proportions for the individual studies (n/N, where n is the number diagnosed with the help of cryo-transbronchial lung biopsy, and N is the total number of subjects evaluated).29,30 The proportions were pooled using a DerSimonian random effects model in the presence of significant heterogeneity. The odds ratio and 95% CIs were calculated to assess the diagnostic yield in the cryo-transbronchial lung biopsy versus the flexible forceps biopsy group. The results from individual studies were pooled using the random effects model.31 The number needed to treat (equal to 1/risk difference) was calculated to estimate the number of cryo-transbronchial lung biopsy procedures that need to be performed to achieve one additional diagnosis compared with flexible forceps biopsy.
Assessment of Heterogeneity
Heterogeneity for the individual outcomes was assessed using the I2 test, which measures the extent of inconsistency among the results of the studies. An I2 value of ≥50% indicates significant heterogeneity.32 Heterogeneity was also assessed using the Cochran Q statistic, and a P value of <.1 was considered to be significant.33
Estimation of Publication Bias
The presence of publication bias was evaluated using the funnel plot (proportion on x axis against the standard error of the proportion on the y axis).34 Publication bias was also investigated using the Egger test35 and Begg-Mazumdar test.36 An ethics committee approval was not required because this was a systematic review of published studies.
Results
The initial database search retrieved a total of 393 citations, of which 14 studies (1,183 subjects in total, 805 undergoing cryobiopsy) finally met the inclusion criteria (Fig. 1).27,37–49 Nine studies were retrospective,27,38–40,43,44,46–48 whereas 5 studies were prospective (4 observational,37,41,42,49 one randomized trial45) (Table 1). Ten studies were conducted in subjects with diffuse lung disease,27,37,40,42–45,47–49 2 in lung transplant recipients,39,41 one in immunocompromised subjects with pulmonary infiltrates,38 and one including subjects from all 3 categories46 (Table 1). The studies were generally of good quality (Table 2), with the median (interquartile range) QualSyst score being 18 (17–19). The inter-observer agreement for scoring of study quality was good (weighted Cohen's kappa = 70.3%). Flexible forceps biopsy was the comparator in 6 studies, whereas cryobiopsy was compared against surgical lung biopsy in one study.

Flow chart. TBLB = transbronchial lung biopsy; SPN = solitary pulmonary nodules.
Characteristics of the Included Studies
QualSyst Tool for Assessment of Quality of the Included Studies
The procedures were performed most commonly under conscious sedation in spontaneously breathing subjects (11 studies); in one study, general anesthesia was employed, whereas in 2 other studies, either of the 2 modalities were used (Table 3). Midazolam with alfentanil (4 studies) and propofol with remifentanil (4 studies) were the most commonly used combinations of sedative/anesthetic and analgesic agents (Table 3). The subjects were intubated with one of the following artificial airways namely the endotracheal tube (6 studies), rigid bronchoscope (3 studies), or laryngeal mask airway (1 study). In 4 studies, the procedure was performed without endotracheal intubation (Table 3). The procedures were performed through a flexible bronchoscope under fluoroscopic guidance in all of the studies. A 2.4-mm cryoprobe was used in a majority of the studies (9 studies), with nitrous oxide as the cryogen (8 studies) and a cooling time ranging from 3 to 6 s (Table 3). The mean duration of the procedure was reported in 6 studies and ranged from 6 to 35 min (Table 3). In most studies, 2–3 cryobiopsy samples were obtained; in one study each, the number was 5 and up to 6, respectively (Table 4). A chest radiograph was performed after the procedure in all of the studies. Digital morphometry was performed in 3 studies.27,43,44 The mean surface area of the biopsy samples was significantly higher with the cryoprobe in comparison with flexible forceps (20.4 vs 4.3 mm2, P = .005). Lung tissue was obtained in 391 of the 399 (98%) cryobiopsy cases in which it was reported (Table 4). The number of alveolar spaces or percentage alveolated area as well as the artifact-free area was higher with the cryoprobe than with flexible forceps biopsy (Table 4). Artifacts associated with the use of the cryoprobe included cold-related artifacts, acute lung injury changes, and the presence of ciliated columnar epithelium in alveolar spaces.42,49 Nine studies explicitly defined a diagnostic reference standard (Table 5), which included: (1) interdisciplinary discussion between clinician, radiologist, and pathologist (5 studies); (2) clinical, radiographic, and pathological findings with 6-month follow-up (one study); and (3) clinical, radiographic, and pathological findings (3 studies).27,38,40,43–45,47–49 A variety of diffuse parenchymal lung diseases, including IPF and nonspecific interstitial pneumonia, could be diagnosed with the help of cryo-transbronchial lung biopsy (Table 5).
Details of the Cryo-Transbronchial Lung Biopsy Procedure
Characteristics of Transbronchial Lung Biopsies Obtained in the Included Studies
Diagnostic Characteristics in the Included Studies
Diagnostic Yield of Cryo-Transbronchial Lung Biopsy
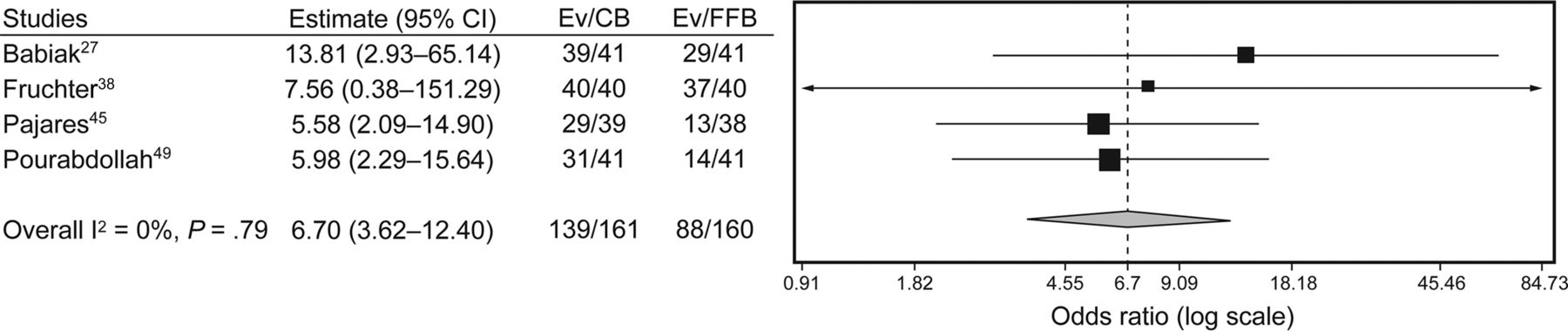
Twelve studies (472 subjects) reported the diagnostic yield of cryo-transbronchial lung biopsy (Table 5).27,37–40,42–45,47–49 Five studies further classified the diagnoses achieved with the help of cryo-transbronchial lung biopsy as definite (or confident) or probable.42,43,47–49 The diagnoses achieved in the remaining 7 studies were considered definite.27,37–40,44,45 The pooled diagnostic yield was 76.9% (95% CI 67.2–85.3) if only the definite diagnoses were considered, whereas it was 85.9% (95% CI 78.2–92.2) when both definite and probable diagnoses were considered (Fig. 2). Four (3 observational, one randomized) studies (Table 6) compared the diagnostic yield of cryobiopsy (161 subjects) with flexible forceps biopsy (160 subjects). The diagnostic yield was significantly higher with cryo-transbronchial lung biopsy (86.3%, 95% CI 80.2–90.8%) compared with flexible forceps biopsy (56.5%, 95% CI 27.5–83.2%) with an odds ratio of 6.7 (95% CI 3.6–12.4%), and a number needed to treat of 4 (Fig. 3).

Diagnostic yield of definite (A) and definite/probable (B) of transbronchial lung biopsy with cryoprobe (random effects model). The diagnostic yield in the individual studies is represented by a square (percentage) through which runs a horizontal line (95% CI). The diamond at the bottom represents the pooled diagnostic yield from the studies.
Characteristics of Studies That Compared the Diagnostic Yield of Cryoprobe Biopsy With Flexible Forceps Biopsy

Forest plot showing the diagnostic yield (both probable and definite) with transbronchial lung biopsy performed with cryoprobe (CB) versus flexible forceps biopsy (FFB). The diagnostic yield was significantly higher in the CB group (odds ratio with 95% CIs, random effects model).
Safety of Cryo-Transbronchial Lung Biopsy
Complications were reported by 13 studies for 764 cryo-transbronchial lung biopsy procedures. Overall, there were 55 (7.2%) major complications. Pneumothorax occurred in 52 (6.8%), severe bleeding in 2 (0.3%), and death in one (0.1%) case (Table 7). The highest rate of pneumothorax (28%) was observed in the study performed in subjects with fibrotic diffuse parenchymal lung diseases.42 The only death was also reported in the same study and was caused by an exacerbation of IPF.42
Complications Associated With Transbronchial Biopsy Reported in the Included Studies
Clinical heterogeneity was evident in the nature of the studies (prospective vs retrospective), patient population, and diagnostic gold standards (Tables 1 and 5). Significant statistical heterogeneity was also observed for the outcome of diagnostic yield of the procedure (I2 = 79.6; Cochran Q statistic 53.9, P < .001). There was evidence of publication bias on visual examination of the funnel plot (Fig. 4) and on statistical tests (Begg-Mazumdar: Kendall's tau = −0.545, P = .009; Egger: bias = −3.577, P < .001).
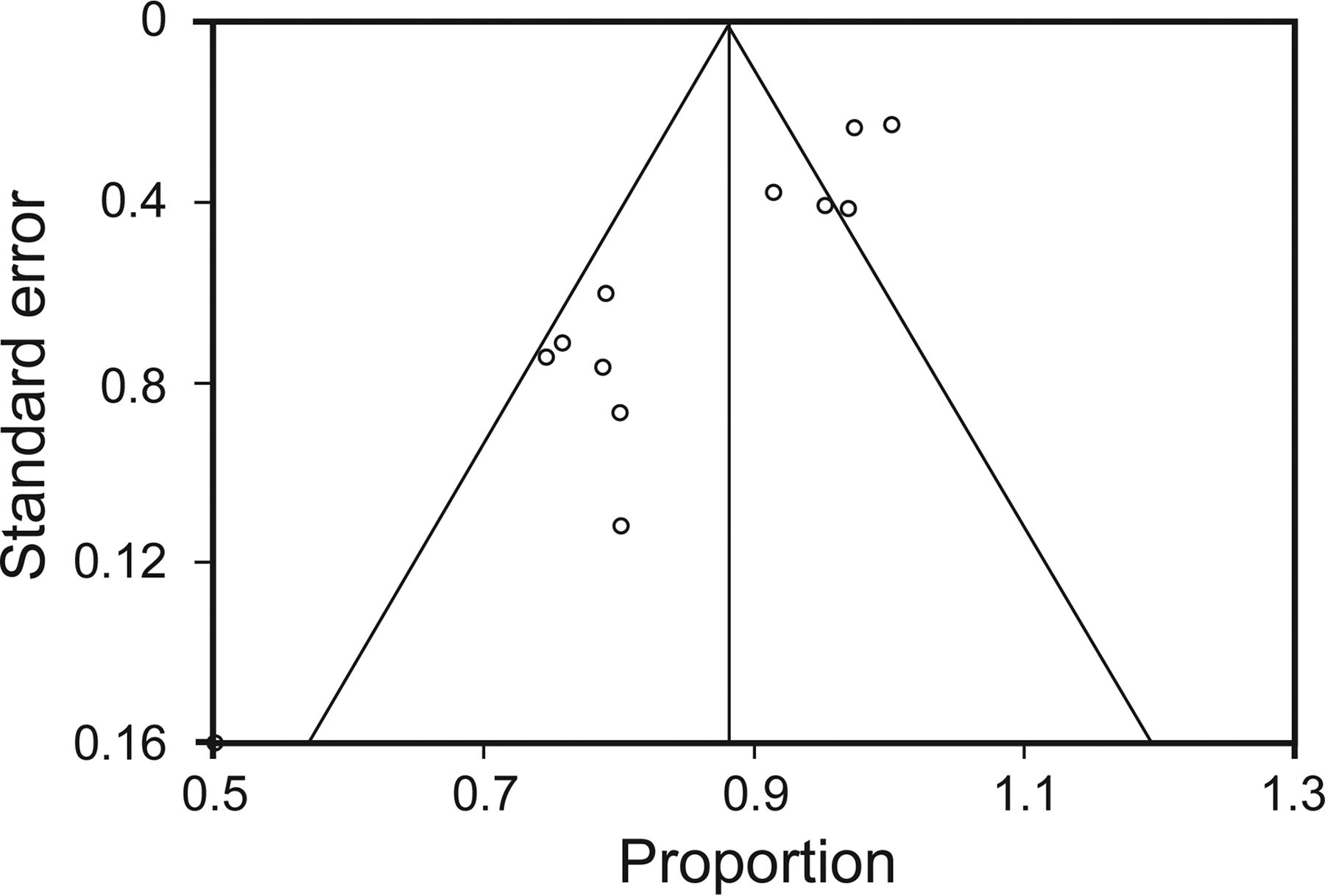
Funnel plot comparing the proportion versus the SE of the proportion for the diagnostic yield. The circles represent the studies included in the meta-analysis. The line in the center indicates the summary proportion. The other lines represent the 95% CIs. There was evidence of publication bias.
Discussion
The results of this study indicate that cryo-transbronchial lung biopsy has a good diagnostic yield (86%), higher than that of flexible forceps biopsy (57%), for obtaining transbronchial lung biopsies in subjects who have diffuse parenchymal lung involvement. In fact, only 4 procedures need to be performed with cryo-transbronchial lung biopsy to obtain one additional diagnosis, compared with flexible forceps biopsy. The cryo-transbronchial lung biopsy procedure is generally safe, associated with a small risk of pneumothorax (6.8%) and a very small risk of severe bleeding (0.3%) and death (0.1%).
The high yield of cryo-transbronchial lung biopsy can be attributed to several factors, including the presence of lung tissue in the biopsy specimen in almost all (98%) cases, large size of the samples, and the absence of significant artifacts. When the cryoprobe is placed deep inside a sub-segmental bronchus and activated for 3–4 s, the lung parenchymal tissue freezes around the probe and adheres to the probe tip. Subsequent traction of the probe allows shearing off of a large volume of the lung parenchyma during withdrawal of the probe. This is unlike the flexible forceps biopsy technique, where the jaws of the forceps grasp the parenchyma, with the potential of causing compression/crush artifacts. The surface area of the cryobiopsy specimen was higher than the flexible forceps biopsy samples by almost 5 times, and these larger samples with sufficient vascular and bronchiolar tissue help in a confident histological diagnosis of the subtype of the fibrotic diffuse parenchymal lung diseases as well as exclusion of cellular rejection and bronchiolitis in the lung transplant population.39
Although transbronchial flexible forceps biopsy provides a good diagnostic sensitivity in diseases like sarcoidosis, organizing pneumonia, lymphangitis carcinomatosis, and infections, the yield is poor in case of interstitial lung diseases, such as IPF, nonspecific interstitial pneumonia, respiratory bronchiolitis-associated interstitial lung disease, and others.9,10,50–52 This is due to the requirement of larger sized lung tissue for differentiating IPF from hypersensitivity pneumonitis and nonspecific interstitial pneumonia, as the former requires the demonstration of temporal and spatial heterogeneity.13 Further, other features like patchy interstitial fibrosis, fibroblast foci, and honeycombing need to be identified.13 A large variety of diffuse parenchymal lung diseases, which are difficult to be diagnosed confidently on small flexible forceps biopsy samples were diagnosed with cryo-transbronchial lung biopsy in the included studies (including IPF, nonspecific interstitial pneumonia, desquamative interstitial pneumonia, pulmonary Langerhans cell histiocytosis, and hypersensitivity pneumonitis), thus emphasizing the utility of this novel technique.
The present analysis also highlights the relative safety of the cryo-transbronchial lung biopsy procedure. The larger defect in the lung parenchyma resulting from a cryo-transbronchial lung biopsy is expected to increase the risk of pneumothorax significantly as compared with flexible forceps biopsy. The incidence of pneumothorax was 6.8% (52 of 764), which is higher than the usual reported rate reported with the flexible forceps biopsy.7,14,15,53,54 However, the risk of pneumothorax is less than that would be expected, considering the larger biopsy tissues obtained with cryo-transbronchial lung biopsy. The possible reasons include the universal use of fluoroscopy while performing cryo-transbronchial lung biopsy and fewer samples required for diagnosis with cryo-transbronchial lung biopsy. Moreover, one third of the pneumothoraces (19 of 52) in the present review occurred in a single study conducted in fibrotic diffuse parenchymal lung diseases. The authors of this study have attributed the high incidence (28% in that study) to the type of patient population and the necessity to biopsy subpleural areas. Thus, the risk of pneumothorax with cryo-transbronchial lung biopsy is acceptable in most patients. Importantly, this needs to be interpreted in light of the fact that only a proportion of the patients (maximum 28%)42 would require an intercostal drain with cryo-transbronchial lung biopsy, compared with 100% patients who undergo surgical lung biopsy.
Severe bleeding (requiring either cessation of the procedure or the use of a bronchial blocker/sealant or surgical intervention for control; bleeding that led either to cardiopulmonary instability or requirement of a blood transfusion or admission to the ICU) occurred in only 0.3% of cases, similar to that seen with flexible forceps biopsy during flexible bronchoscopy, despite the significantly large size of lung tissue samples.7 It is postulated that the freezing effect of the cryoprobe coagulates the small vessels ruptured during the process of biopsy, thereby reducing the risk of significant bleeding. The data on mild and moderate bleeding are not presented because the definition of these categories was variable in the included studies. The mortality rate was also low (0.1%), comparable with that seen with flexible forceps biopsy.7 This is much lower than that for surgical lung biopsy (2–17%).17–23 It is noteworthy that all of the studies considered in this review have excluded patients who had reduced lung function, evidence of pulmonary artery hypertension on echocardiography, hemodynamic instability, hypoxemia, or coagulopathy. Thus, the findings of safety of cryo-transbronchial lung biopsy in the present analysis do not apply to patients presenting with any of these features.
The present analysis has a few limitations. First, the diagnostic reference standards used in the studies are different. In the ideal scenario, the yield of a new diagnostic modality such as cryo-transbronchial lung biopsy should be assessed using surgical lung biopsy as the reference standard, with both of the procedures performed in all of the patients. However, because surgical lung biopsy is invasive and is associated with high morbidity and mortality, many patients frequently do not consent for the performance of surgery; hence, it may not be feasible to have such a study design. A diagnosis achieved after a multidisciplinary discussion assimilating all of the clinical, radiologic, and histopathological data (also used in many of the included studies) constitutes the most feasible composite reference standard, endorsed by the American Thoracic Society/European Respiratory Society guidelines for diagnosis of idiopathic interstitial pneumonias.2,16 Also, we attributed pneumothorax as a complication to cryo-transbronchial lung biopsy where both cryo-transbronchial lung biopsy and flexible forceps biopsy were performed in the same subject. However, these occurred in only 3 instances, and we attributed them to cryo-transbronchial lung biopsy based on a worst case scenario analysis. Most of the studies in this analysis are retrospective observational studies, thus providing only moderate quality evidence for the utility of this technique. Finally, the studies included in this analysis have significant clinical heterogeneity because they have been performed in varied patient populations. There was also the presence of publication bias, which could impact the conclusions of the study. Hence, the results of the present analysis should be considered as hypothesis-generating and require confirmation in larger multi-center randomized trials.
Conclusions
Transbronchial lung biopsy performed with a cryoprobe during flexible bronchoscopy is safe and offers a high diagnostic yield in subjects with diseases diffusely involving the lung parenchyma. In this early appraisal, the technique seems promising in the evaluation of diffuse parenchymal lung diseases.
Footnotes
- Correspondence: Ritesh Agarwal MD DM, Department of Pulmonary Medicine, Postgraduate Institute of Medical Education and Research, Sector-12, Chandigarh 160012, India. E-mail: agarwal.ritesh{at}outlook.in.
The authors have disclosed no conflicts of interest.
- Copyright © 2016 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}
{kind=link}