

Abstract
BACKGROUND: Some pediatric tracheostomized patients who receive inhaled drugs undergo decannulation, and it is unknown whether the dose has to be adjusted. Pressurized metered-dose inhalers (pMDIs) and soft mist inhalers (SMIs) used with valved holding chambers (VHCs) made of non-electrostatic material are available. We hypothesized that using an SMI and changing the delivery route from tracheostomy to oronasal would increase lung dose.
METHODS: Four units of a metallic VHC were studied with albuterol hydrofluoroalkane (pMDI) and albuterol/ipratropium bromide with an SMI using an anatomically correct in vitro model of a 5-y-old spontaneously breathing tracheostomized child. The drug was captured in a filter and was termed lung dose. We tested breathing patterns with tidal volumes of 50, 155, and 300 mL. A mask and a special adapter were used as interfaces for oronasal and tracheostomy delivery, respectively. Spectrophotometry (276 nm) was used to determine albuterol concentration.
RESULTS: The use of SMI resulted in a higher lung dose than the pMDI for all tested conditions except delivery through tracheostomy with tidal volume of 155 mL (P = .69). Switching from oronasal to tracheostomy delivery increased the lung dose for all tested conditions except for the pMDI with the 300-mL tidal volume (P = .83). The use of SMI resulted in higher deposition in the tracheostomy tube than the pMDI.
CONCLUSIONS: In general, an SMI delivers a higher lung dose than a pMDI when using a metallic spacer during oronasal and tracheostomy route with the latter providing a higher lung dose.
- tracheostomy
- drug delivery
- aerosol
- valved holding chamber
- metered dose inhaler
- artificial airway
- soft mist inhaler
- Respimat
- pediatrics
Introduction
Many pediatric patients who undergo tracheostomy receive long-term treatment with inhaled aerosols.1 Also, many children with chronic lung disease and tracheostomy could be decannulated, but they continue to require inhaled aerosols. Currently, there are no guidelines to help the practitioner optimize drug delivery in that patient population.2
A survey of aerosol delivery practices in tracheostomized children revealed that 92% of the responders used pressurized metered-dose inhalers (pMDIs).1 In addition, 83% of those using unassisted methods reported using valved holding chambers (VHCs). The goal of using a VHC is to remove the need of actuation and inhalation coordination.3 There are several components that are crucial to optimal VHC performance (ie, material used).3 There are 2 types of non-electrostatic materials used for VHCs: polymer and metal. Previous studies have reported different performance among VHCs made of different non-electrostatic materials.4
Traditionally, metered-dose inhalers contained propellants, but more recently, a new type of inhaler has been introduced in the market. The Respimat (Boehringer Ingelheim Pharmaceuticals, Ridgefield, New Jersey), also known as the Soft Mist inhaler (SMI) is a propellant-free metered-dose inhaler that provides a slower mist than traditional pMDIs.5 The delivery device is approved in the United States and in Europe for the following drugs: albuterol/ipratropium bromide, tiotropium bromide/olodaterol, olodaterol, and tiotropium bromide. The pMDI for albuterol/ipratropium bromide was replaced by an SMI in the United States and is no longer available. The use of a VHC is not required in adults and older children.6,7 However, handling studies of the Respimat device recommend the addition of a VHC in children ≤5 y old.8 The Respimat with a VHC effectively delivered aerosol to a group of sleeping infants.9
Due to the paucity of clinical studies, most of our insight on optimization of aerosol delivery with pMDIs and VHCs through tracheostomy derives from in vitro studies.10–12 Those studies reported that the type of VHC, breathing patterns, and other factors affect drug delivery of pMDI through tracheostomies. Recently, Cooper et al12 compared oronasal and tracheostomy delivery of albuterol using a pMDI with 2 different VHCs and a continuous output jet nebulizer. They found that the type of VHC and breathing pattern affect the difference between the lung dose obtained via tracheostomy and oronasal routes.12
Knowledge regarding the effect of different drug delivery devices (pMDI vs SMI) and VHCs (metallic vs antistatic polymer) is needed. We hypothesize that the use of SMI, larger tidal volumes, and changing the delivery route from tracheostomy to oronasal will result in a higher lung dose. We also hypothesize that a metallic VHC will perform similarly to one of similar size made of antistatic polymer.
QUICK LOOK
Current knowledge
Spontaneously breathing tracheostomized pediatric patients often receive inhaled treatments with metered-dose inhalers and valved holding chambers. Soft mist inhalers are currently available in the United States.
What this paper contributes to our knowledge
A soft mist inhaler delivered more albuterol than a metered-dose inhaler when both were used with a non-electrostatic chamber in an anatomically correct model of a spontaneously breathing tracheostomized child.
Methods
The experiments were performed at the Pediatric Aerosol Research Laboratory at Arkansas Children's Research Institute, Little Rock, Arkansas.
Breathing Model
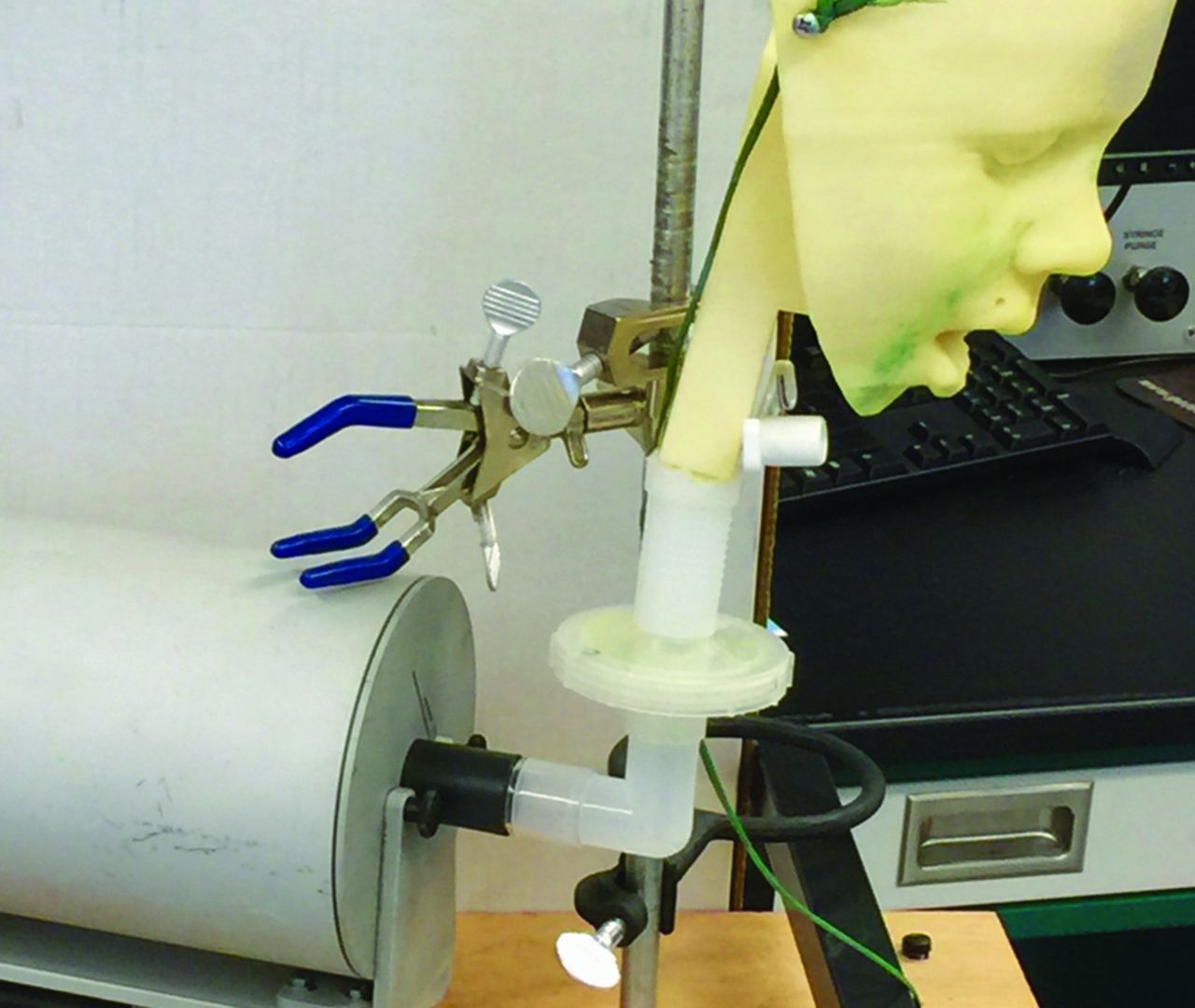
A previously published anatomically correct model of a spontaneously breathing tracheostomized 5-year-old child was used.12 Briefly, a 3-dimensional printed oronasal head model of a 5-y-old child was connected in series to a low dead space filter holder and a breathing simulator (PARI Compass, Munich, Germany) (Fig. 1). The breathing patterns of an infant (tidal volume 50 mL, breathing frequency 30 breaths/min, inspiratory-expiratory ratio 1:3), a child (tidal volume 155 mL, breathing frequency 25 breaths/min, inspiratory-expiratory ratio 1:2), and an older child (tidal volume 300 mL, breathing frequency 25 breaths/min, inspiratory-expiratory ratio 1:2) were used. The model had a hole to allow the insertion of the tracheostomy tube that was occluded during oronasal delivery experiments. A 4.5-mm/6.3-mm inner diameter/outer diameter tracheostomy tube (TRACHOE Medical GmbH, Nieder-Olm, Germany) was used.

Experimental setup.
Devices
Albuterol pMDI (Ventolin hydrofluoroalkane [HFA], 90 μg/actuation; GlaxoSmithKline, Brentford, United Kingdom) and SMI albuterol/ipratropium bromide (Combivent Respimat, 100 μg of albuterol/actuation, Boehringer Ingelheim Pharmaceuticals, Ridgefield, New Jersey) were used. During oronasal delivery, 4 units of metallic VHC (Vortex Tracheo, PARI GmbH, Starnberg, Germany) with its medium size mask (Felix Frog SmartTouch Mask, PARI Midlothian, Virginia) were used (Fig. 2). The Vortex Tracheo is commercialized in Europe but not in the United States. The metallic VHC is not transparent and has a volume of 194 mL. The operation of the inhalation valve can be observed through the mouthpiece. During tracheostomy delivery, the VHC was connected to the tracheostomy tube with a special adapter that is present in the Vortex Tracheo, and during oronasal delivery, the adapter was removed and the mask was connected.

Devices and interfaces used during oronasal and tracheostomy aerosol delivery. Top: Vortex valved holding chamber. Middle: Tracheostomy adapter. Bottom: Face mask.
Protocol
Oronasal Delivery.
A new disposable filter (PARI Respiratory Equipment, Midlothian, Virginia) was used with each run. The model was operated in the vertical position as previously reported.11,12 After selecting a breathing pattern, the accuracy of the tidal volume was verified using a mass flow meter (TSI, Shoreview, Minnesota).11,12 The seal between the head/airway model and the mask was achieved with putty.12 The pMDI was primed with 4 puffs at the beginning of every testing day and was shaken for 5 s before each actuation. The SMI was primed before use as per the manufacturer's recommendations. The same canister was used for each run to minimize variability. The pMDI and the SMI were inserted into the back of the VHC. The breathing simulator provided 7 breaths, and the inhalers were actuated at the beginning of the second inhalation.12 A total of 10 actuations were utilized to improve drug recovery, and the used filter was processed for albuterol concentration.11,12 The VHCs were cleaned and air-dried, and lack of residual drug was verified by spectrophotometry. This process was done for each of the 2 devices (pMDI and SMI) and for each of the 3 breathing patterns (infant, child, and older child).
Tracheostomy Delivery.
A similar procedure was used for tracheostomy delivery except that the mask was replaced by a special adapter to connect to the tracheostomy tube. Upon completion of each experiment, the tracheostomy tube was removed and flushed with 10 mL of double-deionized water. The filter and tracheostomy samples were analyzed with a spectrophotometer.
Albuterol Determination
After washing with double-deionized water the filter holder and the filter, the latter was placed in a 50-mL tube and was vigorously vortexed and shaken. The samples were analyzed with spectrophotometry at 276 nm (Biomate 3 UV-visible spectrophotometer, Thermo Fisher Scientific, Waltham, Massachusetts).12
Statistical Analysis
Lung dose (amount of albuterol recovered from the filter) was the main outcome. The comparison of lung doses between oronasal and tracheostomy delivery and between the 2 devices was done with unpaired t test. The effects of breathing patterns for each device/delivery route scenario on lung dose were studied with analysis of variance followed by Tukey test (multiple comparisons). P values of <.05 were considered statistically significant. Calculations were done with a statistical software package (Kaleidagraph 4.1, Synergy Software, Reading, Pennsylvania).
Results
Results are expressed in Table 1 and Figure 3.
Lung Dose (μg of Albuterol) Achieved With Different Valved Holding Chambers With Pressurized Metered-Dose and Soft Mist Inhalers During Oronasal and Tracheostomy Delivery

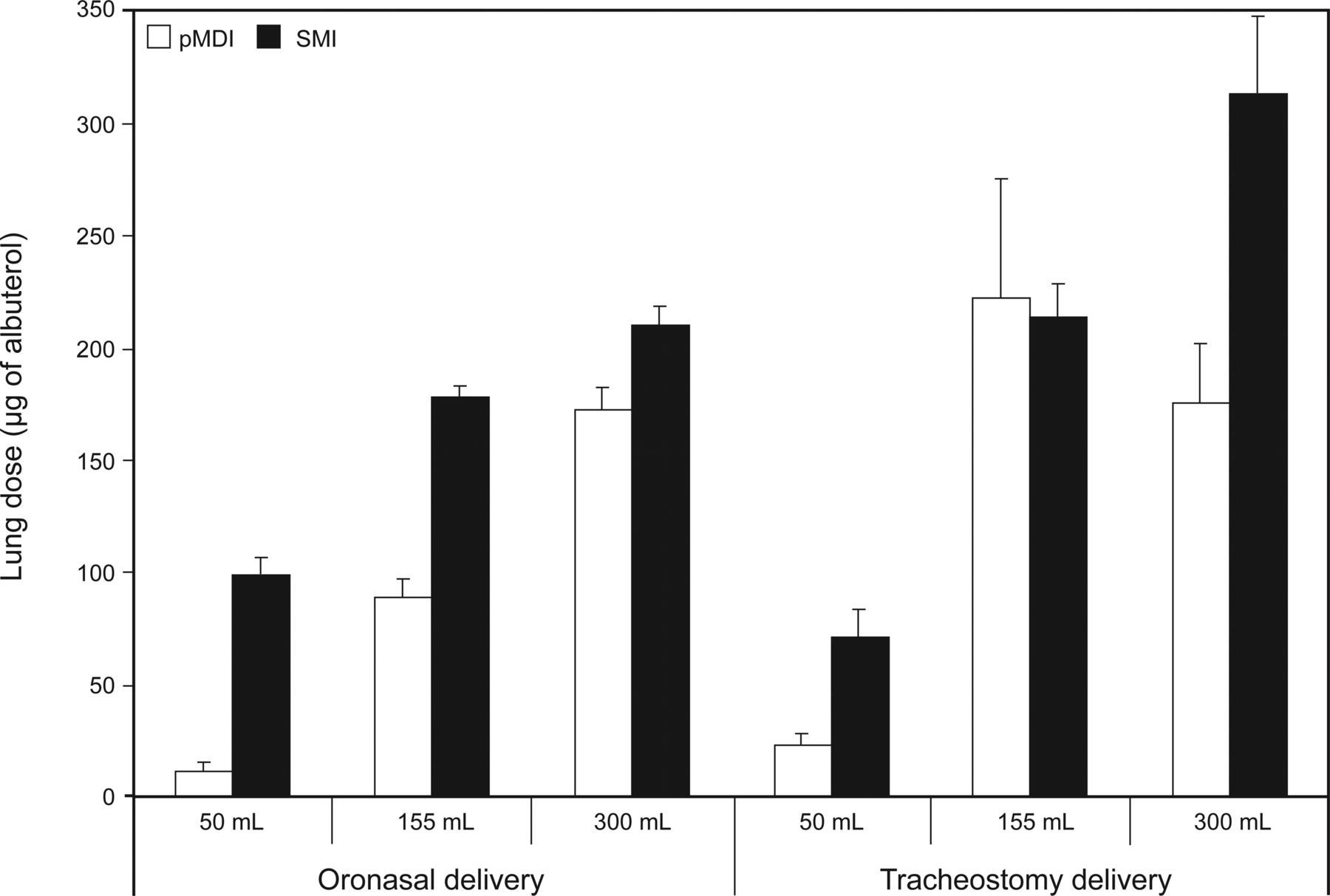
Lung dose achieved with a metallic valved-holding chamber with pressurized metered-dose inhaler (pMDI) and soft mist inhaler (SMI) with different breathing patterns during oronasal and tracheostomy albuterol delivery.
Comparison Between pMDI and SMI
When albuterol with a metallic VHC was delivered through the oronasal route, the SMI achieved higher lung doses than the pMDI. The difference was statistically significant for all breathing patterns but was the largest for the 50-mL tidal volume (8.5-fold).
When albuterol with a metallic VHC was delivered through the tracheostomy tube, the SMI achieved higher lung doses than the pMDI for the breathing patterns with a 50-mL (3-fold difference) and 300-mL (1.8-fold difference) tidal volume. However, no difference was noted for the breathing pattern with a tidal volume of 155 mL (P = .69).
Comparison Between Oronasal and Tracheostomy Delivery
When the delivery route of albuterol administered with pMDI and metallic VHC was changed from tracheostomy to oronasal, lung dose increased for the breathing patterns with 50- and 155-mL tidal volumes but not for the breathing patterns with a tidal volume of 300 mL (P = .83). The tracheostomy/oronasal lung dose ratio for the pMDI with metallic VHC was 2, 2.5, and 1 for breathing patterns with tidal volumes of 50, 155, and 300 mL, respectively.
When the delivery route of albuterol administered with SMI and metallic VHC was changed from tracheostomy to oronasal, lung dose decreased for the breathing pattern with tidal volume of 50 mL but increased for the other. The tracheostomy/oronasal lung dose ratio for the SMI with metallic VHC was 0.7, 1.2, and 1.5 for breathing patterns with tidal volumes of 50, 155, and 300 mL, respectively.
Breathing Patterns
When using a pMDI with a metallic VHC through the oronasal route, the lung dose was higher for higher tidal volumes (P = .001). During delivery through tracheostomy, the breathing pattern with a 50-mL tidal volume was lower than others (P < .001). The lung dose achieved with breathing patterns with tidal volumes of 155 and 300 mL were similar (P = .059). When using an SMI with a metallic VHC through the oronasal and tracheostomy routes, the lung dose increased with higher tidal volumes (P < .001).
Amount of Drug Deposited in the Tracheostomy Tube
The amount of albuterol retained in the tracheostomy tube when using a pMDI and Vortex was 0.7, 3, and 12.1% of the nominal dose for breathing patterns with tidal volumes of 50, 155, and 300 mL, respectively. The tidal volume of 300 mL had the highest drug retention (P < .001).
The amount of albuterol retained in the tracheostomy tube when using an SMI and metallic VHC increased with higher tidal volumes (P < .001) and was 1.3, 16.1, and 36.5% of the nominal dose for breathing patterns with tidal volumes of 50, 155, and 300 mL, respectively. The SMI had a higher intra-tracheostomy deposition than the pMDI for all breathing patterns (P = .009, P = .001, and P = .004 for the breathing patterns with a tidal volume of 50, 155, and 300 mL respectively.
Discussion
We found that in general, albuterol delivery via an oronasal and tracheostomy route using a metallic VHC resulted in a higher lung dose with an SMI than with a pMDI. We also found that in general, the lung dose was higher for tracheostomy than for oronasal delivery for both pMDI and SMI devices used with a metallic VHC. Finally, deposition in the tracheostomy tube was higher for SMI than pMDI when both were used with a metallic VHC.
The finding that the use of an SMI provided a larger lung dose than the pMDI is consistent with the characteristics of the aerosols produced by both inhalers.5 The SMI produces an aerosol that is 10 times slower and is ejected for a 3-fold greater duration than the one produced by the pMDI.5 We speculate that the difference in magnitude noted among different tidal volumes could be explained by the relative influence of difference in speed and duration of the aerosols. We speculate that a slower aerosol will result in less impaction and will be mainly responsible for the increase in lung dose found with tidal volumes of 155 and 300 mL. We speculate that the higher magnitude of the increase in lung dose noted with the 50-mL tidal volume is heavily influenced by the duration of aerosol because it is only one quarter of the volume of the VHC compared with 75 and 100% of the volume for the tidal volumes of 155 and 300 mL, respectively. Our findings are also consistent with adult studies comparing lung deposition between a pMDI and an SMI but without the use of a VHC.13 Wachtel et al14 reported a lung dose of 33% for an SMI using a different airway model but with a similar VHC (Vortex). The difference with our lung dose (21.1%) could be due to the fact that we used a different airway model and breathing pattern. In another study, Amirav et al15 reported a 30 and 60% lung dose in a 20-month-old model using breathing patterns with a tidal volume of 80 and 120 mL, respectively. They also reported a 20 and 40% lung dose in a 14-month-old model using breathing patterns with a tidal volume of 50 and 80 mL, respectively.15 The same group reported a 4.2% lung deposition in a group of 9-month-old infants using a VHC and Respimat.9 Their in vitro model overestimated lung deposition by a 4-fold difference.9,15 Our model yielded a 9% deposition for the breathing pattern with a tidal volume of 155 mL. Again, differences in airway models, breathing patterns, VHCs, and masks could potentially explain these differences.
The finding that during oronasal delivery of pMDI lung dose increased with increasing tidal volumes is consistent with previous reports using anatomically correct and non-anatomically correct models.11,12,16 During tracheostomy delivery, lung dose was lower for the 50-mL tidal volume but was similar between the breathing patterns with 155 and 300 mL. This finding is in agreement and disagreement with previous reports.11,12 Cooper et al,12 using the same model and 2 VHCs made of a nonelectrostatic polymer, reported a direct correlation between tidal volume and lung dose for one (Aerotrach Plus) and a lower lung dose for the 50-mL tidal volume than for other tidal volumes (155 and 300 mL) with the other VHC (Aerochamber Mini). Berlinski et al,11 using a non-anatomically correct model, reported similar findings for the same tracheostomy size and similar breathing patterns (tidal volumes of 80, 155, and 310 mL) for the Aerochamber Mini. However, lung dose was similar among all breathing patterns for the Aerotrach. These differences could be explained in part by the characteristics of the models used. Whereas this study and the one by Cooper et al12 used a 2-compartment model with bidirectional flow, the study by Berlinski et al11 used a 2-compartment model with unidirectional flow. Their model placed a one-way valve at the vocal cord level that opened during expiration in contrast to the bidirectional flow model that allowed air flow through the vocal cords during inspiration and expiration.11,12 These findings underscore the fact that data for a specific device should not be extrapolated to others and that choice of model could influence results.
Consistent with a previous report,12 the amount of drug deposited in the tube increased with increasing tidal volumes. This was true for both the SMI and the pMDI, with the latter being lower than previously reported.12 However, this was in contrast to findings by Berlinski et al11 that reported for the pMDI similar deposition for different tidal volumes. The difference could be explained in part by the difference in model (unidirectional vs bidirectional flow) and pMDI formulation (Proair HFA vs Ventolin HFA).11,17 An unexpected finding was that deposition in the tracheostomy tube was higher with the SMI than with the pMDI. We hypothesized that the lower speed would have resulted in lower impaction in the tube. We speculate that the longer duration of the aerosol of the SMI allowed more time to deposit in the tube.
This study adds to the body of knowledge provided by previously reported data using the same model and with experiments done by the same operator and allows a direct comparison with fewer biases than are usually found.12 During oronasal delivery of pMDI with tidal volumes of 50 and 155 mL, the Aerochamber Mini was better than the others and the Aerotrach VHC was better than the Vortex VHC. However, when the large tidal volume (300 mL) was used, lung dose was higher for the Aerochamber VHC followed by the Vortex VHC and then the Aerochamber Mini VHC. During tracheostomy delivery of pMDI, the Vortex VHC performed similarly to the Aerotrach VHC for the lower tidal volume (50 mL), and both had a lower lung dose than the Aerochamber Mini VHC. However, when larger tidal volumes were used (155 and 300 mL), the Vortex VHC outperformed the other 2. These data suggest the existence of a complex relationship between lung dose obtained with a pMDI, the breathing pattern, and the type of VHC used.
Our findings have several clinical implications: (1) pMDI and SMI are not interchangeable, and the magnitude of the difference in drug delivery varies significantly with different tidal volumes; and 2) recommendations based on data obtained with a specific device/formulation should not be assumed to be equal to other combinations until proven. In the absence of dosing equivalency, clinicians should consider starting at a lower dose and titrating to effect when switching from a less efficient to a more efficient delivery system. Given the number of variables that play a role in drug delivery (VHCs, masks, aerosol generators, breathing patterns, etc), practitioners should consider utilizing products that are cost-efficient and have been studied in conditions similar to the ones in which they will be used.
The major limitation of this study is its in vitro nature, which does not provide the biological variability that occurs during real life. These methods tend to overestimate lung dose, especially the fraction that is smaller than the 0.5 μm that would have been exhaled but is trapped in the filter instead. Nonetheless, these are well-established methods in aerosol research. The findings of our study should not be extrapolated to other devices, tracheostomy size tubes, and breathing patterns. Another limitation is that we did not measure particle size of the aerosols that left the tip of the tracheostomy tube.
Conclusions
The experiments reported in this study should caution practitioners from interchangeably using pMDI and SMI inhalers. Our findings underscore that data obtained with one device/formulation combination cannot be extrapolated to others. Whereas a dose increase might be necessary for the patients with low tidal volume when changing the delivery route of an SMI from an oronasal to a tracheostomy delivery route, the opposite action should be taken for larger tidal volumes and when an SMI is used. Animal and human studies are needed to help improve in vitro/in vivo correlation.
Footnotes
- Correspondence: Ariel Berlinski MD, Pediatric Pulmonology Section, 1 Children's Way, Slot 512-17, Little Rock, AR 72202. E-mail: BerlinskiAriel{at}uams.edu.
Ms Cooper was supported by a University of Arkansas for Medical Sciences College of Pharmacy Summer Research Fellowship. The Pediatric Aerosol Research Laboratory at Arkansas Children's Hospital Research Institute was partially established by and receives partial support from the George Endowment for Asthma. Dr Berlinski has disclosed relationships with Vertex, AbbVie, Aptalis Pharma, Genentech, Janssen Research and Development, Gilead, Teva, Philips, Novartis, the National Institutes of Health, and the Therapeutic Development Network. Ms Cooper has disclosed no conflicts of interest.
- Copyright © 2016 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}