

Abstract
BACKGROUND: The lung diffusion capacity (DLCO) determined by the single-breath technique greatly helps in the differential diagnosis and classification of severity of common lung diseases. However, widespread use of single-breath DLCO tests in Latin America has been limited, in part, by the lack of appropriate reference values. Our objective was to derive robust reference equations for single-breath DLCO from healthy Hispanic adults, using the most recent guidelines and taking into account altitude above sea level and hemoglobin.
METHODS: We recruited healthy adults from Caracas (690 m), Santiago (650 m), Mexico City (2,240 m), and Bogota (2,640 m). DLCO testing was completed using an instrument that exceeds American Thoracic Society/European Respiratory Society 2005 guidelines for spirometry and single-breath DLCO and provided centralized training and a quality assurance program.
RESULTS: We included 480 healthy Hispanic adults (58.3% women) with a mean age of 46 y (range 22–83 y). Their mean ± SD single-breath DLCO was 30.4 ± 9.2 mL/min/mm Hg. Results as a percentage of predicted by Crapo's reference values (the closest to obtained values) were 83 ± 10% (Caracas), 91 ± 10% (Santiago), 104 ± 17% (Mexico City), and 118 ± 19% (Bogota), and current suggested adjustments by hemoglobin or altitude did not correct differences, especially in Santiago and Caracas.
CONCLUSIONS: We recommend these new single-breath DLCO reference equations to predict single-breath DLCO in Latin America performed with current instruments and procedures and including as a predictor altitude above sea level.
Introduction
The combination of spirometry and the lung diffusion capacity (DLCO) determined by single-breath technique tests is widely available in pulmonary function testing (PFT) laboratories, since it assists in the differential diagnosis of patients with dyspnea, assesses the severity of both obstructive and restrictive types of lung disease, and provides objective measurements of treatment efficacy.1 The guidelines for PFT were updated by the American Thoracic Society (ATS) and European Respiratory Society (ERS) in 20052 and are widely recognized as standards of practice by other pulmonary subspecialty societies worldwide.
The selection of appropriate reference values is crucial to adequately interpret PFT results, to ascertain the correct classification of functional patterns, and to more accurately estimate disease severity. However, the 2005 ATS/ERS PFT interpretation guidelines2 did not recommend a single set of single-breath DLCO reference equations. In fact, few reference value studies have been reported since 2000.3–6
Most PFT laboratories in Latin America currently use single-breath DLCO reference equations from studies of non-Hispanic adults in Europe or the United States,7–9 but these give substantially different percent-of-predicted single-breath DLCO values for many patients, increasing misclassification rates.
The aim of this study was to generate robust single-breath DLCO reference equations from a group of healthy Hispanic adults from 4 large Latin American cities with the rationale that testing with standardized methods would improve current suggested adjustments by hemoglobin and altitude. Some of the results have been reported previously in the form of an abstract.10
QUICK LOOK
Current knowledge
The lung diffusion capacity (DLCO) determined by the single-breath technique is commonly essential in the process of diagnosis and evaluation of severity of chronic lung diseases. This testing should be performed under the current guidelines (American Thoracic Society/European Respiratory Society 2005), widely recognized as standards of practice. However, widespread use of single-breath DLCO tests in Latin America has been limited, in part, by the lack of appropriate reference values.
What this paper contributes to our knowledge
This is a multinational study regarding reference values of DLCO obtained in an adult population from Latin America at different altitudes. The main results were obtained using current guidelines, modern instruments, and good test quality, giving comparable results across the 4 participant cities and with substantial advantages over previous studies. Reference equations properly adjust for age, height, sex, altitude up to 2,600 m, and hemoglobin.
Methods
Subjects
Previous studies showed that adults living at high altitude have higher single-breath DLCO values,11 so we chose cities located at different altitudes above sea level for our study, including Santiago de Chile (650 m), Caracas (960 m), Mexico City (2,240 m), and Bogota (2,640 m). The study was approved by the ethics committees of each institution (see the supplementary materials at http://www.rcjournal.com), and participants gave their written informed consent. We adopted standardized instrumentation, training, quality control, and systematic review of results as described previously.12 PFT technologists for this study underwent a standardized, 1-week training in Mexico City on proper use of equipment, quality assurance, and practical testing. Men and women ≥25 y old were recruited by announcements in all institutions and related hospitals that invited students, employees, and the relatives of patients from a variety of socioeconomic levels to participate. Similar announcements were also placed in the vicinity of the hospitals. We used a brief interview and a standardized questionnaire13 to exclude those who reported smoking >400 cigarettes in their lifetime; who had undergone previous upper abdominal or thoracic surgery; who had received a physician diagnosis of diabetes mellitus, respiratory disease, or cardiovascular disease; or who had recently experienced respiratory symptoms. We also excluded pregnant women, those with a heart rate >110 beats/min, and those with surgery of the eyes or ears in the 3 months before testing. Data from subjects who were unable to perform acceptable single-breath DLCO test were not included in the final analysis.
Testing
All study sites used the EasyOnePro (firmware V04b, ndd Medical Technologies, Zurich, Switzerland), a small portable instrument for spirometry and single-breath DLCO tests. The test gas was 21% oxygen (not adjusted for altitude), 10% helium, 0.3% carbon monoxide, and the remaining gas was nitrogen. Unacceptable maneuvers were not used for data analysis. We used standard venipuncture techniques to draw blood for hemoglobin analysis. Test methods closely followed 2005 ATS/ERS guidelines,14 and the quality assurance program followed its recommendations and included biological controls in all sites and simulators at the beginning of the study in Mexico City and Bogota, the cities with highest altitude, as described with more detail in the supplementary material.
Statistical Analyses
At the end of the study, averages and SD values or means and intervals were used to describe the variables according to their distribution. Reference equations for single-breath DLCO, alveolar volume (VA) (single-breath total lung capacity), and single-breath DLCO/VA (dependent variables) were generated separately for men and women, using robust multiple regression models, including as independent variables linear and quadratic terms for weight, height, age, and altitude above sea level, with and without measured hemoglobin (since the latter was often not available at the time of testing). Squared predictors were tested as well as interaction between relevant variables. The transformed variables remained in the final equation only if they significantly improved the r2 of the equation. We estimated directly the lower limit of normal (5th percentile) separately for men and women, utilizing the semi-parametric quantile regression,15 including predictors utilized for prediction of mean single-breath DLCO. We also estimated the residual volume as VA-FVC and generated predicting equations for residual volume/single-breath total lung capacity.
Results
We recruited 480 healthy subjects (58.3% women) who fulfilled the selection criteria and completed tests of good quality. Most non-eligible individuals were current or previous smokers or were discovered in a brief interview to have respiratory symptoms or asthma. After testing was done, we excluded 11 individuals because of body mass index >35 kg/m2, 5 because of air flow obstruction found in response to bronchodilator and atopy suggestive of asthma, 3 because of diabetes, 3 because of hypertension, and 4 because of claustrophobia that would not allow them to enter the body box used for additional testing.
The main characteristics of the participants by city are depicted in Table 1. The mean age was 46 y (range 22–83 y). Age distribution from 25 to 65 y was similar in the 4 cities, but the Caracas center recruited only a few adults >65 y old. On average, recruited individuals were 162 ± 10 cm tall and had a weight of 66.8 ± 11.5 kg (only 4.2% had a body mass index >30 kg/m2), a single-breath DLCO of 30.4 ± 9.3 mL/min/mm Hg, and a vital capacity of 3.9 ±1.0 L. The mean difference between the 2 acceptable single-breath DLCO tests was 0.98 ± 0.76 mL/min/mm Hg.
Characteristics of Healthy Hispanic Adult Study Subjects
From all individuals, 455 (94.8%) had 2 acceptable maneuvers, whereas 7 had 1, and 18 had none, and single-breath DLCO repeatability was better than 3 units for subjects. The intratest coefficient of variability for single-breath DLCO was 2.45 ± 1.99% (SD), and that for single-breath DLCO/VA was 3.25 ± 3.7%. The mean intratest coefficient of variability for VA in the studied population was 2.79 ± 3.1% for the 2 selected maneuvers. The coefficient of variability was consistently higher for single-breath DLCO/VA and for VA than for single-breath DLCO. The number of DLCO maneuvers performed was 2 for 76% of participants, 3 for 19%, 4 for 3%, and 5 for 2%.
Independent predictors of a higher single-breath DLCO included male sex, height, altitude, and hemoglobin (see Figs. S1 and S2 in the supplementary material), whereas single-breath DLCO declined with aging (Figs. 1 and 2). Hemoglobin was available for 169 men and 250 women (87% of all subjects). Adding squared age, height, or altitude terms or interaction terms to the equation increased r2 significantly in some models. Parsimonious reference equations are given in Table 2 with and without hemoglobin. Similar prediction equations using only linear terms are shown in Table 3, with slightly less variability explained by the models (lower r2).

Diffusing capacity of the lung (DLCO) determined by the single-breath technique as a function of age for women (A) and men (B). Variability decreased with age for women. Average values (lines) were obtained by locally weighted scatter-plot smoothing.
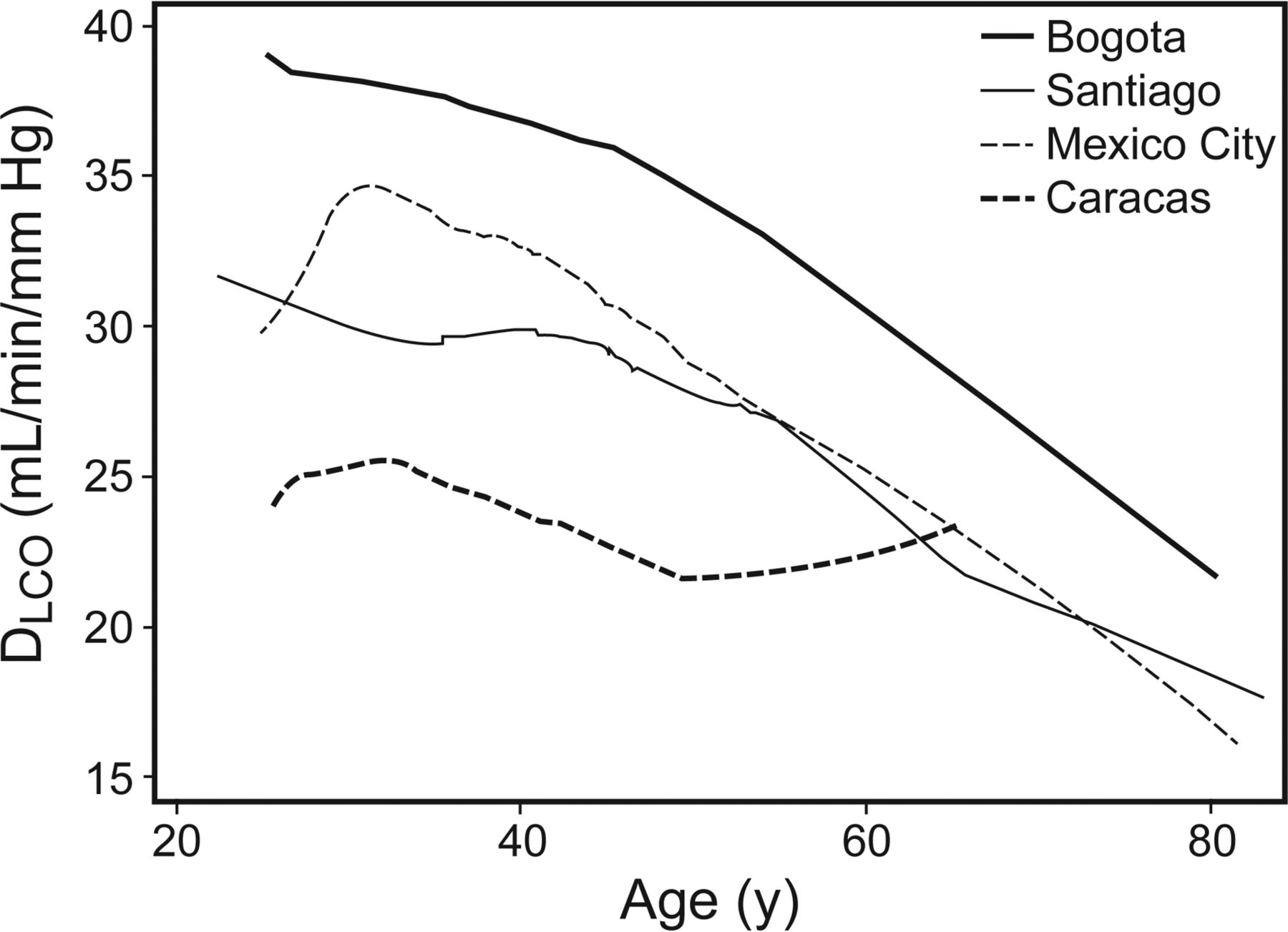
Diffusing capacity of the lung (DLCO) determined by the single-breath technique as a function of age. Data smoothing was done using locally weighted scatter-plot smoothing.
Reference Equations for Diffusing Capacity of the Lung Determined by the Single-Breath Technique
Parsimonious Diffusing Capacity of the Lung Determined by the Single-Breath Technique Reference Equations Using Only Linear Terms
Variance of single-breath DLCO increased with altitude or barometric pressure with significant Breusch-Pagan and Cook/Weisberg heteroskedasticity tests and was eliminated if regression was done with log single-breath DLCO instead of single-breath DLCO, but prediction of single-breath DLCO did not improve over the untransformed term. The Breach-Pagan test was also not significant if altitude was eliminated from the equation, but r2 decreased significantly (see Table 2). Using the daily barometric pressure available from the instrument (or mean barometric pressure for the city) did not increase the r2 when compared with use of the mean altitude above sea level (data not shown). The concordance correlation coefficient between the internally predicting equation using hemoglobin and altitude was 0.89 (95% CI 0.87–0.91) and was 0.88 for the equation without hemoglobin (95% CI 0.86–0.90) but was only 0.77 (95% 0.74–0.81) for the equation without altitude or hemoglobin (based only on sex, age, and height).
The healthy adults in this study had single-breath DLCO values on average above (5–17%; see Table 1) those of previous studies,8,9,16 with mean values closest to the study of Crapo and Morris,7 done at 1,420 m above sea level and using an FIO2 of 0.25, simulating sea level (see Table 1 and Fig. 3). We observed heterogeneous results for the different cities, with an overall concordance correlation coefficient rho = 0.69 (95% CI 0.65–0.73) between predicted and observed results. Adjusting single-breath DLCO by hemoglobin and altitude14,17 improved the prediction in Mexico and Bogota, but overestimation remained for Santiago and Caracas: overall rho = 0.75 (95% CI 0.71–0.78) adjusting only by hemoglobin and 0.81 (95% CI 0.78–0.84) adjusting by hemoglobin and altitude (see Fig. 3). The age coefficient from the study by Crapo and Morris7 did not apply well for our data, as shown by a positive slope of single-breath percent-of-predicted DLCO as a function of age in Figure 3. In the online supplementary material, we provide predicting equations for the single-breath DLCO/VA (KCO, e-Table 1), single-breath total lung capacity (VA, e-Table 2), and residual volume/single-breath total lung capacity (e-Table 3) from the same participants.
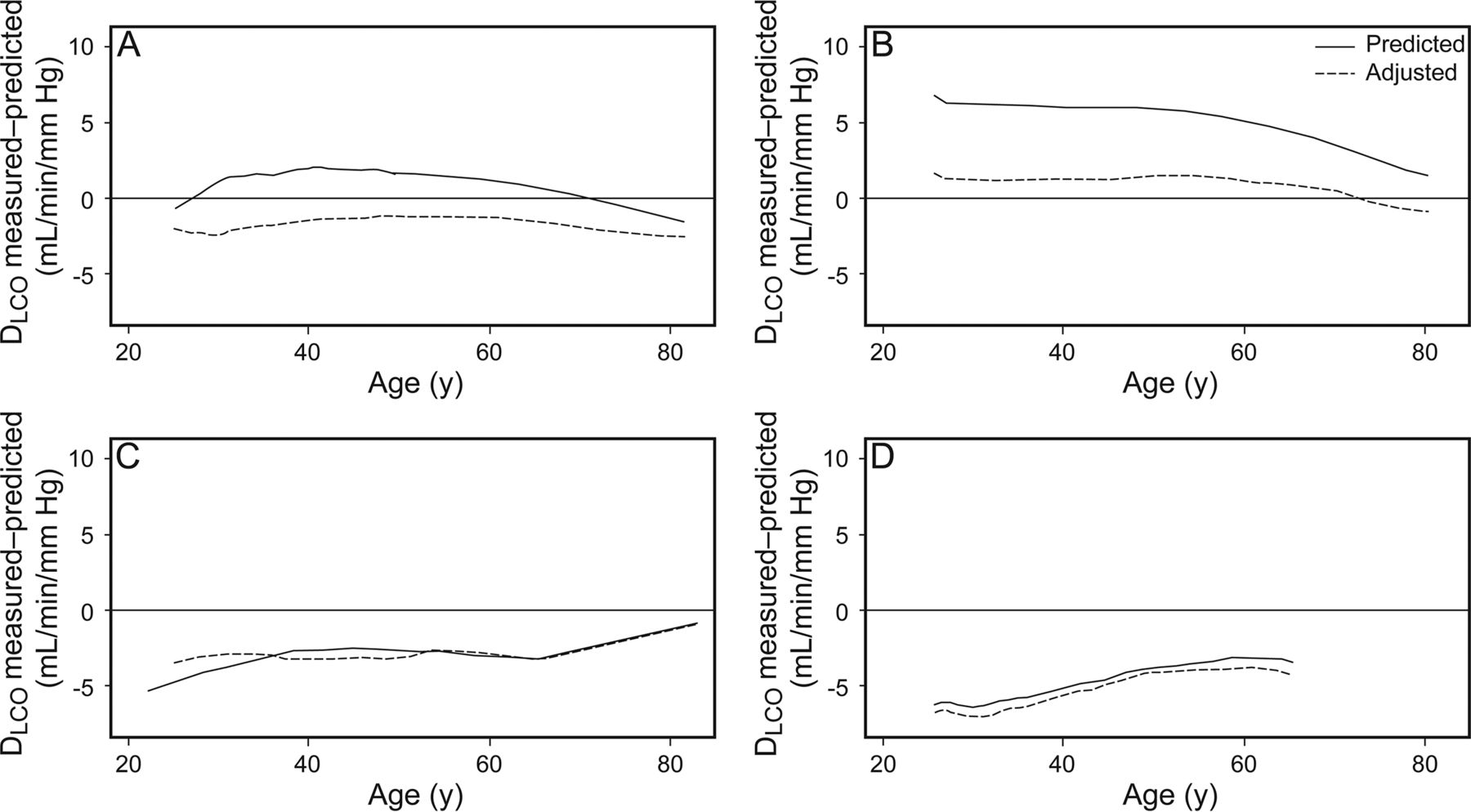
Predicted diffusing capacity of the lung (DLCO) determined by the single-breath technique for the healthy Hispanic study subjects in Mexico City (A), Bogota (B), Santiago (C), and Caracas (D) (using the reference equations of Crapo and Morris7). Dashed lines show adjustment for hemoglobin and altitude. Graphs were plotted after smoothing of the residuals over age.
Discussion
Single-breath DLCO increased with altitude of residence, with body size (height or weight), and with hemoglobin and decreased with age, as described previously in various studies done at different times with heterogeneous equipment and procedures.3–6,8–10,14,16,18 This study was done with current equipment and procedures and good test quality, giving comparable results across several cities of Latin America with substantial advantages over previous studies. Reference equations in use were obtained many years ago with varied equipment, procedures, and populations and according to our data give results with systematic bias for single-breath DLCO and also with coefficients that do not adjust properly to changes with age, altitude, and height. Relevant additions from our study were: 1) comparison across different altitudes, and 2) inclusion of hemoglobin in the majority of the subjects. These allow simultaneous adjustments for independent variables indispensable in countries with significant populations residing at moderate or high altitudes. Current practice was to adjust obtained values for single-breath DLCO by altitude and hemoglobin, with equations proceeding from different studies. With our reference values, altitude and hemoglobin can be taken into account simultaneously, but the most relevant variable was altitude, and once it was accounted for, the additional contribution of hemoglobin was moderate in the studied population, although statistically significant.
Limitations of the study included the following. Participant selection was not population-based (but nevertheless age distribution was adequate, including individuals of varying socioeconomic strata). Children were not included, and older adults (age >65) were 13% (n = 64). More individuals were contributed by Mexico City and Bogota, and no city at sea level was included. Carboxyhemoglobin was not measured, but smokers were excluded. The usual level of carboxyhemoglobin in Mexico City was about 1.5% in the 1980s,19 and average values continue the same (unpublished data from the PFT laboratory).
On the other hand, the uniform equipment, training, and methods and the varied altitude of residence provide, from our point of view, significant advantages over current reference values. As done recently for spirometry by the Global Lung Function Initiative Group, it would be very useful to include younger individuals, including children during growth and development, to obtain continuous single-breath DLCO equations from infancy to old age,20 so we have shared our DLCO data with the Global Lung Function Initiative Group.
Poverty is associated with low lung volumes for a given height,21,22 and in developing countries, socio-economic status is often associated with ethnicity. Differences in the ratio of leg length to height can explain the majority of these differences in lung volumes, but we did not measure sitting height or an index of socioeconomic status or ethnicity in our study subjects, which may have varied between study sites. Socio-economic status has rapidly improved during the past few decades in the urban areas of developing countries, leading to increases in lung volumes from one birth cohort to the next. These increases in lung volumes are probably associated with increases in single-breath DLCO and VA, but this has not yet been confirmed.
Single-breath DLCO is a clinically important test underused in many parts of the world. Several factors have limited more widespread use: the cost of the equipment and its maintenance, the difficulty and cost of obtaining certified calibrating gas mixtures, a quality control considerably more demanding than spirometry, and the lack of appropriate reference values with adjustments for altitude and hemoglobin. The size and cost of single-breath DLCO instruments has diminished during the past decade.
Conclusions
We report reference values for single-breath DLCO obtained in an adult population at different altitudes above sea level using modern guidelines and instruments. We suggest that these reference equations offer a significant advantage over existent equations when testing Hispanic patients at a high altitude or with hemoglobin outside of the normal range.
Acknowledgments
We thank additional collaborators in the single-breath DLCO study group. Maria Montes de Oca (Caracas) participated in the final version of the protocol. Robert Jensen participated in the central PFT training. All tests and calibration checks were performed by Mónica Silva (Mexico), Patricia Sandoval (Santiago), Margarita Barrero, Maria Isabel Quintero (Bogota), and Jonatan Pereira (Caracas), who also served as biological controls. Monica Velazquez recruited normal subjects in Mexico City, and Elisa Sanchez-Gallen and Monica Silva received the tests done at all sites and verified quality. Paul L Enright MD reviewed the manuscript and gave thoughtful suggestions.
Footnotes
- Correspondence: Juan Carlos Vázquez-García MD MSc, Departamento de Fisiología Respiratoria, Instituto Nacional de Enfermedades Respiratorias “Ismael Cosío Villegas”, Calzada de Tlalpan 4502, Colonia Sección XVI, C.P. 14080, Tlalpan, Distrito Federal, Mexico. E-mail: drjcvazquez{at}gmail.com.
This study was supported by each participant institution. ndd Medical provided equipment for pulmonary function testing, but there was no participation in the design, analysis, or writing of the paper. The authors have disclosed no conflicts of interest.
Dr Vázquez-García presented a version of this paper at the IX Congress, Asociación Latinoamericana de Tórax (ALAT), held July 31 to August 2, 2014, in Medellin, Colombia.10
Supplementary material related to this paper is available at http://www.rcjournal.com.
- Copyright © 2016 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}