

Abstract
BACKGROUND: A 2005 consensus conference led by the National Association for Medical Direction of Respiratory Care (NAMDRC) defined prolonged mechanical ventilation (PMV) for adults as invasive and/or noninvasive mechanical ventilation (NIV) for ≥ 21 consecutive days for ≥ 6 h/d. In children, no such consensus definition exists. This results in substantial variability in definitional criteria, making study of the impact and outcomes of PMV across and within settings problematic. The objective of this work was to identify how PMV for children and neonates is described in the literature and to outline pediatric/neonatal considerations related to PMV, with the goal of proposing a pediatric/neonatal adaptation to the NAMDRC definition.
METHODS: We searched electronic databases for studies describing PMV in children. We extracted definitional criteria and developed recommendations based on the literature review and our clinical experience.
RESULTS: Of the 416 citations obtained, 87 met inclusion criteria, totaling 34,255 subjects. Identified criteria for the pediatric PMV definition included: number of consecutive days of mechanical ventilation (ranging from 6 h to 3 months), inclusion of NIV, time spent off the ventilator during weaning (considered as same ventilation episode), and importance of chronological age (term neonates) and postmenstrual age for preterm neonates. We considered high-flow nasal cannula; however, we determined that its current role as a weaning adjunct is unclear.
CONCLUSIONS: Therefore, we developed the following recommendations for the pediatric PMV definition: ≥ 21 consecutive days (after 37 weeks postmenstrual age) of ventilation for ≥ 6 h/d considering invasive ventilation and NIV and including short interruptions (< 48 h) of ventilation during the weaning process as the same episode of ventilation. We propose a definition of pediatric PMV that incorporates the number of consecutive days of mechanical ventilation while taking into account use of NIV and lung maturity and including short interruptions during the weaning process.
Introduction
Mechanical ventilation is a common treatment in intensive care, whether for neonates, children, or adults. Independent of the underlying disease, this supportive treatment is associated with many complications that may prolong its duration, such as ventilator-associated lung injury and pneumonia. Health-care costs associated with intensive care are projected to increase as a result of more patients requiring prolonged mechanical ventilation (PMV).1 In 2005, a consensus conference led by the National Association for Medical Direction of Respiratory Care (NAMDRC) defined PMV for adults as mechanical ventilation for ≥ 21 consecutive days for ≥ 6 h/d of invasive (via endotracheal tube or tracheostomy) and/or noninvasive (facial/nasal interface) methods of delivery.2 In children, 10 years after the published NAMDRC definition, no such consensus definition exists, making it difficult to interpret study results describing a PMV population and to determine the impact of PMV across and within settings.
The absence of a pediatric PMV definition has resulted in: (1) substantial variability in duration of ventilation described as PMV in the published literature, with duration generally ranging from 2–7 d3–5 to 21–28 d6–9 (these 2 groups may be derived from the perspective of pediatric intensivists who want to differentiate between patients who are able to be extubated quickly and longer-term ICU patients and of pediatric pulmonologists who may be making decisions about home mechanical ventilation support; (2) lack of standardization regarding the inclusion of noninvasive ventilation (NIV) in the definition; (3) lack of standardization regarding the inclusion of times when the child is ventilator-free during weaning (ie, should these contribute to the number of days of consecutive ventilation?); and (4) no specific considerations for neonates in relation to when to commence counting the number of consecutive days that define PMV (ie, at which age, chronological or postmenstrual).7–10 Therefore, there is an urgent need to standardize the definition of PMV in children to: (1) describe the epidemiology of PMV; (2) assist clinicians with reprioritizing goals of care and the type of information to share with patients and their families10; and (3) identify effective interventions that will reduce the number of children requiring PMV. In this perspective, we propose an operational definition of pediatric PMV based on relevant literature and the authors' clinical experience.
QUICK LOOK
Current knowledge
The pediatric prolonged mechanical ventilation definition has not yet been defined and results in substantial variability in definitional criteria.
What this paper contributes to our knowledge
The authors reviewed literature and report that pediatric prolonged mechanical ventilation definition that can be used is defined by ≥21 consecutive days (after 37 weeks postmenstrual age) of ventilation for more than 6 hours per day including invasive and noninvasive ventilation duration and short interruptions (<48h) of ventilation during the weaning process as the same episode of ventilation.
Methods
In February 2016, we searched the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE (2000 to February 2016), and EMBASE (2000 to February 2016) using the following search terms: prolonged, protracted, chronic, sustained, increased length, or long term mechanical ventilation. Criteria were determined a priori, and studies were eligible for inclusion if they included mechanically ventilated (invasive and NIV) children or neonates, including mixed adult and pediatric cohorts. Exclusion criteria included: case reports, case series of < 10 patients, commentary or editorials, and non-peer-reviewed articles. Articles written in a language other than English were not included. We extracted the definitional criteria used to identify the study cohort as PMV and any rationale reported for the definitional criteria used.
Results and Discussion
Of the 416 citations obtained, 87 met inclusion criteria (see the supplementary materials at http://www.rcjournal.com), totaling 34,255 subjects. Criteria used to define PMV were heterogeneous. Most of the articles (77%) defined PMV by a time criterion (ie, the duration of mechanical ventilation). However, there was no consensus as to the duration, with ranges varying from 6 h to 3 months (Fig. 1), with shorter duration (≥ 4 d) for surgical as opposed to medical patients (≥ 7 or 21 d, with 21 d used by the most recent studies). Other studies defined PMV as the presence of a tracheostomy, receiving ventilation at home, or receiving ventilation in a care center dedicated to chronic ventilation.
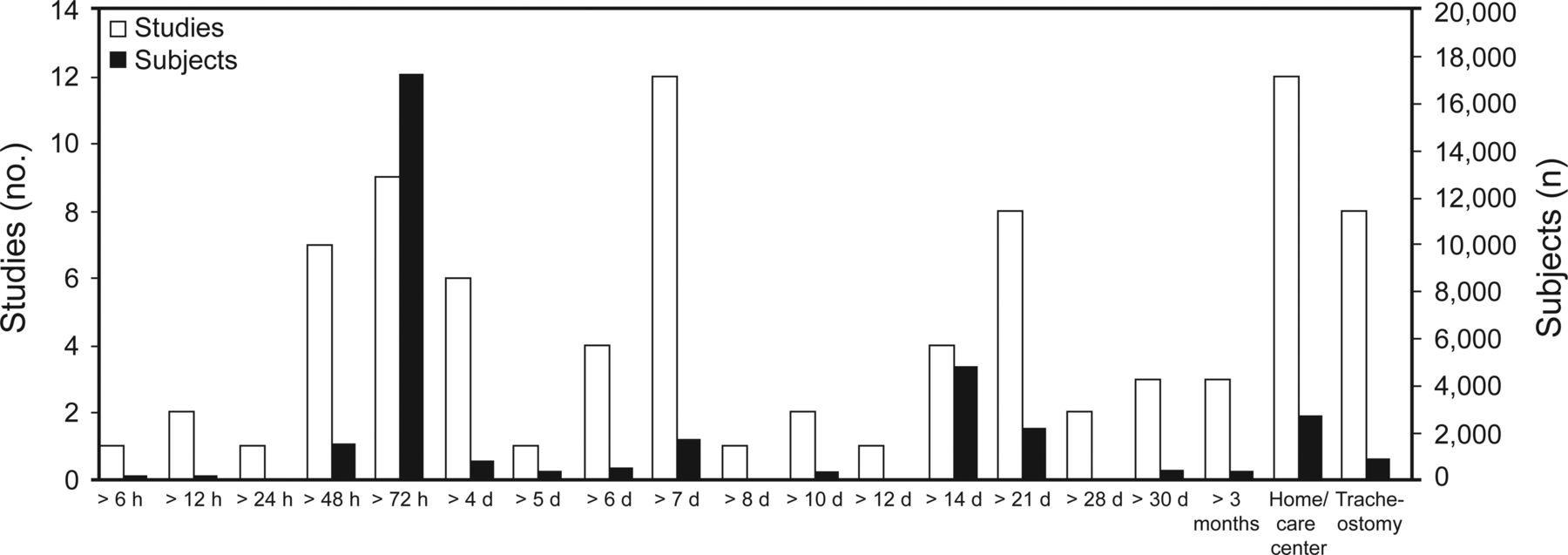
Duration of mechanical ventilation used to describe prolonged mechanical ventilation.
What Duration of Ventilation Should Be Used for PMV in Children?
In the NAMDRC PMV definition,2 21 consecutive days of mechanical ventilation was chosen for the adult population. Moreover, 21 d of ventilatory support has been used to define PMV in pediatric literature6,7 and may correspond to a turning point in the goals of care and type of weaning strategies to be used. Another advantage of this definition is that it offers objectivity, uniformity, and simplicity in terms of identifying the patient cohort.11 It corresponds to 2.5–3% of the population admitted to pediatric ICUs4,7 and represents a cohort of ventilated children who need rehabilitation strategies12 to promote weaning success and generally have a tracheotomy in place if they require invasive ventilation.13,14
How Should Short Episodes Off the Ventilator During Weaning Affect Establishment of PMV as Defined as 21 d of Consecutive Ventilation?
In our systematic review, few studies4,7 discussed the time off the ventilator during weaning. The NAMDRC PMV definition recommends this term be applied to patients receiving mechanical ventilation for ≥ 21 consecutive days for ≥ 6 h/d. However, if clinically indicated during these 21 d, weaning trials may occur with patients removed from any form of ventilatory support for up to 48 h before the establishment of weaning success.2 Patients who fail weaning will be returned to ventilatory support; however, this means that there has been an interruption in the number of consecutive days of mechanical ventilation. Therefore, we propose that in the case of weaning failure (defined as the need to recommence ventilation within 48 h before 21 d of ventilation), the days off ventilatory support should be included in the number of consecutive days of mechanical ventilation used to define pediatric PMV (see Fig. 2C). Infants with lung fragility (eg, bronchopulmonary dysplasia) may be at risk of more than one PMV episode in their life. For simplicity and uniformity reasons, we argue that the duration on and off the ventilator in the pediatric PMV definition should not be modulated by patient history and comorbidities.

Schematic representation of the proposed definition of prolonged mechanical ventilation (PMV) in neonates and children. A: Definition of PMV in neonates older than 37 weeks postmenstrual age. B: Different ventilation modes included in the PMV definition for children. C: Weaning failure < 48 h before 21 d counted as the same episode of respiratory support. The dotted vertical line shows the demarcation for PMV.
Should HFNC Be Included in the Number of Consecutive Days of Ventilatory Support to Establish Pediatric PMV?
The NAMDRC definition of adult PMV recommended that NIV be included in the number of consecutive days of mechanical ventilation, which we support for inclusion of pediatric PMV. However, the role of high-flow nasal cannula (HFNC) was not discussed, and at that time, few data were available on the physiological benefits of HFNC. At present, although there are limited and equivocal data suggesting that HFNC generates PEEP in adults, the evidence seems stronger in the pediatric population. In children, HFNC has been demonstrated to generate PEEP between 4 and 6 cm H2O with gas flows > 1.7 L/min/kg.15–18 In adults, HFNC generates a more unpredictable and less marked increase of PEEP that ranges from 1.5 to 5 cm H2O.19,20 HFNC decreases work of breathing in all age groups, whether it is measured by the electrical activity of the diaphragm,16 pressure rate product,21 or clinical scores or vital signs,15 even when no respiratory failure is present.16 The risk of intubation with HFNC is similar to NIV and significantly lower than using standard nasal cannula for neonates.22 Despite all of these data, inclusion of HFNC in the pediatric PMV definition is still a source of debate, and we advocate that this issue be discussed in a consensus conference.
When Defining Pediatric PMV Do We Use the Chronological Age or the Corrected Age for Neonates?
Preterm birth is defined by the World Health Organization as neonates born alive before 37 weeks of pregnancy. In neonates, age can be counted according to chronological age (age from birth) or using the corrected age defined as the chronological age reduced by the number of weeks born before 40 weeks of gestation; the term should be used only for children ≤ 3 y of age who were born preterm.23 Corrected age takes into account the maturation stage of the newborn that includes neurological, cardiovascular, and respiratory development and is considered important as a defining feature of other definitions. For example, bronchopulmonary dysplasia is diagnosed by the ongoing need of supplemental oxygen at different time points depending on the postmenstrual age (gestational age plus chronological age) and gestational age.24 Neonates born before 32 weeks gestational age may be diagnosed with bronchopulmonary dysplasia at 36 weeks postmenstrual age; those born at ≥ 32 weeks gestational age may be diagnosed using the chronological age from 4 to 8 weeks of life. We propose that the definition of pediatric PMV use chronological age when the cohort is homogeneous in terms of gestational age (eg, preterm neonates of 28 weeks gestational age). However, if a cohort includes premature and term neonates, the usual case in pediatric ICUs, the corrected age should be used to standardize the maturation stage of neonates. In such a heterogeneous cohort, the duration of ventilation before 37 weeks gestational age would not count toward the 21 consecutive days of ventilation. This means that the definition of pediatric PMV could not be applied before 40 weeks gestational age (see Fig. 2A). To illustrate this operational definition of pediatric PMV, here are 3 cases. (1) A 5-month-old girl who was born at 24 weeks (1-month-old corrected age or 44 weeks postmenstrual age) is transferred from the neonatal unit to the pediatric ICU (Fig. 2A). She was intubated from birth to 38 weeks postmenstrual age and was successfully weaned from invasive ventilation to NIV after a second hydrocortisone treatment at 40 weeks postmenstrual age. She is still receiving NIV 22 h on 24 (total of 5 months of mechanical ventilation; 7 weeks [44 − 37 weeks] if corrected age is used). (2) A 7-y-old boy was admitted to the ICU for pneumonia and required NIV support (Fig. 2B). On the second day, he was intubated for severe oxygenation failure. After 7 d of invasive mechanical ventilation, he was extubated. Two hours later, NIV was commenced due to increased work of breathing. He was subsequently reintubated because of severe CO2 retention. Ten days later, he was extubated to NIV and was successfully weaned from mechanical ventilation after 4 d (total 23 d of mechanical ventilation). (3) A 10-y-old boy who was intubated for Guillain-Barré syndrome was extubated on day 6 of mechanical ventilation (Fig. 2C). Thirty-six hours later, he was unable to protect his airway and required reintubation. Two weeks later, he was successfully extubated (total 22 d of mechanical ventilation).
Summary
We have highlighted important issues for consideration in the establishment of a pediatric PMV definition, namely determination of ≥ 21 consecutive days of mechanical ventilation (after 37 weeks postmenstrual age) of ventilation for ≥ 6 h each day considering invasive and NIV and including short interruptions (< 48 h) of ventilation during the weaning process as the same episode of ventilation (Table 1). To gain consensus and subsequent adoption of this definition, we plan to host a consensus conference with international experts representing pediatric intensive care, neonatal intensive care, and the pediatric pulmonology community. We will refine this definition by discussing the relevance to different patient populations (eg, chronic lung disease, neuromuscular disease, congenital heart defect) and debating the role of weaning adjuncts, such as HFNC, to come to a final consensus.
Proposed Criteria for Pediatric Prolonged Mechanical Ventilation
Footnotes
- Correspondence: Philippe Jouvet MD PhD, Soins Intensifs Pédiatriques, Hôpital Sainte-Justine, 3175 Chemin Côte Sainte-Catherine, Montréal, Québec H3T 1C5, Canada. E-mail: philippe.jouvet{at}umontreal.ca.
Dr Rose has disclosed a relationship with the Canadian Institutes of Health. Dr Jouvet has disclosed a relationship with the Health Research Agency of Quebec (FRQS). Dr Sauthier has disclosed no conflicts of interest.
Supplementary material related to this paper is available at http://www.rcjournal.com.
- Copyright © 2017 by Daedalus Enterprises









{kind=link}
{kind=link}